
Abstract
Objectives To firstly investigate the efficacy of three different dosages of home-based, knee-extensor strength exercise on isometric knee-extensor strength in patients eligible for knee replacement due to severe knee osteoarthritis, and secondly, the influence of exercise on symptoms, physical function and decision on surgery.
Design Randomized dose-response trial.
Setting Primary and secondary care.
Participants One-hundred and forty patients eligible for knee replacement were included. Eligibility for surgery was assessed by an orthopedic surgeon specialized in knee arthroplasty.
Interventions Patients were randomized to three groups; 2, 4 or 6 home-based knee-extensor exercise-sessions per week (group 2, 4 and 6 respectively) for 12 weeks (N=47/group). Exercise instruction was given by a trained physiotherapist.
Main outcome measures The primary outcome was isometric knee-extensor strength. Secondary outcomes were Oxford Knee Score, Knee Osteoarthritis Outcome Score, average knee pain last week (0-10 numeric rating scale), 6-minute walk test, stair climbing test, exercise adherence and “need for surgery”. The primary endpoint was after 12 weeks of exercise (before surgery) and the secondary after surgery. Outcome assessors and patients were blinded to allocation.
Results After 12 weeks of exercise, data were available for 117 patients (N=39/group). Isometric knee-extensor strength increased in all groups but intention-to-treat analysis showed no difference between the three groups in change from baseline to after 12 weeks of exercise in isometric knee-extensor muscle strength: Group 2 vs. 4 (0.009 Nm/kg [95% CI−0.15 to 0.17], P=0.913), group 2 vs. 6 (−0.03 Nm/kg [95% CI−0.18 to 0.13], P=0.725) and group 4 vs. 6 (−0.04 Nm/kg [95% CI−0.20 to 0.13], P=0.668). For the secondary outcomes a significant difference before surgery was found between group 2 and group 6 for Oxford Knee Score (4.2 [95% CI 0.6 to 7.8], P=0.02) and average knee pain last week (NRS 0-10) (−1.1 [95%−2.2 to−0.1], P=0.03) in favour of group 2. No other differences were observed before and after surgery. After the 12-week exercise intervention, 38 (32.5%) patients wanted surgery and 79 (67.5%) postponed surgery. This was independent of exercise dosage.
Conclusion Knee-extensor strength increased with both 2, 4 and 6 exercise sessions per week but none of the prescribed exercise dosages were superior to the others for the primary outcome isometric knee-extensor strength after 12 weeks. Two home-based knee-extensor exercise sessions a week seems superior to six for patient-reported outcomes, and across exercise dosages, only one in three patients decided to have surgery after the coordinated home-based exercise intervention.
Trial registration ClinicalTrials.gov identifier: NCT02931058, pre-registered October 10th, 2016. Protocol PubMed (PMID: 29347947).
What is already known on this topic Clinical guidelines recommend exercise therapy targeting the knee-extensor muscles in patients eligible for knee replacement before surgery is considered.
Exercise therapy may reduce knee osteoarthritis symptoms and impact the decision on surgery, but the dose-response relationship is not described.
Exercise therapy is typically delivered as supervised programs requiring physical attendance at fixed times and often require self-payment, which may be a barrier for some patients.
What this study adds Knee-extensor strength increased with 2, 4 and 6 exercise sessions per week, but none of the prescribed exercise dosages were superior to the others after 12 weeks – indicating no dose-response relationship.
Two in three patients eligible for knee replacement decided to postpone knee replacement surgery after 12 weeks of home-based exercise with one simple exercise.
This study successfully employed a model of coordinated care where the patients’ decision on surgical treatment was re-evaluated based on symptom changes following simple home-based exercise therapy. These findings suggest using a model of coordinated non-surgical and surgical care to improve the decision on surgery for patients eligible for knee replacement.
Introduction
Recent findings show that exercise therapy in patients with knee OA can reduce symptoms before potential surgery and postpone surgery in 50% or more of cases.1–4 In line with this, guidelines from knee OA societies recommend that exercise therapy is tried out before surgery is considered in patients eligible for knee replacement.5–10 Because the indication for knee replacement is not clear-cut, identifying the right patients to operate at the right time is difficult11,12 – making the coordination of non-surgical and surgical care crucial in selecting the right candidates for knee replacement.13–16 Any changes in symptoms after exercise therapy may play an important role in the shared decision-making process on the decision for surgery.17–20
Exercise programs for patients with knee OA like ‘Good Life with osteoArthritis in Denmark’ (GLA:D) - now successfully implemented worldwide21 - and ‘Better management of patients with OsteoArthritis’ (BOA) support the effectiveness of exercise therapy and education for this patient population and deliver optimized care.22–25 These exercise programs are supervised, require physical attendance at fixed times and often require self-payment; factors which can be barriers for some patients and hinder participation and long-term adherence, creating inequality for the care accessible.26–29 An important element in exercise programs for patients with knee OA is knee-extensor strength30, as decreased knee-extensor strength is associated with an increased risk of developing knee OA,31 risk of knee pain and decline in function.32 Our recent meta-regression analysis suggest no dose-response relationship between prescribed knee-extensor exercise and change in outcomes after knee-extensor exercise in patients scheduled for knee replacement – indicating that small exercise dosages might be equally effective to larger.33 Based on these results, we investigated the dose-response relationship of one home-based exercise targeting the knee-extensor muscles, using a very simple and low-cost exercise option. Compared to supervised exercise programs, this solution does not require physical attendance at fixed times and is free of charge – providing patients with an alternative treatment option.
The QUADX-1 trial was designed within a model of coordinated care where the patients’ decision on surgical treatment was re-evaluated based on symptom changes following home-based exercise therapy. The re-evaluation was a shared decision-making process between the patient and an orthopedic surgeon.
We asked the following questions:
Is there a dose-response relationship between knee-extensor exercise and change in isometric knee-extensor strength in patients eligible for knee replacement?
Do different dosages of simple knee-extensor exercise change symptoms and decision on surgery in patients eligible for knee replacement?
The purpose was mainly to investigate the efficacy of three different dosages of home-based, knee-extensor strength exercise on isometric knee-extensor strength in patients eligible for KR due to severe knee OA, and secondly, the influence of exercise on symptoms, physical function and decision on surgery. The primary hypothesis was that an exercise dosage of four knee-extensor strength sessions per week would elicit the greatest change in isometric knee-extensor strength pre-operatively compared to two or six sessions per week.
Methods
Trial design
This is the primary trial report for the Quadriceps Exercise Before Total Knee Arthroplasty Trial (The QUADX-1 Trial).34 The trial is a three-arm parallel-group randomized dose-response trial with three intervention groups and no control group. The three intervention groups all performed one home-based knee-extensor exercise for 12 weeks with dosages of 2, 4, or 6 sessions per week, respectively. Outcomes were assessed at 1) baseline, 2) after 12 weeks of exercise (primary endpoint), 3) acutely after surgery and 4) three months after surgery. The trial was double blinded with blinding of all outcome assessors and all participants in relation to the intervention in the other groups and the trial hypothesis. Between October 2016 and January 2019 patients eligible for KR at the Orthopedic Department at Copenhagen University Hospital, Hvidovre were invited to participate. We pre-registered the trial on clinicaltrials.gov on 10th October, 2016 (NCT02931058) before enrollment of the first patient, and published the full trial protocol - including protocol amendments - open access on 18th January, 2018.34 Approvals from the Ethics Committee of the Capital Region, Denmark (H-16025136) and the Danish Data Protection Agency (2012-58-0004) were obtained before the first patient was enrolled. This trial is reported according to recommendations in the CONSORT checklist.35
Participants
Patients potentially eligible for trial participation were recruited at the surgical outpatient clinic. The patients were referred from their general practitioner for surgical evaluation by an orthopedic surgeon specialized in KR surgery. The patients were told that if they agreed to participate, they would complete the home-based exercise intervention and afterwards their need for surgery would be re-evaluated. The inclusion criteria were: eligible for KR due to knee OA (assessed by an orthopedic surgeon), radiographically verified knee OA with Kellgren-Lawrence classification ≥ 2, average knee pain ≥ 3 (Numeric Rating Scale (NRS)) in the last week, eligible for home-based knee-extensor exercise, age ≥ 45 years, resident in one of three municipalities involved in the trial (Copenhagen, Hvidovre or Broendby) and able to speak and understand Danish. The exclusion criteria were: exercise therapy being contra-indicated, neurological disorder, diagnosed systemic decease (American Society of Anesthesiologists’ physical status classification score ≥ 4),36 terminal illness, severe bone deformity demanding use of non-standard implants, or a greater weekly alcohol consumption than the national recommendation.37
Interventions
Detailed intervention descriptions and all related intervention material can be found in the open access trial protocol34 – including a link to an instructional video (http://bit.ly/2EV7NrF). Following baseline assessment, the patients were referred to a physiotherapist in their local municipal rehabilitation setting. Here the patients were instructed how to perform a single knee-extensor exercise at home. The knee-extensor exercise was performed sitting on a chair with an exercise band wrapped around the ankle and fixed behind a door for resistance (Figure 1). Patients were provided with a personal exercise band for exercising at home and a brochure with instructional notes and illustrations. The patients were randomized to one of three weekly exercise dosages: two, four or six sessions per week for twelve weeks. For all groups training comprised just the single knee-extensor strength exercise. Patients were instructed to perform the exercise in three sets of twelve repetitions at a load corresponding to twelve repetition maximum (RM) in each set with each repetition lasting eight seconds (concentric phase 3 s, isometric phase 1 s, eccentric phase 4 s) (Table 1). The rationale for prescribing one home-based exercise was that it is a simple and low-cost alternative to supervised exercise therapy programs. Further, it is pragmatic and time-saving, and therefore has the potential to facilitate adherence and mastery of the exercise while stressing the knee joint minimally.38–40 A BandCizer© sensor was attached to the exercise band to objectively assess exercise adherence.

The home-based knee-extensor exercise. The exercise band is fixed behind a door with an anchor. BandCizer© sensor technology was used to objectively assess exercise adherence.
Prescribed knee-extensor exercise dosages.
Outcome assessments and outcomes
Outcomes were assessed at four endpoints; at baseline (t0), after twelve weeks of home-based exercise/before surgery (t1), at hospital discharge (1-8 days after surgery) (t2) and three months after surgery (t3). Outcomes at endpoints t2 and t3 were only collected for patients that underwent surgery. The primary endpoint was after the exercise period (t1) and the secondary endpoints were just before hospital discharge (t2) and three months after surgery (t3). After the 12-week exercise period, at endpoint t1, each patient’s decision on surgery was re-evaluated in a shared decision-making process between the patient and orthopedic surgeon (i.e. continue with exercise therapy or schedule KR surgery). Outcome assessments were performed blinded by the primary investigator and a research assistant dedicated to the trial. Both were trained according to the trial outcome assessment protocol to ensure standardized assessments throughout the trial. Following outcome assessments, the data were entered in the browser-based research database Research Electronic Data Capture (REDCap 7.1.1) by blinded trial personnel. To ensure data validity, blinded double-data entry was used.
Primary outcome
The primary outcome was change in isometric knee-extensor strength from baseline to after the exercise period (t0-t1). Isometric knee-extensor strength was measured using a computerized strength chair (Good Strength Chair, Metitur Oy, Jyvaskyla, Finland), which is valid and reliable in the KR population.41 Five measurements of maximal isometric knee-extensor strength at 60° knee flexion were completed, separated by 60-s pauses. The patients were instructed to extend their knee as forcefully as possible with a gradual increase in force over a 5-s period while receiving strong standardized verbal encouragement. Isometric knee-extensor strength is expressed as the maximal voluntary torque per kilogram body mass (Nm/kg). The highest obtained value was used for analysis. Isometric knee-extensor strength was chosen as the primary outcome, as it is relevant to have an outcome closely related to the exposure when investigating a dose-response relationship, while also being an outcome that can mediate other health effects.42–44
Secondary outcomes
The secondary outcomes were change in isometric knee-extensor strength after surgery (t0-t2 and t0-t3), change in performance-based function comprising six-minute walk test (6MWT), stair climb test (SCT), current knee pain and average knee pain during the last week (0-10 NRS), self-reported disability; Knee Osteoarthritis Outcome Score (KOOS) and Oxford Knee Score (OKS), “need for surgery” and objectively measured exercise adherence (t0-t1, t0-t2 and t0-t3). Other outcomes were registration of adverse events and harms.
The “need for surgery” outcome was an assessment of the patients’ self-perceived need for surgery. After the 12-week exercise period at outcome assessment t1 the patients were asked by the outcome assessor: “Based on your knee symptoms in the last week would you say that you need knee surgery?” Three answer options were possible: 1) Yes, I believe I need surgery, 2) I do not know or 3) No, I do not believe I need surgery.
Exercise therapy adherence was objectively quantified using a sensor attached to the exercise band (BandCizer© sensor technology). The sensor collects and stores data on date, time, number of sets, number of repetitions and time-under-tension (TUT). The sensor technology has been reported to be valid and reliable for musculoskeletal conditions.45–47 In the present trial patients were defined as adherent if >75% of the prescribed exercise sessions were completed.
For detailed information on the secondary outcomes please see the protocol paper.34
Sample size
For the planned three-group one-way ANOVA analysis, a sample size of 126 patients (42 per group) was required to obtain a power of 80%. The a priori sample size calculation was based on a normal mean difference with a two-sided significance level of 0.05, a minimal clinical important difference of 0.15 Nm/kg (15%) and a common standard deviation of 0.22 Nm/kg in isometric knee-extensor strength.48 To allow for a dropout rate of 10%, a total of 140 patients were included in the intention-to-treat (ITT) analysis.
Randomization, sequence generation, allocation concealment mechanisms and implementation
The patients were randomly assigned to one of the three exercise groups (two, four or six sessions per week) by a 1:1:1 allocation ratio. The random allocation sequence was computer-generated by a statistician otherwise not involved in the trial in any way. One hundred and forty sequentially numbered sealed opaque envelopes were generated. When a patient had been included in the trial (signed written informed consent and completed baseline assessment) a research assistant independent of the trial opened an envelope and informed the patient’s municipality of the exercise group allocation. The random allocation sequence was stored on a secure password locked server only accessible by the research assistant independent of the trial.
Blinding
All outcome assessors and the data analysts were blinded to the exercise group allocation. At outcome assessments the assessors started by informing the patients not to mention their exercise dosage. For analysis the data was coded in such a way that group allocation was concealed blinding the data assessors and analysts to the patients’ allocation. The physiotherapists and patients were not blinded to the allocation due to the nature of the intervention, however the patients were blinded to the other exercise dosages and the study hypothesis.
Statistical methods
The primary intention-to-treat analysis tested the hypothesis that an exercise dosage of four knee-extensor strength sessions per week would elicit a greater change in isometric knee-extensor strength pre-operatively compared to two or six sessions per week. For all outcomes, between group contrasts were compared using repeated measures of variance (one-way ANOVA). Normality assumptions of the model residuals were checked to ensure that the underlying assumptions of the statistical model were met. Results are presented firstly as absolute changes (e.g. Nm/kg) and secondly, as relative changes (%) from baseline. Mean scores with ±SD, between group contrasts (change scores) with 95% CI and p-values for each outcome at each time-point across all three groups are reported. Descriptive statistics are presented as mean with ±SD. Normal distribution of data was checked by q-q plots and histograms. As supplementary analyses, simple regression models were performed using the pooled exercise adherence data across all three groups. The dependent variables were the primary and secondary outcomes and the independent variable was exercise adherence quantified in two ways: 1) as total number of completed exercise sessions and 2) as total time-under-tension (TUT) per patient. All analyses followed the ITT principle and to create full datasets, missing data were imputed using multiple imputation (100 imputation sets). Multiple imputation models were based on age, gender, group allocation and all previous scores in relevant outcomes. Missing data at the different time-points are presented in appendix 1. All analyses were performed blinded by the principal investigator and a statistician, and followed the pre-specified analysis plan.34 Analyses were performed in SAS Enterprise Guide version 7.1.
Results
Participant flow, Recruitment and Baseline data
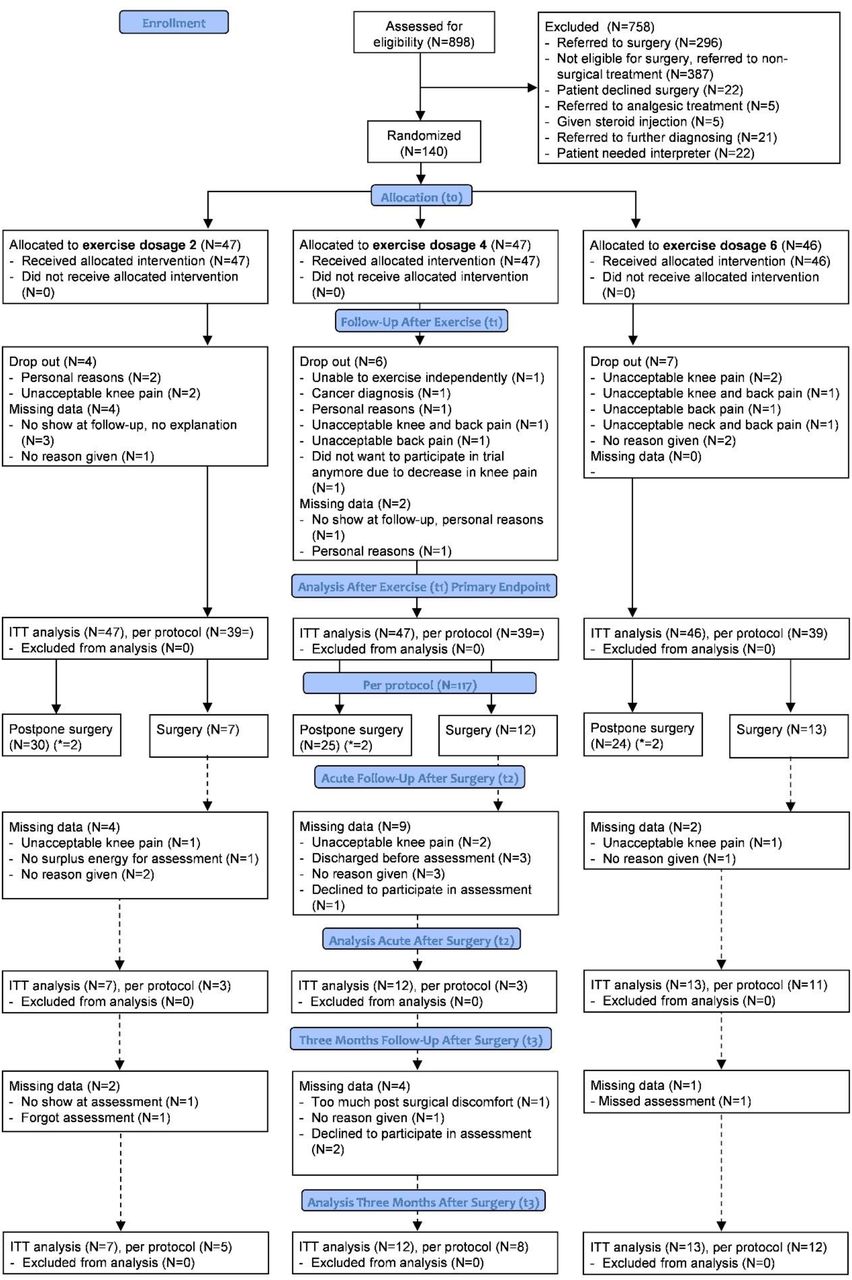
Between 25th October 2016 and 8th January, 2019, 898 patients potentially eligible for KR were assessed for eligibility. One-hundred and forty patients were included and randomized to an exercise dosage of 2 sessions/week, 4 sessions/week or 6 sessions/week (Figure 2, flow chart). Assessments at the primary endpoint (after 12 weeks of exercise [t1]) was completed for 117 patients with 39 in each group. At the two secondary endpoints, 32 patients were available for assessment. Assessments were completed for 17 patients acutely after surgery (t2) and for 25 patients three months after surgery (t3). Reasons for drop-out and missing data for each group are provided in figure 2. For the intention-to-treat analyses, 140 patients were included in the primary analysis (t0-t1) and 32 patients were included in the secondary analyses (t0-t2 and t0-t3). Baseline characteristics are provided in table 2 for the whole sample and for each group separately. The baseline characteristics were comparable between groups (no statistical hypothesis testing was undertaken as suggested by the CONSORT group).35 Separate baseline characteristics for the patients lost to follow-up and the remaining patients are provided in appendix 2.

Flow chart of each assessment time-point of the trial according to the CONSORT guidelines.35 ITT = intention-to-treat analysis. Dotted lines indicate assessment time-points after surgery. *6 patients (N=2/group) wanted surgery but had competing co-morbidities disqualifying them as candidates for surgery (Appendix 3).
Numbers analyzed, Outcomes and estimation and Ancillary analyses
The outcome scores for the primary and secondary outcomes at the primary endpoint (t1) are presented in table 3. Due to the large proportion of patients who postponed surgery after the exercise intervention, only 32 patients were available for the post-operative intention-to-treat analyses at the secondary endpoints; acutely after surgery (t2) and three months after surgery (t3). Separate baseline characteristics of the 32 patients who had surgery is presented in appendix 4. No between group differences for any outcomes were observed for the assessments at these endpoints (Appendix 5 and 6).
Mean change in all outcomes between baseline and following 12 weeks home-based exercise (t0-t1). Intention-to-treat analysis, N = 140. One-way ANOVA based on imputed data.
Assessment after exercise (primary endpoint (t1))
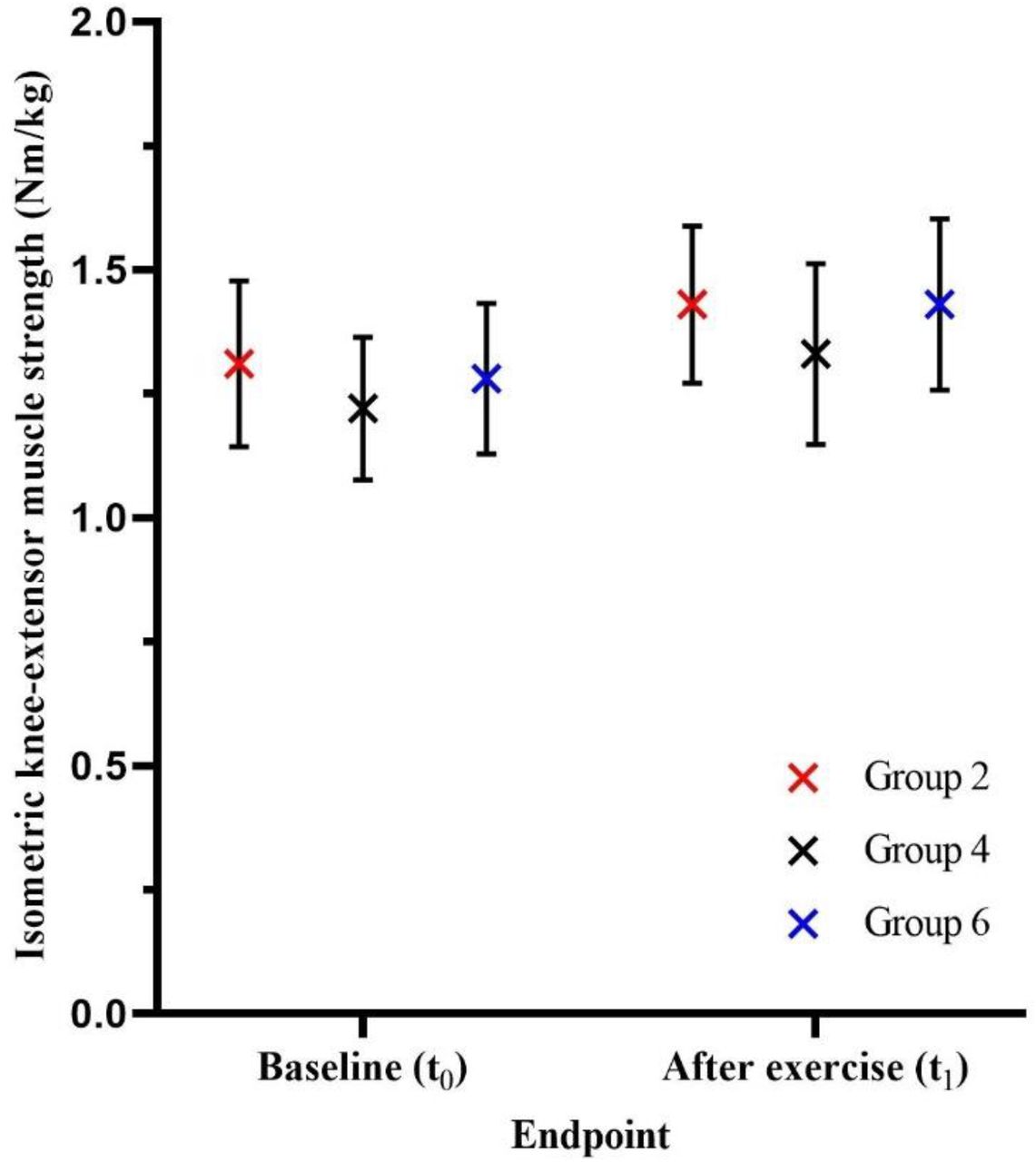
Primary outcome – Isometric knee-extensor strength (Nm/kg): The intention-to-treat analysis showed no difference between the three groups in change between baseline and following 12 weeks of exercise (primary endpoint (t0-t1)) in isometric knee-extensor muscle strength: group 2 vs. 4; 0.009 Nm/kg (0.1%) [95% CI−0.15 to 0.17], P=0.913, group 2 vs. 6;−0.03 Nm/kg (−2.6%) [95% CI−0.18 to 0.13], P=0.725 and group 4 vs. 6;−0.04 Nm/kg (−2.7%) [95% CI−0.20 to 0.13], P=0.668 (Figure 3). Within group changes between baseline and following 12 weeks of exercise showed an increase in isometric knee-extensor muscle strength for the whole sample and all three groups separately, though not statistically significant for group 4: whole sample; 0.13 Nm/kg (10.2%) [95% CI 0.07 to 0.19], P=<0.0001, group 2; 0.12 Nm/kg (9.2%) [95% 0.02 to 0.22], P=0.021, group 4; 0.11 Nm/kg (9.0%) [95%−0.01 to 0.23], P=0.064 and group 6; 0.15 Nm/kg (11.7%) [95% CI 0.04 to 0.25], P=0.007 (Table 3).

Isometric knee-extensor muscle strength (Nm/kg) at baseline (t0) and after twelve weeks of home-based knee-extensor exercise (t1) across the three groups. The X represents the mean value and the whiskers the corresponding 95% confidence intervals.
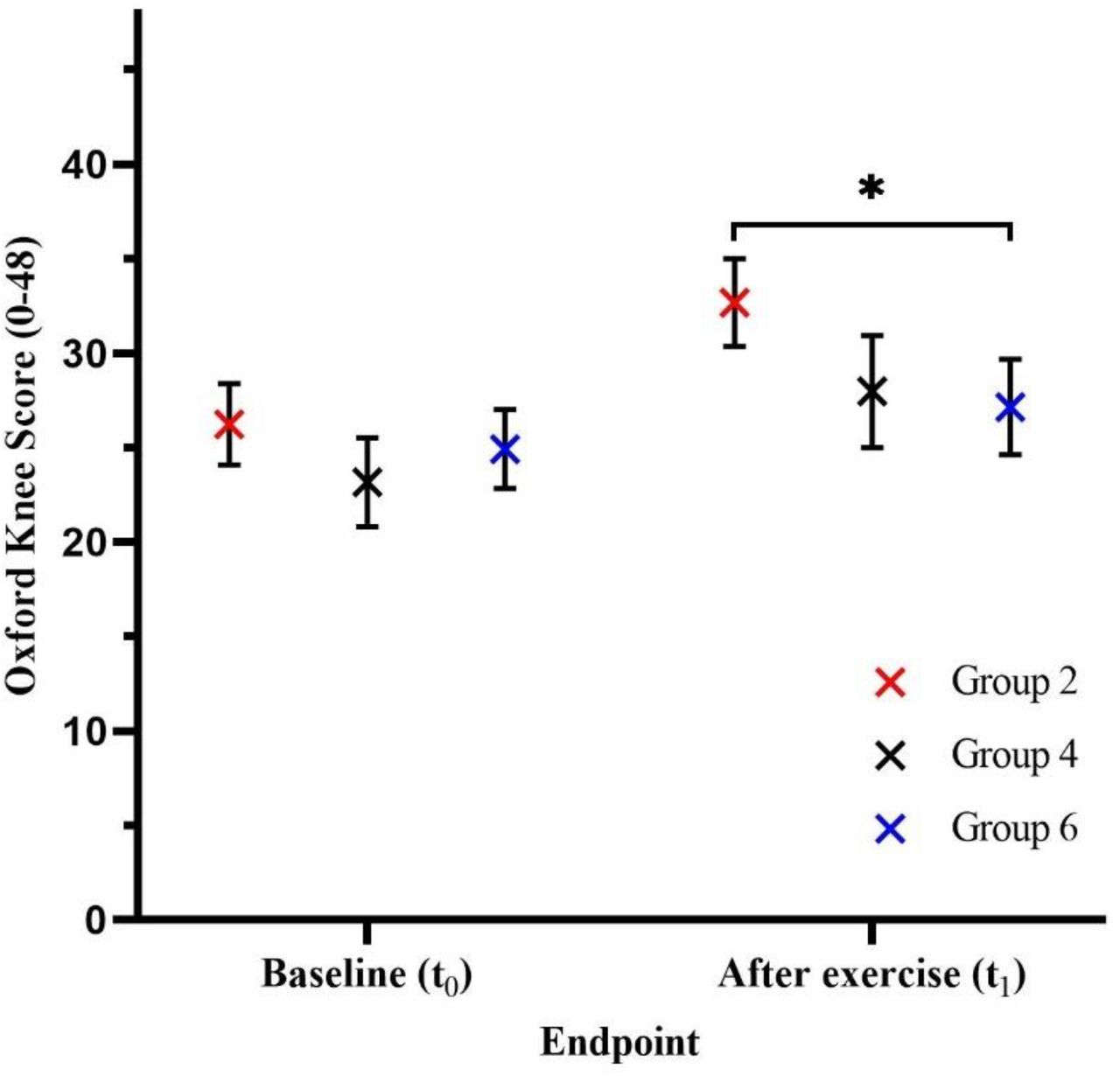
Secondary outcomes: The intention-to-treat analyses showed a significant difference in change between baseline and following 12 weeks of exercise between group 2 and 6 in favour of group 2 for Oxford Knee Score: 4.2 OKS points (15.2%) [95% CI 0.6 to 7.8], P=0.021 (Figure 4) and average knee pain last week (NRS 0-10):−1.1 NRS points (−19.5%) [95%−2.2 to−0.1], P=0.030 (Table 3). No between group differences were observed for any other group comparisons or secondary outcomes at the primary endpoint after 12 weeks exercise. Within group changes showed a positive change for the whole sample, and all three groups separately, for all secondary outcomes at the primary endpoint. Larger changes were observed in group 2 compared to group 4 and 6, and in group 4 compared to group 6. For the outcome “need for surgery”; 37 patients answered “Yes, I believe I need surgery”, 25 “I do not know” and 55 “No, I do not believe I need surgery”. For the distribution of answers between the three groups, see table 3.

Oxford Knee Scores at baseline (t0) and after twelve weeks of home-based knee-extensor exercise (t1) across the three groups. The X represents the mean value and the whiskers the corresponding 95% confidence intervals. *=change score for group 2 significantly higher than group 6 (P=0.021).
Treatment decision after exercise therapy
As a post hoc analysis, the number of patients who underwent surgery and those who postponed surgery were registered. Of the 117 patients with follow-up assessments after 12 weeks of exercise (Figure 2), 79 (67.5%) postponed surgery, 32 (27.4%) underwent KR, and 6 (5.1%) wanted surgery, but the orthopedic surgeon deemed this as contra-indicated due to co-morbidities (Appendix 3) (Table 4).
Exercise adherence
Data from 95 patients was available for the exercise adherence assessment. Of the 45 patients without available data, 23 did not complete the 12 weeks of exercise (dropped-out and missing data), 8 had less than 6 recorded exercise sessions and 14 had technical problems or lost the BandCizer© sensor. Exercise adherence was quantified as 1) total number of sessions and 2) total time-under-tension (TUT). When exercise adherence was quantified as total number of sessions both group 2 and 4 completed >75% of the prescribed dosage (84.8% and 81.9%, respectively) (Figure 5). When quantified as total time-under-tension (TUT) no groups completed >75% of the prescribed dosage. No between group differences were observed (Table 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adherence to prescribed exercise dosage across the three groups with exercise quantified as total number of exercise sessions. Circles represent the mean number of recorded exercise sessions for each patient. Red circles represent patients prescribed two exercise sessions per week. Black circles represent patients prescribed four exercise sessions per week. Blue circles represent patients prescribed six exercise sessions per week. The red dotted line represents the prescribed exercise dosage in group two (24 sessions). The black dotted line represents the prescribed exercise dosage in group four (48 sessions). The blue dotted line represents the prescribed exercise dosage in group six (72 sessions).
Supplementary analyses
For the supplementary regression analyses the three groups were pooled into one sample. No association was observed between the level of exercise adherence and pre-operative changes for any outcomes, except for a weak inverse association between total number of sessions and change in the six-minute walk test (Slope−0.7323 [95%−1.819 to−0.1826]) (Appendix 7).
Harms
A total of 14 adverse events were registered during the trial period. Exacerbated knee pain due to the exercise intervention was reported as the most frequent cause of harm (Table 7). See the flow chart for elaboration on the adverse events across the three groups (Figure 2).
Discussion (Generalizability, Interpretation)
The QUADX-1 trial found that none of the different prescribed knee-extensor exercise dosages (2, 4 and 6 sessions/week) in patients eligible for knee replacement were superior in improving isometric knee-extensor strength, while an exercise dosage of 2 exercise sessions/week seems superior to 6 sessions/week for Oxford Knee Score and average knee pain last week (0-10 numeric rating scale). Furthermore, independent of exercise dosage, only one in three patients completing the exercise therapy intervention decided to undergo surgery for their knee OA.
The results of the present trial are relevant for the following reasons. Firstly, larger exercise dosages do not seem to be more effective than smaller.49 Secondly, an exercise intervention with one home-based exercise can lead to clinically relevant improvements in symptoms comparable to more comprehensive interventions in patients eligible for knee replacement.22,49,50 Finally, a simple exercise therapy intervention using only one exercise, in a model of coordinated care, can prompt the majority of patients eligible for knee replacement to postpone surgery.
Decision on surgery – Coordinated non-surgical and surgical care
The large number of patients who postponed surgery highlights the importance of coordinating non-surgical and surgical care in patients eligible for knee replacement. The proportion of patients postponing and choosing surgery across the three groups was similar – indicating that the decision to postpone surgery is independent of prescribed exercise therapy dosage. This also fits the general pattern of comparable improvements in all three dosage groups. A contributing factor explaining the large number and similar distribution of patients postponing surgery among the three groups could be the non-specific effect of the applied ‘model’ of coordinated non-surgical and surgical care.16,51–53 In this ‘model’, the patients’ decision on surgical treatment was re-evaluated, following exercise therapy, by the patient and their orthopedic surgeon. This re-evaluation of treatment after exercise therapy, based on change in knee OA related symptoms, combined with additional attention from an orthopedic surgeon could facilitate the patients’ decision to postpone surgery.54–57 This is exemplified in table 5 showing that patients who believe they need surgery, undergo surgery, while those who “don’t know” or do not believe they need surgery postpone it. We do not know if or when the QUADX-1 trial participants who postponed surgery will undergo surgery, something of great interest to clinicians,58 but we will follow this cohort of patients and report findings in the future.
Using exercise therapy in the care pathway to evaluate the need for surgical care challenges the current premise for exercise therapy before surgery (exercise-based pre-habilitation) in the Enhanced Recovery After Surgery (ERAS) concept where it is assumed that exercise therapy before planned surgery is always followed by surgery.59–63 Instead of being a predetermined care pathway (leading to surgery), exercise therapy before potential surgery could be used to inform the shared decision-making process when planning a care pathway.8,17,18 A more optimal way of coordinating the two treatment options, exercise therapy before potential surgery and knee replacement, could be to incorporate the effect of exercise therapy to further inform the shared decision-making. In this way patients without an acute need for surgery can be screened, and untimely surgery with potential complications avoided – something which is not possible at a one-time outpatient consultation. A care pathway in which exercise therapy is employed prior to knee replacement complies with guideline recommendations while also being cost-effective.5–10,64 We have previously argued that the premise for exercise therapy before potential surgery to enhance post-operative outcomes in patients eligible for knee replacement should be questioned33 as several systematic reviews conclude no clinically relevant effect.33,65–74 In line with this and based on the results from the QUADX-1 trial, we suggest the use of exercise therapy within the ERAS concept is to “pre-evaluate” to promote shared decision-making in an enhanced care pathway for patients with severe knee OA rather than to “prepare” patients for surgery. However, a prerequisite for successful coordination of care is that the involved healthcare professionals trust in the effectiveness and legitimacy of the different treatment modalities available, i.e. exercise therapy and surgery.13,58,75,76
Implications for one home-based exercise
The results from the QUADX-1 trial suggest no dose-response relationship between the prescribed knee-extensor exercise dosages and change in outcomes. In fact, the lowest dosage seems to have the largest effect on patient-reported outcomes. Interestingly, results from the QUADX-1 trial are comparable to other trials reporting similar proportions of patients who postpone surgery and corresponding clinically relevant improvements in patient-reported outcomes after exercise therapy.50,77 Compared to the intervention in the QUADX-1 trial, the exercise therapy interventions in these trials are more comprehensive and costly, comprising more exercises and supervision. This suggests that the intervention and associated exercise dosage needed to improve symptoms in patients eligible for knee replacement does not necessarily have to be either extensive or comprehensive.49 This corresponds well to the results from the supplementary regression analyses and our recent meta-regression analysis indicating no dose-response between prescribed pre-operative knee-extensor exercise dosage and change in outcomes before scheduled knee replacement – although this was not a randomized comparison.33 The objective assessment of exercise adherence showed that group 2 exercised half as much as group 4 and 6 (total sessions and TUT). This further supports the finding of no dose-response relationship, and that even small exercise dosages for this patient population may result in improved outcomes.
In general, patients in the QUADX-1 trial improved knee function and patient reported outcomes – suggesting that exercise therapy, and not dosage, is the most important element in improving these outcomes for patients eligible for knee replacement. A potential explanation for this is that patients eligible for knee replacement have an inactive lifestyle due to their knee condition.78,79 An inactive lifestyle can lead to decreased physical ability and muscle strength leaving a large potential for improvement with exercise therapy.43,80–82 Thus, patients eligible for knee replacement might not need large exercise dosages to improve their symptoms.43,49,83 This suggests that one well-instructed home-based knee-extensor exercise is a viable treatment alternative to supervised exercise for patients with severe knee OA. For example, for patients who have a busy daily schedule, patients who live far from a clinic and patients who cannot afford or are not interested in attending formal group exercise sessions at a clinic at fixed times.26
Limitations
The trial was designed without a non-exercise comparator, so we do not know how patients would respond to the intervention without an exercise component. It is well established, however, that patients with knee OA benefit from exercise compared to non-exercise controls.7 The Danish healthcare system is publicly funded and treatment is therefore free. Refusing surgery after having been on a waiting list does not postpone the possibility of surgery for years. The patients can be re-assessed by an orthopaedic surgeon within months and have surgery scheduled if needed. This might limit the comparability to other countries with a different healthcare system.
Conclusion
Knee-extensor strength increased with both 2, 4 and 6 exercise sessions per week but none of the prescribed exercise dosages were superior to each other for the primary outcome isometric knee-extensor strength after 12 weeks. Two home-based knee-extensor exercise sessions a week seems superior to six for patient-reported outcomes, and across exercise dosages, only one in three patients decided to have surgery after the coordinated home-based exercise intervention. We suggest using a model of coordinated non-surgical and surgical care to improve the decision on surgery for patients eligible for knee replacement. Exercise before potential surgery should be used to evaluate the need for surgery and not to change outcomes after surgery in this patient population.
Data Availability
The raw data is available by contacting the corresponding author Rasmus Skov Husted via email: rasmus.skov.husted{at}regionh.dk
Other information
Registration
ClinicalTrials.gov identifier: NCT02931058, pre-registered October 10th, 2016.
Protocol
Open access Protocol PubMed (PMID: 29347947).34
Funding
This work was supported by grants from The Capital Region’s strategic funds (R142-A5363), The Capital Region’s foundation for cross-continuum research (P-2015-1-01, P-2018-1-02, P-2019-1-03), The Danish Rheumatism Association (R156-A4923) and Copenhagen University Hospital Amager-Hvidovre’s strategic funds (2019-800). The funding sources had no role in this work.
Acknowledgements
Acknowledgement go to: Research assistant Line Holst for help with trial management and outcomes assessment, and to the physiotherapists in the participating municipalities (Broendby, Hvidovre and Copenhagen) and the orthopedic surgeons at the Orthopedic Department at Copenhagen University Hospital, Hvidovre.
Appendix
Assessment after surgery (secondary endpoints [t2 and t3])
Footnotes
E-mail addresses: AT (a_troelsen{at}hotmail.com), HH (henrik.husted{at}regionh.dk), BG (birk.mygind.groenfeldt{at}regionh.dk), KT (kristian.thorborg{at}regionh.dk), TK (thomas.kallemose{at}regionh.dk), MSR (misr{at}hst.aau.dk), TB (thomas.quaade.bandholm{at}regionh.dk)
References



