
Abstract
Substance use disorders commonly co-occur with one another and with other psychiatric disorders. They share common features including high impulsivity, negative affect, and lower executive function. We tested whether a common genetic factor undergirds liability to problematic alcohol use (PAU), problematic tobacco use (PTU), cannabis use disorder (CUD), and opioid use disorder (OUD) by applying genomic structural equation modelling to genome-wide association study summary statistics for individuals of European ancestry (Total N = 1,019,521; substance specific Ns range: 82,707-435,563), while adjusting for the genetics of substance use (Ns = 184,765-632,802). We also tested whether shared liability across SUDs is associated with behavioral constructs (risk taking, executive function, neuroticism; Ns = 328,339-427,037) and non-substance use psychopathology (psychotic, compulsive, and early neurodevelopmental disorders). Shared genetic liability to PAU, PTU, CUD, and OUD was characterized by a unidimensional addiction risk factor (termed The Addiction-Risk-Factor, independent of substance use. OUD and CUD demonstrated the largest loadings, while problematic tobacco use showed the lowest loading. The Addiction-Risk-Factor was associated with risk taking, neuroticism, executive function, and non-substance psychopathology, but retained specific variance before and after accounting for genetics of substance use. Thus, a common genetic factor partly explains susceptibility for alcohol, tobacco, cannabis, and opioid use disorder. The Addiction-Risk-Factor has a unique genetic architecture that is not shared with normative substance use or non-substance psychopathology, suggesting that addiction is not the linear combination of substance use and psychopathology.
INTRODUCTION
Substance use and use disorders (SUDs) represent large and growing public health problems that account for nearly 6% of global disease burden1. SUDs, both licit and illicit, commonly co-occur with each other and also with non-substance psychopathology; comorbidity is associated with increased symptom severity2 and worse outcomes (e.g., less responsivity to treatment, greater socioeconomic costs3). However, the etiology underlying shared risk across these disorders is poorly understood.
Shared Genetic Liability
According to twin studies, the moderate-large heritability (50-60%) of distinct SUDs (i.e., alcohol, nicotine, cannabis, and other illicit drugs) is partly attributable to a shared genetic vulnerability.4 Similarly, genetic correlations estimated from genome-wide association study (GWAS) data support a shared genetic vulnerability between SUDs (e.g., SNP-rG = .73 between alcohol use disorder and opioid use disorder),5 between SUDs and substance use (e.g., SNP-rG = .78 between problematic alcohol use and drinks per week),6 and between SUDs and psychopathology (e.g., SNP-rG = .33 between cannabis use disorder and major depressive disorder7). What remains unclear is the extent to which genetic liability across substance use disorders is shared with and distinct from that of substance use (but not dependence) and non-substance psychopathology, and what putative intermediate phenotypes may link shared genetic liability between SUDs and non-substance psychopathology.
Substance Use and Use Disorder
Substance use and SUDs have substantial genetic overlap; however, genetic mechanisms that relate to SUD liability beyond normative or frequently occurring substance use remain. For opioids8, alcohol9,10,11, and cannabis7, the use and use disorder dimensions show differing associations with psychopathology (e.g. schizophrenia) and life outcomes (e.g. educational attainment)7,8,12,13.
Substance use and Psychopathology
Recently, Lee and colleagues14 identified 3 broad clusters (psychotic, compulsive, and early neurodevelopmental) representing shared and distinct genetic liability to 8 non-substance psychiatric disorders. While there has been limited integration of substance use phenotypes into psychopathology models, polygenic liability to cross-diagnostic vulnerability is associated with general substance use and SUDs15. Further, emerging evidence suggests partial overlap: tobacco use shares variance with ADHD16, alcohol and cannabis dependence load with antisocial behavior17, and alcohol use and use disorder load together onto an Externalizing factor18. Collectively, these data suggest that substance use and use disorders share some common genetic liability with psychopathology.
Stage-Based Addiction Individual Differences and Substance Use Disorders
SUD vulnerability has been conceptualized within a 3-stage neurobiological model consisting of binge/intoxication, preoccupation/anticipation, and withdrawal/negative affect19. In this model, initial positive reinforcement is derived from stimulation of neural reward circuitry that drives impulsive behaviors in the context of under-developed tolerance. With continued use and progression towards SUD, the reinforcing properties of substances shift from positive to negative reinforcement; as use becomes compulsive, it functions to return the body to drug-present homeostasis and alleviate low mood, a predisposition to which is broadly indexed by neuroticism20. Following repeated drug-reward and drug-homeostasis pairings, cognitive preoccupation with the drug in expectation of reward/relief emerges in the context of impaired executive functioning21. While GWASs support genetic correlations between SUDs and risk-taking5,22, Executive Functioning23, and negative affect5,22, the extent to which common genetic liability across SUDs relates to these constructs has yet to be examined.
The Current Study
Given evidence of shared liability to SUDs and other forms of psychopathology, understanding the shared and unique genetic contributions to SUDs and how these relate to heritable proxies for stage-based addiction constructs, non-substance psychopathology, and substance use may generate etiologic insights that improve psychiatric nosology, prevention, and treatment. To this end, we first estimate the shared genetic structure across SUDs by applying genomic structural equation modelling (gSEM)24 to summary statistics generated by the largest GWAS of problematic alcohol use (PAU)22, problematic tobacco use (PTU)25,26, cannabis use disorder (CUD)7, and opioid use disorder (OUD)5. We name the shared variance across SUDs the Addiction-Risk-Factor. Second, we relate the Addiction-Risk-Factor to genetics of behavioral constructs representing proxies of the stage-based model of SUDs. We estimate the extent to which genetic liability to risk-taking, executive function, and neuroticism are related to The Addiction-Risk-Factor. Third, we examine whether The Addiction-Risk-Factor is associated with the 3 factors representing genetic liability to non-substance psychopathology14 (i.e., psychotic, compulsive, and neurodevelopment) and whether stage-based addiction constructs (i.e., risk-taking, executive function, neuroticism) indirectly link The Addiction-Risk-Factor to psychopathology. Finally, given that genetic liability to substance use (e.g., ever using, quantity-frequency) and later stages of SUDs are partially distinct7,12,13, we repeat all analyses while incorporating genetic liability to substance use (i.e., alcohol drinks/week26; tobacco ever regularly use26, cannabis ever use27) as covariates.
We hypothesized that SUDs and problem substance use would be largely characterized by a common genetic vulnerability (i.e., The Addiction-Risk-Factor) with evidence of potentially important substance-specific liability (e.g., metabolic and signaling pathways for a specific drug such as ADH1B variants with alcohol28). We hypothesized that (i) The Addiction-Risk-Factor would be associated with all 3 non-substance psychiatric clusters while retaining variance unique to itself, (ii) genetic liability to behavioral phenotypes representing vulnerability to stage-based addiction constructs (i.e., risk-taking, executive function, and neuroticism) would be associated with The Addiction-Risk-Factor and account for a proportion of the association between The Addiction-Risk-Factor and psychopathology factors, and (iii) after accounting for genetics of substance use, The Addiction-Risk-Factor would retain unique variance (i.e., we expect significant residual genetic correlations among SUDs) and maintain similar patterns with non-substance psychopathology and stage-based constructs.
METHODS
Samples
Summary statistics from the largest available discovery GWASs were used to represent genetic risk for each construct (more details are in Supplemental Table 1). These include: i) 4 SUDs (problematic alcohol use22, problematic tobacco use25, cannabis use disorder7, opioid use disorder5); ii) 3 substance use phenotypes (alcohol drinks/week26, lifetime ever smoking26, lifetime cannabis use27); iii) 3 traits proxying the stage-based model of SUDs (risk-taking, executive function, neuroticism); and iv) 9 non-substance psychiatric disorders. Analyses were restricted to data from individuals of European ancestry because GWAS on these constructs in other ancestral origins are not available or are underpowered, and cross-ancestry analysis can confound genetic correlation estimates29. All GWAS summary statistics were filtered to retain variants with minor allele frequencies > 0.01 and INFO score > 0.90 for GSCAN and PGC7,26 and INFO score > 0.70 for the MVP5,30.
Indirect associations from a mediation model (see Figure 4) where stage-based constructs link non-substance psychopathology (3 factors from Lee et al.,) and The Addiction-Risk-Factor. F1 = compulsive disorders, F2 = Psychotic disorders, F3 = Neurodevelopmental disorders. The proportion accounted for by the indirect association (%) and the significance of the indirect association are shown. * P < .05 for the indirect association pathway.
Problematic Substance Use/Substance Use Disorder Summary Statistics
Problematic Alcohol Use
Summary statistics for problematic alcohol use (PAU) were derived from a meta-analysis of GWASs of DSM-IV alcohol dependence from the Psychiatric Genomics Consortium11 (PGC-AD; n = 11,569 case, 34,999 controls), ICD-9/10 based diagnoses of alcohol use disorders from the Million Veteran Program phase 1 and 2 data (MVP; n = 45,995 cases; 221,396 controls)9 and the Problem subscale score from the Alcohol Use Disorders Identification Test (AUDIT-P)13 from the UK Biobank (n = 121,604)22. The final GWAS summary statistics included data on 435,563 participants22. We also report on model fit with PGC-AD (instead of PAU) in the supplement (Alternative Models, M1).
Problematic Tobacco Use (PTU)
We used summary statistics from the GWAS of the Fagerström Test for Nicotine Dependence25 (FTND). As cigarettes per day is an item within the FTND and the genetic correlation between FTND and cigarettes per day is high (calculated rG = 0.97 CI = .12)12, we combined CPD And FTND into a single indicator. We applied Multi-Trait Analysis of Genome-wide association study summary statistics (MTAG31) to summary statistics generated from the GWAS and Sequencing Consortium of Alcohol and Nicotine Use (GSCAN) GWAS of cigarettes per day to create the combined problematic tobacco use (PTU) phenotype26. The final GWAS summary statistics had an effective sample size of n = 270,120 individuals. We also report on model fit with just FTND as an indicator in the supplement (Alternative Models M2).
Cannabis Use Disorder (CUD)
Summary statistics were derived from a GWAS meta-analysis7 of DSM-IV and DSM-III-R cannabis abuse and dependence from the Psychiatric Genomics Consortium (n = 5,289 cases; n = 10,004 controls), ICD-10 cannabis use disorder from the Lundbeck Foundation Initiative for Integrative Psychiatric Research (iPSYCH) (n = 2,758 cases; n = 53,326 controls), and hospital-based diagnoses from deCODE (n = 6,033 cases; n = 280,396 controls). The final European-ancestry sample included 14,080 cases with CUD and 343,726 controls.
Opioid Use Disorder
Opioid use disorder (OUD): Summary statistics were derived from a meta-analysis5 of GWASs of DSM-IV opioid abuse or dependence from Yale-Penn, and the Study of Addiction: Genetics and Environment, and ICD-9/10 codes for opioid use disorder from the Million Veteran Program (n = 10,544 cases; n = 72,163 opioid-exposed controls).
Substance Use Summary Statistics
Alcohol use
Alcohol use summary statistics were derived from the GSCAN GWAS32 for current (this past week or average in the past year) reported drinks/week (n = 537,349). There was a strong correlation with lifetime PAU (SNP-rG between drinks/week and PAU = 0.77±0.02)22.
Lifetime Tobacco Use
Summary statistics came from the GSCAN GWAS of reported ever/never regular cigarette smoking (ever n = 301,524, never n = 331,278). There was a moderate correlation with PTU (SNP-rG = 0.28±0.03).
Stage-based Behavioral Constructs
The three-stage behavioral model of addiction focuses on “state” changes in substance use behaviors. Because GWASs measure individual differences in traits, we selected behaviors that (1) are known to convey vulnerability to each stage as proxies, and (2) are heritable.
Risk-taking and sensitivity to reward
A GWAS of risk-taking derived from a single item in the UK Biobank (“Would you describe yourself as someone who takes risks?”; data field #2040; risk taker n = 83,677; non-risk taker n = 244,662)33.
Executive Function
The “preoccupation/anticipation” stage is characterized by maladaptive reward valuation and future planning. Recent work argues that this vulnerability is captured by executive functioning34. Summary statistics from a GWAS of a latent factor representing common executive functioning were used (N = 427,037)23.
Negative Emotionality and Sensitivity to Stress
The stage of withdrawal/negative affect represents substance use functioning to mitigate aversive withdrawal symptoms, such as negative affect. Neuroticism has been found to modify stress sensitivity and neural reward processing35. Neuroticism was chosen as a trait-based measure representing liability to negative affect as opposed to depression because depression was included in the non-substance psychiatric disorder factor generation and because neuroticism includes trans-diagnostic constructs such as negative urgency (i.e., impulsive attempts to cope with negative affect) that may place individuals at risk for the negative reinforcing aspects of SUDs. We selected the largest GWAS of neuroticism as a heritable proxy (N = 390,278)20.
Non-Substance Summary Statistics
Summary statistics from the PGC Cross-disorder GWAS on the 8 disorders that were previously shown to fit a 3 factor confirmatory model were used14. These disorders included Schizophrenia36, Bipolar disorder37, Major depressive disorder38, Attention Deficit Hyperactivity disorder39, Obsessive Compulsive Disorder40, Anorexia Nervosa41, Tourette Syndrome42, and Autism Spectrum Disorder43 (See Supplemental Table 1 for details).
Statistical analysis
First, we estimated the pairwise genetic correlations between PAU, PTU, CUD and OUD using Linkage Disequilibrium Score Regression (LDSR)29. After confirming that the four SUDs were significantly genetically correlated (see Results), we applied confirmatory factor analysis to the covariance matrix generated by LDSR using gSEM44 with weighted least squares estimation; PAU, PTU, OUD, and CUD indicators were allowed to load freely on a single latent factor (i.e., The Addiction-Risk-Factor). Variance of this common latent factor was scaled to 1.0. A residual correlation between PAU and OUD was also estimated to account for measurement overlap, because the Million Veterans Project sample was contained in both PAU and OUD GWAS (but see model fit without this residual correlation in the supplement – Alternative Models M1). In supplemental analyses, we also examined alternative two factor models (Alternative Models M3).
Second, we used a series of structural regression models to estimate the extent to which genetic liability to stage-based constructs of addiction (i.e., risk-taking, executive function and neuroticism) are related to The Addiction-Risk-Factor. Here, the Addiction-Risk-Factor variance was freed, and the OUD loading was set to 1.0 to scale the model. Intercorrelations were estimated between risk-taking, executive function and neuroticism.
Third, we recreated the three factors from Lee et al14. (i.e., psychotic disorders, compulsive disorders, and early neuro-developmental disorders) and estimated their relationship with The Addiction-Risk-Factor while allowing for inter-factor correlations (the association between The Addiction-Risk-Factor and an alternative cross-disorder genetic model from a preprint45 was also estimated; this alternative model is shown in Supplemental Figure 5). This allowed us to estimate the unique association between each of the 3 psychopathology factors and The Addiction-Risk-Factor and to estimate variance that was residual to The Addiction-Risk-Factor. We then examined whether proxies for stage-based addiction constructs (i.e., risk-taking, executive function and neuroticism) indirectly linked The Addiction-Risk-Factor to the 3 non-substance psychopathology factors using a multiple mediator model. We also conducted supplemental modified Q-Trait analyses45 to examine the extent of the mediation (Q-Trait Analysis). To estimate residual associations (i.e., direct paths) between the stage-based constructs and The Addiction-Risk-Factor, we re-structured the mediation model to one in which the 3 non-SUD psychopathology factors served as “mediators” of the relationship between risk-taking, executive functioning, neuroticism, and The Addiction-Risk-Factor.
To separate the genetics of SUD from the genetics of substance use, we estimated models where substance use GWAS summary statistics were endogenous predictors of all measured variables in the model. For example, in the model estimating the association between The Addiction-Risk-Factor and psychiatric factors, the 8 psychiatric disorders and the 4 SUD disorder variables were regressed on the 3 substance use variables. In this way, covariate effects were estimated simultaneously to our associations of interest.
RESULTS
The Addiction Risk Factor
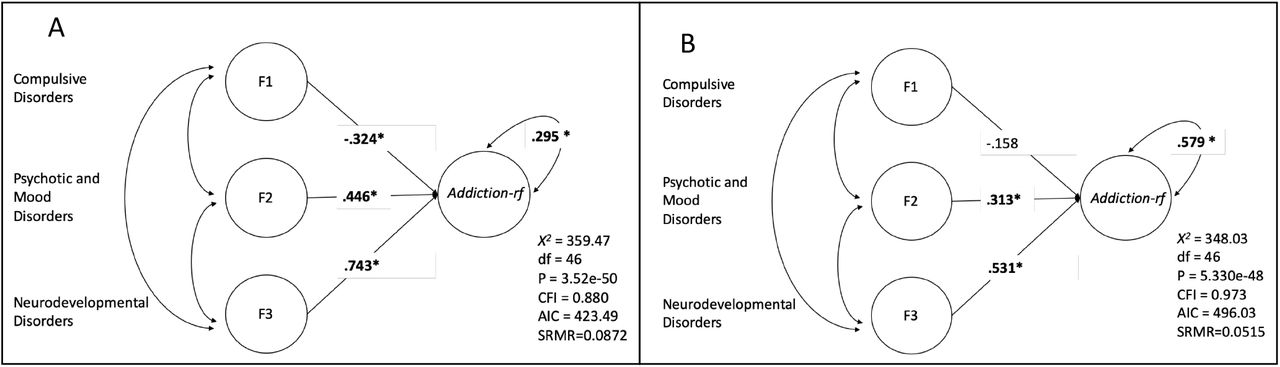
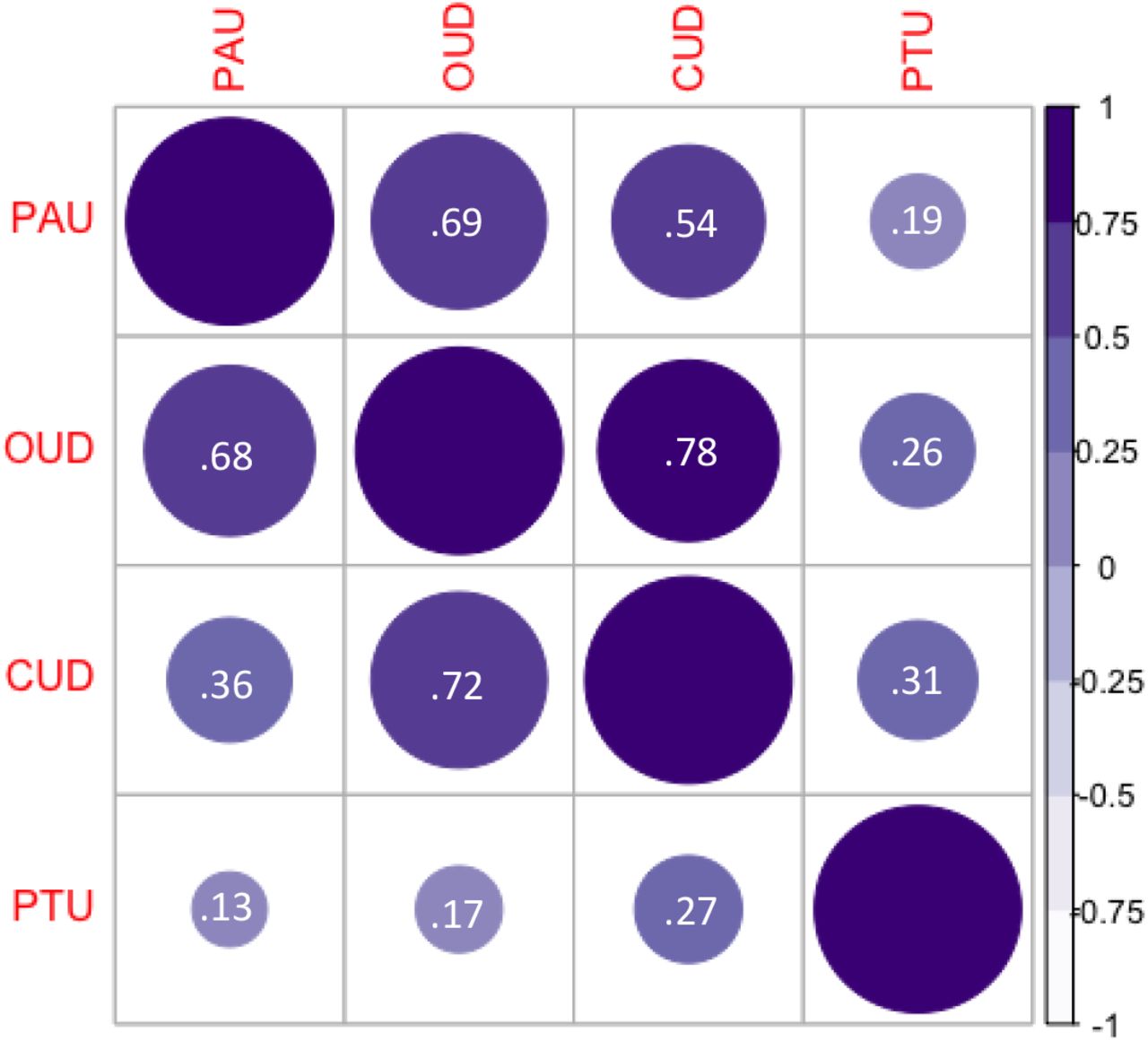
Genetic correlations between problematic alcohol use (PAU22), problematic tobacco use (PTU25,26), cannabis use disorder (CUD7), and opioid use disorder (OUD5) ranged from 0.19 (S.E. = .04) to 0.78 (.09) (Supplemental Figure 1 and Supplemental Figure 2). PTU showed the lowest SNP-rG with other SUD phenotypes [i.e., PAU = 0.19 (.04), CUD = 0.31 (.05), OUD = 0.26 (.08)] while OUD showed the highest [PAU = 0.69 (.07), CUD = 0.78 (.09)]. A confirmatory factor model specifying a unidimensional Addiction-Risk-Factor underlying the genetic covariance among PAU, PTU, CUD and OUD fit the data well [X2(1) = .017, p = .895, CFI = 1, SRMR = .002; residual r = .51, p = 0.016; Figure 1A]. Loadings were uniformly high except for PTU. Neither PAU nor PTU were impacted by the inclusion of non-diagnostic indices of addiction risk (Supplemental Results Alternative Models M1-M2). Alternative 2-factor models did not fit the data well (Alternative Models M3).

Panel A: the model, loadings, and fit for a model that allowed all 4 SUD categories to load on a latent factor. A residual correlation was added between OUD and PAU to account for large sample overlap (both used the Million Veterans Project data; models without residual correlations also fit well: Supplemental Figure 3). Addiction-rf=The Addiction Risk-Factor. Panel B: the same model, but accounting for common substance use (ever smoke, ever use marijuana, and drinks per week) as covariates at the indicator level, i.e. the three substance use measures are exogenous to all indicators in this model and the model represents the residual associations after accounting for substance use. Both models provided excellent fit to the data. Bold* represents significance at p < .05. Note that in panel B, the residual of CUD is zero; this model constraint was necessary, as the model produced a negative residual without the constraint. Note: If you want to recreate the correlation matrix from both panels, the model with residual correlations cannot recover the implied correlation between PAU and OUD without taking the square root of the residual variance, rather than the value of the residual variance itself.

Executive Function, Neuroticism and Risk-taking. Panel A the model, fit, and regression pathways without accounting for common substance use. Panel B is the same model, but accounting for common substance use (ever smoke, ever use marijuana, and drinks per week) as covariates at the indicator level (regressed on all measured variables/GWAS). Bold* represents significance at p < .05.
The inclusion of genetic liability to typical substance use did not modify the single factor structure of The Addiction-Risk-Factor (Figure 1B); all SUDs continued to load significantly on the factor. However, factor loadings were lower for all substances, especially for PAU, which may be attributable to the high genetic correlation between drinks/week and PAU. Alternative parameterization of substance use as covariates did not improve model fit (Alternative Models M4).
Shared Liability to Stage-based Behavioral Phenotypes
Genetic liability to stage-based addiction constructs was shared with The Addiction-Risk-Factor (Figures 2, Q-Trait Analysis in Supplemental Methods). As expected, The Addiction-Risk-Factor was positively associated with genetic liability to risk-taking (β = 0.45) and neuroticism (β = 0.25), and negatively associated with executive function (β = -0.17; Figure 2A). Despite significant genetic overlap between The Addiction-Risk-Factor and stage-based behavioral phenotypes, The Addiction-Risk-Factor retained unique variance (Addiction-Risk-Factor residual = 0.68). When conditioning for genetic liability for substance use, The Addiction-Risk-Factor remained significantly associated with increased genetic liability to risk-taking (β = 0.22) and neuroticism (β = 0.18) and decreased genetic liability to executive function (β = -0.28; Figure 2B). Accounting for genetic liability for substance use substantially reduced the association between The Addiction-Risk-Factor and risk-taking from 0.45 to 0.22 (pdf = 1 = 4e-09) and accentuated the negative association with executive function from β = -0.17 to -0.28 (p(df = 1) = 0.013); there was a smaller effect on the association with neuroticism (from β = 0.25 to 0.18, p(df = 1) = 0.012).
Shared Liability to Non-substance Psychopathology
Genetic liability to non-substance psychopathology (i.e., compulsive disorders, psychotic disorders, and neurodevelopmental disorders) was shared with The Addiction-Risk-Factor (Figure 3, full models in Supplemental Figure 4; Supplemental Figure 5 shows results with an alternative cross-disorder model from a recent preprint45). Psychotic disorders (β = 0.45) and neurodevelopmental disorders (β = 0.74) were positively associated with The Addiction-Risk-Factor while compulsive disorders showed a negative association (β = -0.32; Figure 3A). Due to the strong correlation between The Addiction-Risk-Factor and early-onset neurodevelopmental disorders (which includes ADHD) we allowed ADHD to load on The Addiction-Risk-Factor to control for ADHD; here, an association between The Addiction-Risk-Factor and early-onset neurodevelopmental disorders remained, but was significantly attenuated (from β = 0.74 to 0.43, p(df = 1) = 5e-5). When conditioning The Addiction-Risk-Factor for substance use, the psychotic and early neurodevelopmental disorder factors remained significantly associated with The Addiction-Risk-Factor (Figure 3B). Despite the significant genetic overlap with other psychiatric disorder domains, The Addiction-Risk-Factor retained unique variance representing genetic liability specific to SUDs (The Addiction-Risk-Factor residual = 0.30, p = 4.54e-3). This unique variance remained significant when accounting for genetic liability to substance use (The Addiction-Risk-Factor residual = 0.58, p = 0.015).

Compulsive disorders (F1; Tourette’s syndrome, Obsessive compulsive disorder, and Eating Disorders), Psychotic Disorders (F2; Major Depressive Disorder, Schizophrenia, and Bipolar Disorder) and neurodevelopmental dysfunction (F3; ADHD, Autism, and Major Depressive Disorder). Panel A the model, fit, and regression pathways without accounting for common substance use (model was scaled by setting the Opioid Use Disorder loading to 1). Panel B is the same model, but accounting for common substance use (ever smoke, ever use marijuana, and drinks per week) as covariates at the indicator level (regressed on all measured variables/GWAS), i.e. the three substance use measures are exogenous to all indicators in this model and the model is the residual associations after accounting for substance use. Bold* represents significance at p < .05. Addiction-rf = The Addiction-Risk-Factor.
The specifications for the mediation models are shown in Supplemental Figure 6. Genetic liability to risk taking accounted for a proportion of the associations between all non-substance psychopathology domains and The Addiction-Risk-Factor (Table 1). Executive function uniquely indexed an indirect effect between psychotic disorders and The Addiction-Risk-Factor (Table 1). When conditioning The Addiction-Risk-Factor for genetic liability to substance use, risk-taking no longer accounted for a portion of the association between any non-substance psychopathology domain and The Addiction-Risk-Factor, but executive function continued to account for a proportion of the overlap (indirect effect of 0.048) between psychotic disorders and The Addiction-Risk-Factor (Table 1). Post-hoc analyses revealed that executive function retained a unique association with The Addiction-Risk-Factor after accounting for genetic liability to both substance use and non-substance psychopathology (Supplementary Table 2).
DISCUSSION
We applied genomic structural equation modeling (gSEM)24 to GWAS summary statistics to characterize the genetic influences shared across SUDs and estimate how common genetic liability is related to trait conceptualizations of a theoretical stage-based SUD model as well as to non-substance psychopathology. Three primary findings emerged. First, genetic risk for specific SUD phenotypes (i.e., PAU22, PTU25,26, CUD7, and OUD5) was largely attributable to a single Addiction risk factor, The Addiction-Risk-Factor (Figure 1). Second, The Addiction-Risk-Factor was associated with genetic liability to trait representations of stage-based facets of addiction (risk taking [binge/intoxication], executive function [preoccupation/anticipation], neuroticism [negative affect]19; Figure 2). It was also associated with non-substance psychopathology factors (compulsive disorders, psychotic disorders, neurodevelopmental disorders; Figure 3). Trait representations of stage-based facets of addiction partially accounted for the shared genetic liability between non-substance psychopathology and The Addiction-Risk-Factor. Third, associations between The Addiction-Risk-Factor and stage-based constructs and non-substance psychopathology were largely independent of genetic liability to substance use phenotypes (i.e., tobacco use, cannabis use, alcoholic drinks/week). However, consistent with the stage-based model of addiction, accounting for substance use attenuated associations between risk taking and The Addiction-Risk-Factor while potentiating associations with executive functioning. Collectively, our findings suggest that SUDs are characterized by a common genetic factor, Addiction-Risk-Factor.
The Addiction-Risk-Factor retains variance that is not shared with other psychopathology
After accounting for genetic liability to substance use as well as the commonality between The Addiction-Risk-Factor and non-substance psychopathology, The Addiction-Risk-Factor retained significant variance. These data suggest that The Addiction-Risk-Factor may be characterized by unique pathways not shared with substance use or non-substance psychopathology, i.e., addiction is not the linear combination of substance use and psychopathology.
A single latent factor, fit these data well, but specific SUDs showed varying degrees of association. The illicit SUDs (CUD and OUD; Figure 1) were almost entirely captured by the common latent factor. Notably, the loading for PTU on The Addiction-Risk-Factor was the smallest. One potential contributor to the residual variance of PTU may be the use of FTND and cigarettes/day as indices of PTU. Unlike the Diagnostic and Statistical Manual (DSM) criteria which index psychological and physiological aspects of tobacco use disorder, the FTND is an index of biochemical dependence and although used widely by investigators to define addiction, phenotypically shows only moderate agreement with DSM-defined nicotine dependence (r = 0.50; kappa = 0.3)46.
Proxies of Stage-based Behavioral Constructs and The Addiction-Risk-Factor
Behavioral stage-based models of SUD posit a cyclical relationship between positive reinforcement, negative reinforcement, and incentive salience19 that we found can be (partially) captured by genetic liability to risk-taking, executive functioning, and negative emotionality (neuroticism). The strongest association with The Addiction-Risk-Factor was for risk-taking.
When substance use was included as a covariate in the model, the shared genetic loading between The Addiction-Risk-Factor and both risk-taking and neuroticism was attenuated down while the association with executive function increased. The reduction in the association with neuroticism is counter to expectations from the stage-based model which posits a more prominent role of negative affect for SUD relative to substance use. We speculate that neuroticism, which represents an amalgam of negative affect traits, may be too broad a construct when considering SUD-specific negative affect; large-scale studies of domains of negative affectivity (e.g., negative urgency) are needed.
Non-substance Psychopathology and The Addiction-Risk-Factor
We found that the 3 non-substance psychopathology clusters, derived from 8 psychiatric disorders14, were genetically associated with The Addiction-Risk-Factor. The association with early neurodevelopmental disorders, which include ADHD, was the strongest. Cross-loading ADHD on The Addiction-Risk-Factor to condition on ADHD attenuated the loading but it remained high. Associations between The Addiction-Risk-Factor and the psychopathology clusters were greater than associations with trait representations of behavioral stages of addiction (with the exception of risk-taking). For instance, the genetic association between The Addiction-Risk-Factor and the two disorder clusters that included Major Depressive Disorder (i.e., psychotic disorders and early neurodevelopmental disorders) was greater in magnitude than the Addiction-Risk-Factor-neuroticism association. Interestingly the compulsive disorder factor did not show strong associations with The Addiction-Risk-Factor, suggesting that compulsive disorders and addiction-related compulsive behaviors have distinct etiologies.
Of the 3 behavioral correlates, risk-taking was the most prominent contributor to the association between The Addiction-Risk-Factor and all non-substance psychopathology factors. After accounting for substance use, only risk-taking and executive function mediated The Addiction-Risk-Factor associations with the psychotic disorder factor. Executive function maintained the only direct association with The Addiction-Risk-Factor after accounting for genetics of substance use and genetics of non-substance psychopathology. Thus, we speculate that while risk-taking may characterize the genetic overlap between substance use and other psychopathology, executive function impairment is a risk factor that not only shapes the overlap between addiction and non-substance psychopathology but also explains variance in addiction above and beyond that overlap.
Limitations
There are several limitations. First, we had to restrict our analyses to individuals of European descent due to the lack of well-powered discovery GWAS informative for other ancestry groups. Second, to maximize sample size of discovery GWASs, our alcohol and tobacco use GWAS incorporated measures of “problematic” use that, while genetically highly correlated with AUD and ND, may include behavioral patterns that are less severe than those represented by use disorder and were not assessed based on clinical presentation. Third, the analyses contain an over-representation of men, in part because the MVP samples contributed most of OUD and half of PAU and the MVP is ∼90% male. Studies with larger numbers of women would allow stratified analyses to explore the differences between sexes observed in epidemiological studies. Fourth, while it is unlikely that individuals completed assessments of risk-taking, neuroticism, and executive function while under the influence of substances, how substance use may have influenced these assessments cannot be determined. Fifth, though significant, mediation pathways were small in effect. Sixth, how these processes effect phenotypic patterns is unknown, however twin studies support a common factor model as well4.
Conclusions
Common genetic liability undergirds distinct SUDs and shares variance with putative behavioral intermediary phenotypes/SUD risk factors and non-substance psychopathology. This addiction genetic factor is more than a linear combination of substance use and psychopathology; it represents a unique addiction dimension that is partially captured by executive functions.
Data Availability
All data are made publicly available through their respective consortiums.
Funding
This research was supported by MH109532 (AA, JG, HJE, ECJ) and T32DA007261 (ASH). AA acknowledges K02DA32573. ECJ was supported by F32AA027435. RP acknowledges R21DA047527. RB acknowledges R21-AA027827.
The Substance Use Disorders Working Group of the Psychiatric Genomics Consortium (PGC-SUD) is supported by funds from NIDA and NIMH to MH109532. Disclosures/COI: JG is named as an inventor on PCT patent application #15/878,640 entitled: “Genotype-guided dosing of opioid agonists,” filed January 24, 2018. The authors have no conflicts of interest.
Supplemental Tables and Figures
Alternative Model specifications
To establish our factor model, we tried several different approaches. First, we confirmed that the problematic alcohol use (PAU) and problematic tobacco use (PTU) variables did not significantly alter factor structure, as these are more proxies of the underlying construct of interest. Samples that are about an order of magnitude smaller are available for this exploration.
First, we reran the model with alcohol dependence from the Psychiatric Genetics Consortium GWAS of European descent (N= 38,686)1 as the indicator for alcohol use disorder, instead of the larger problematic alcohol use (PAU) GWAS (Models M1). As the PGC alcohol dependence GWAS did not include data from the MVP, we also used this as an opportunity to test whether the residual genetic correlation between opioid use disorder (OUD) and alcohol dependence was present in the absence of measurement overlap. The model fit well (X2 = 1.22, p = .54, df = 2, CFI = 1). When we tested the residual correlation, it was large although no longer significant (r=0.71, P=4.46e-01). The residual variance for alcohol dependence was also not significant (r=0.207 p=.51). As the alcohol dependence measure without MVP does not have a significant residual correlation, we posit that the need for the residual correlation when the MVP PAU summary data are used is to improve fit due to the larger sample or due to measurement overlap in the MVP.
Second, we tested whether inclusion of cigarettes per day with FTND created a poor proxy for tobacco dependence (Model M2). The model with FTND an indicator fit well, (X2 = 0.027, p = .987, df = 2, CFI = 1) FTND indictor pathway was larger, but the confidence intervals overlapped substantially (r = .502, CI = .121).
For our next test of robustness, we conducted two follow-up analysis to examine whether parsing Addiction-rf into a two-factor structure improved fit (Models M3). The highest pairwise associations between SUD indicators were OUD with PAU. PTU with CUD also showed a high pairwise associations. Both factors were allowed to correlate. This model did not fit the data well (model fit: X2 = 34.039, p = 1.94e-07, df = 3, CFI = .924, AIC = 47.039). We also fit a model where PAU and PTU loaded on one factor (“licit drugs”) while CUD and OUD loaded on another correlated factor (“illicit drugs”). This model did not fit the data well either (model fit: X2 = 293924.2, p = <.001, df = 5, CFI = -721.5134, AIC = 293934.2).
Next, there are two alternative models we tested to see if there was a more appropriate analysis to account for substance use (Models M4). To be clear, substance use is a covariate, but its covariate effect may be better modeled via alternative models. First, we generated a substance use factor using ever smoking regularly, marijuana use, and drinks per week as indicators. We then regressed the use disorder indicators on this factor. This model fit the data poorly. (X2=394.4224, df=1, p=5.739041e-77 AIC=426.4224 CFI=0.8833732) and significantly worse than our original model (X2 diff=394.007, df=9, p=2e-64).
Next, rather than have the substance use variables endogenous to the indicators of addiction factor, we tested whether an alternative model where the indicators predicted the addiction factor directly fit the data better via a nested comparison. A model with the substance use variables predicting addition-rf fit the data poorly (X2=324.481, df=10, P=1.025754e-63, AIC=360.481, CFI=0.9040932).
Q-Trait Analysis
Background. Background
Q-Trait analysis1 was developed to test whether a latent genetic factor estimated using gSEM mediates the genetic association between an external trait (i.e., one not loaded onto the latent genetic factor) and factor indicators (those loading on the latent genetic factor). We conducted Q-trait analysis to test whether The Addiction-Risk-Factor accounts for genetic associations between these traits and each individual SUD indicator loading onto it (i.e., OUD, PAU, PTU, CUD). Q-Trait analysis evaluates this by comparing one model in which only the latent genetic factor is associated with the external trait to another model in which each indicator (i.e., the trait loading onto the genetic factor) is associated with the external trait. A χ2 difference between these models is calculated and if there is a significant difference, it suggests that the genetic association between the external trait and the factor indicators are not accounted for by the latent genetic factor. However, this analysis is conducted with all factor indicators in a single model independent of the latent factor, and does not model scenarios in which the latent factor may differentially mediate (e.g., fully, partially, or not at all) individual factor indicators. Because of this limitation, in cases where we found no evidence that the latent genetic factor completely mediated the genetic association between the external trait and factor indicators (i.e., when there was a significant χ2 difference), we conducted a series of post-hoc models regressing the latent genetic factor and each individual genetic indicator on the external traits in an iterative processes (For example, a model in which the latent genetic Addiction-Risk-Factor and problematic tobacco use were regressed on executive function).
Results
Q-Trait analysis revealed that the latent genetic Addiction-Risk-Factor mediated associations between risk-taking and individual SUD indicators, as indicated by a lack of significance in model fit (X2diff(3) = 6.478, P=0.091). Although initial Q-trait modeling provided no evidence that the latent genetic Addiction-Risk-Factor accounted for associations between individual SUD indicators with executive function (X2diff(3) = 25.7, P = 1.00e-5) and neuroticism (X2diff(3) = 625.7, P=1.00e-5), post-hoc analyses revealed that the lack of evidence for mediation is attributable to differential mediation across indicators. Executive function is correlated with The Addiction-Risk-Factor, but shows stronger associations with problematic alcohol use, cannabis use disorder, and opioid use disorder than problematic tobacco use (see Supplemental Table 1). Because of this we tested an additional model wherein the latent genetic Addiction-Risk-Factor and problematic tobacco use were regressed on executive function simultaneously, which revealed no significant difference from the model in which all individual SUD indicators were included (X2diff(2) =4.635, P = .0985), suggesting that the common latent Addiction-Risk-Factor mediates associations between executive function and PAU, OUD, and CUD, but not PTU. Further, additional regression path greatly bolstered upward the association between The Addiction-Risk-Factor and executive function (r=-.31, p = 1.00e-17). For neuroticism, the addition of specific paths with PAU and CUD in addition to The Addiction-Risk-Factor revealed evidence that the latent genetic factor mediates associations with OUD and PTU (X2diff(1) = 2.798, P=0.0944). However, this did not change the association with the latent factor (r=.20, p=7.08e-3); it is simply that neuroticism has associations with PAU and CUD that are independent of The Addiction-Risk-Factor.
Interpretation for downstream analysis
Downstream analysis did not retain these specific associations. For executive functioning, we still found significant associations between cEF and addiction risk, and mediating pathways despite the association being attenuated downward by our chosen model. Neuroticism did not maintain mediating pathways, and so improving the model would not have led to additional discovery power for the neuroticism phenotype.
Behavioral Liabilities Mediate the Association Between -Factor and Psychiatric Factors
Indirect associations from a mediation model (see Figure 4) where stage-based constructs link non-substance psychopathology (three factors from Lee et al.,) and The Addiction-Risk Factor (Addiction-rf). Indirect association is represented by the proportion accounted for by the indirect association (%) and the significance of the indirect association. F1 = compulsive disorders, F2 = Psychotic disorders, F3 = Neurodevelopmental disorders.

Genetic correlations (SNP-rG) were estimated between all variables. The upper diagonal represents the bivariate associations from LD Score regression. PAU = Problematic Alcohol Use, OUD = Opioid Use Disorder CUD = Cannabis Use Disorder. PTU = Problematic Tobacco Use. FormerSmoke = smoking cessation, AgeSmoke=Age first smoking regularly, MJUse = Marijuana Use, DPW = Drinks Per Week, EverSmoke = Ever Smoking regularly, NE = neuroticism, Risk = Risk-taking, EF = Executive Function, PTSD = Post-Traumatic Stress Disorder, TS = Tourette’s Syndrome, OCD = Obsessive Compulsive Disorder, GAD = General Anxiety Disorder, MDD = Major Depressive Disorder, BiP = Bipolar disorder, Scz = Schizophrenia, ADHD =

Genetic correlations (SNP-rG) were estimated between all substance use disorder categories. The upper diagonal represents the bivariate associations from LD Score regression. The lower diagonal are correlations estimated in Genomic Structural Equation Modeling when controlling for common substance use (drinks per week, ever smoking marijuana or tobacco). All genetic correlations were positive (shown in purple). PAU = Problematic Alcohol Use, OUD = Opioid Use Disorder CUD = Cannabis Use Disorder. PTU = Problematic Tobacco Use. All rGs were significant (all p> .01).

Alternative specification of one factor model, without residual correlation between problematic alcohol use and opioid use disorder.

The top two panels represent the standardized estimates, the bottom two are unstandardized with standard errors. The left panels include the substance use variables as covariates. Bold*= p-value < .05.

Alternative model of psychopathology, taken from Grotzinger et al.2 the left panel represents the model with standardized estimates. The right panel represents the unstandardized estimates with standard errors. Bold*= p-value < .05.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Model Specification for Mediation Models Linking non-substance psychopathology and Addiction-rf.
In panel A, we tested whether neurobiological stage-based constructs mediated the association between the Addiction-rf-Factor and non-substance psychopathology. In mediation model two, we tested whether neurobiological stage-based constructs had remaining (direct) associations with Addiction-rf beyond non-substance psychopathology variables.
Acknowledgments
We gratefully acknowledge our contributing studies and the participants in those studies without whom this effort would not be possible.
The MVP summary statistics were obtained via an approved dbGaP application (phs001672.v4.p1). The authors thank Million Veteran Program (MVP) staff, researchers, and volunteers, who have contributed to MVP, and especially participants who previously served their country in the military and now generously agreed to enroll in the study. (For details, see https://www.research.va.gov/mvp/ and Gaziano, J.M. et al. Million Veteran Program: A mega-biobank to study genetic influences on health and disease. J Clin Epidemiol 70, 214-23 (2016)). This research is based on data from the Million Veteran Program, Office of Research and Development, Veterans Health Administration, and was supported by the Veterans Administration (VA) Cooperative Studies Program (CSP) award #G002.
This study included summary statistics of a genetic study on cannabis use (Pasman et al, 2018 Nature Neuroscience). We would like to acknowledge all participating groups of the International Cannabis Consortium, and in particular the members of the working group including Joelle Pasman, Karin Verweij, Nathan Gillespie, Eske Derks, and Jacqueline Vink. Pasman et al, (2018) included data from the UK Biobank resource under application numbers 9905, 16406 and 25331.
Footnotes
Additional Supplemental models and name changes.
Reference Cited



