
Abstract
Background Isolated REM sleep behavior disorder (iRBD) is the most specific prodromal marker of Parkinson’s disease (PD), often accompanied by various non-motor symptoms. In PD, non-motor symptoms are strongly associated with reduced health-related quality of life (hrQoL).
Objectives To identify factors linked to poorer hrQoL in patients with iRBD and to compare their hrQoL to healthy control participants (HC) and patients with PD.
Methods Sixty-two patients with iRBD (M = 66.44±6.14), 29 patients with PD (M = 67.21±7.23), and 19 HC (M = 67.57±8.16) were included. We administered the 36-Item Short Form Health Survey (SF-36) to assess hrQoL. Additionally, participants underwent a comprehensive clinical evaluation of non-motor symptoms.
Results The SF-36 total score was significantly lower in patients with iRBD (83.33±16.96) compared to HC (92.29±5.49, U = 390.00, Z = −2.218, p = .027, r = 0.246). Poorer hrQoL in patients with iRBD was linked to self-reported neuropsychiatric symptoms, sleep-wake disturbances, and a higher burden of autonomic symptoms (all r = -.25 to -.76, all p < .05). Multiple regression analysis revealed fatigue and depressive symptoms as significant predictors of poorer hrQoL in patients with iRBD (F (5.56) = 51.59, p < .001, adjusted R2 = 0.81).
Conclusions This study highlights the importance of non-motor symptoms for hrQoL in prodromal PD, irrespective of motor symptoms. Fatigue and depressive symptoms arise as the most relevant therapeutic targets in the prodromal stage of PD to optimize the patient’s quality of life.
1 Introduction
Isolated rapid eye movement (REM) sleep behavior disorder (iRBD) is a parasomnia defined by dream-enacting behavior and a loss of muscle atonia during REM sleep1,2. Compelling evidence identified iRBD as an incipient α-synucleinopathy3–5. To date, iRBD is the most specific prodromal marker of Parkinson’s disease (PD) and can precede the onset of PD-defining motor symptoms up to decades6,7.
By definition, patients with iRBD do not exhibit severe motor symptoms, but mild motor disturbances can be observed8–10. In contrast, non-motor symptoms such as constipation, olfactory dysfunction, and depressive symptoms are frequent in iRBD11. A recent systematic review and meta-analysis reported a prevalence of depression in patients with iRBD of 28.8% and an odds ratio for depression of 2.5712, indicating disturbed mental well-being in prodromal PD.
Health-related Quality of Life (hrQoL) is increasingly recognized as the essential factor for the impact of a disease on a patient’s life. In PD, a significantly lower hrQoL compared to HC has been reported13. Interestingly, the burden of non-motor symptoms in PD, particularly depressive symptoms, showed a stronger association with hrQoL than motor symptoms13,14. Data on hrQoL in iRBD are scarce, and only one study assessed hrQoL in iRBD, showing reduced hrQoL in iRBD patients compared to HC15. Moreover, identifying factors associated with reduced hrQoL is vital, particularly in prodromal PD, as it may help develop therapeutic interventions to restore hrQoL without disease-modifying agents.
It is, therefore, of broad clinical interest to understand which symptoms arising in the prodromal stage of PD are linked to hrQoL. In the present study, we studied hrQoL in patients with iRBD compared to HC and patients with PD, and its relation to emerging motor symptoms and a variety of non-motor symptoms. We hypothesized that hrQoL is diminished in patients with iRBD compared to HC but still better than in PD. Comparable to PD, non-motor symptoms may contribute to poorer hrQoL in patients with iRBD beyond demographic variables and subtle motor symptoms.
2 Materials and Methods
2.1 Study design and participants
Participants were recruited from July 2020 to November 2021 at the University Hospital of Cologne from our ongoing iRBD discovery cohort16. Inclusion criteria for patients with iRBD were age 50 to 80 years, the ability to give informed consent, and polysomnography-confirmed iRBD according to the International Classification of Sleep Disorders III criteria1,16. The exclusion criterion was a significant cognitive impairment operationalized by the Montreal Cognitive Assessment (MoCA; cutoff <22)17. We also included patients with PD diagnosed according to the current consensus criteria18 with identical in- and exclusion criteria. For HC, depressive symptoms operationalized by the Beck’s Depression Inventory II (BDI-II; cutoff ≥9)19 and symptoms of RBD or any movement disorder were additional exclusion criteria. Patients with PD and HC were recruited from other studies of the investigators.
All subjects gave written informed consent prior to participation. The local ethics committee of the Medical Faculty of the University of Cologne approved the study.
2.2 Assessment of health-related quality of life
HrQoL was measured with the 36-Item Short Form Health Survey (SF-36)20, a cross-disease patient-reported health status survey. A systematic review including 29 studies showed that the SF-36 questionnaire is the most frequently used generic assessment to estimate hrQoL in PD13. As the SF-36 is not disease-specific, it is better suited to investigate hrQoL in the prodromal stage of PD than PD-specific hrQoL questionnaires, which typically focus on motor-related symptom burden. The questionnaire consists of 36 items assessing eight hrQoL domains: physical function, role limitations due to physical problems (physical role), bodily pain, general health, vitality, social functioning, role limitations due to emotional problems (emotional role), and psychological well-being. Most questions use Likert scaling, but several subitems have a dichotomous (yes/no) format. The questionnaire is scored by recoding item responses first and subsequently averaging items of one domain to create the eight SF-36 domain scores. The total score indicates the arithmetic average of all domain scores. Domain scores and the total score range from 0 to 100, with higher scores indicating better hrQoL.
2.3 Clinical Assessment
Subjects completed questionnaires on various non-motor symptoms. Sleep quality was evaluated by the Pittsburgh Sleep Quality Index (PSQI)21. Cognitive, emotional, and behavioral features of psychophysiological insomnia were measured by the Regensburg Insomnia Scale (RIS)22. The Epworth Sleepiness Scale (ESS)23 interrogates daytime sleepiness. Presence and severity of anxiety were determined using Beck’s Anxiety Inventory (BAI)24, and depressive symptoms were assessed with the BDI-II25. Apathy was assessed by the Apathy Evaluation Scale (AES)26, and fatigue was examined by the Fatigue Scale for Motor and Cognitive Functions (FSMC)27. Subjective cognitive impairment (SCI) was measured by an extended version of the Subjective Memory Impairment Questionnaire (SMI-Q)28,29. We assessed the SCOPA-AUT30 questionnaire to examine autonomic symptoms and the non-motor symptom questionnaire (NMSQ)31 for non-motor symptoms in general. For all questionnaires, higher total scores indicate a higher symptom burden.
All participants underwent a comprehensive clinical work-up including the 12-item Sniffin’ Sticks test (Burkhardt®, Wedel, Germany), cognitive screening with the MoCA17, and motor symptoms were quantified with part III of the MDS-UPDRS32 (except for HC participants).
2.4 Statistical analyses
Statistical analyses were conducted using SPSS version 28.033 and R Studio34. The normality of data was assessed with Shapiro-Wilk and Kolmogorov-Smirnov tests and Q-Q plots. As all data were not normally distributed. The Kruskall-Wallis test was used to assess group differences (iRBD, HC, PD). Post-hoc tests were performed using Mann-Whitney-U tests. A chi-Square test was performed to interrogate categorical variables. The relationship between hrQoL and non-motor symptoms and clinical and demographic data was analyzed with Spearman partial correlations, including age and sex as covariates. Based on a significant correlation in the bivariate partial correlation analyses (p < .05), non-motor symptom scales were selected as potential determinants of hrQoL in multiple linear regression analyses for the subgroup of patients with iRBD. PSQI, RIS, ESS, BAI, BDI-II, AES, FSMC, SCI, SOPA-AUT, and NMSQ were included as independent variables in a stepwise regression approach. The SF-36 total score and the eight SF-36 domain scores were used as dependent variables. All regression models included age and sex as covariates. The significance level was set at p < .05 uncorrected.
2.5 Data Availability Statement
The data included in this study are available on reasonable request to the corresponding author.
3 Results
Sample Characteristics
The analyses included sixty-two patients with iRBD, 19 HC participants, and 29 PD patients. Patients with iRBD were comparable concerning age and sex to both other groups. Patients with iRBD were aged 54 to 78 years (66.44 ± 6.14), 54 of whom were male (87%), and none reported any relevant motor impairment during daily routine. Demographic and clinical characteristics are shown in Table 1.
Significant group differences were observed for PSQI (H(2) = 13.54, p = .001), RIS (H(2) = 14.07, p = .001), ESS (H(2) = 19.34, p < .001), and FSMC (H(2) = 25.95, p < .001). Post-hoc analysis revealed no significant differences between HC and iRBD. Nevertheless, both HC and iRBD exhibited significantly lower scores when compared to PD. Further significant group differences were observed for BAI (H(2) = 28.40, p < .001), BDI (H(2) = 22.78, p < .001), SCI (H(2) = 16.60, p < .001), SCOPA-AUT (H(2) = 27.87, p < .001), and NMSQ (H(2) = 34.77, p < .001). Post-hoc tests indicated significantly higher values in patients with iRBD than HC but lower than in PD. In addition, AES (H(2) = 9.82, p = .007) differed significantly between groups. Post-hoc tests showed no differences between iRBD and PD. However, both iRBD and PD displayed significantly higher scores when compared to HC.
Health-related quality of life in iRBD compared to PD and HC
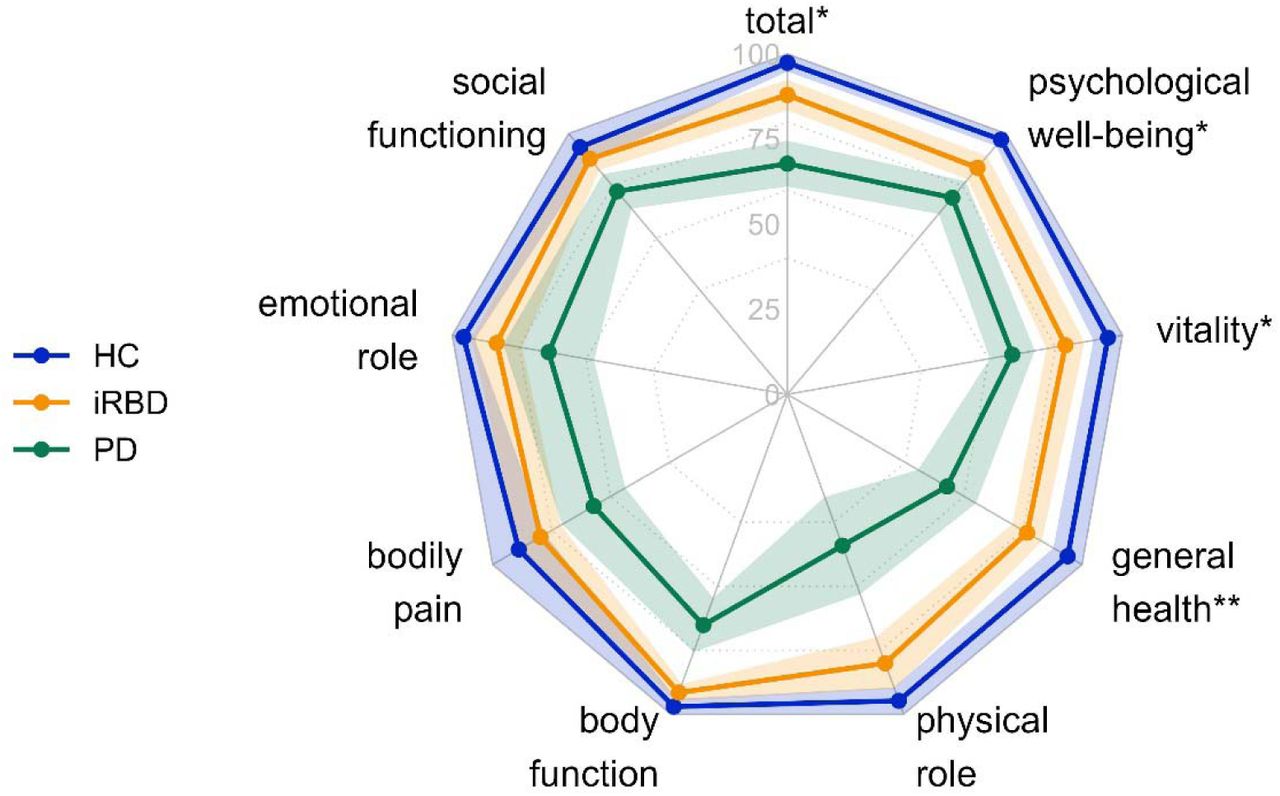
A Kruskal-Wallis test revealed significant group differences in the SF-36 total score (H(2) = 35.32, p < .001). HC participants had a significantly higher SF-36 total score than patients with iRBD (U = 390.00, Z = −2.218, p = .027, r = 0.246), but patients with PD had a significantly lower SF-36 total score compared to iRBD (U =323.50, Z = −4.902, p < .001, r = 0.514) and HC (U = 30.00, Z = −5.176, p < .001, r = 0.747). Furthermore, there were significant differences between patients with iRBD and HC in the SF-36 domains general health (U = 346.00, Z = −2.720, p = .007, r = 0.302), vitality (U = 402.00, Z = −2.096, p = .036, r = 0.233), and psychological well-being (U = 375.50, Z = −2.414, p = .016, r = 0.268, see Figure 1). HrQoL in PD was significantly lower than in patients with iRBD and HC in all SF-36 domains (all U = 37.00 to 673.50, all Z = −5.056 to 2.606, all p < .01, all r = 0.273 to 0.730).

Note. N = 110. Dots express mean values, and colored areas show 95% confidence intervals. HC = Healthy control participants (n = 19); iRBD = iRBD patients (n = 62); PD = PD patients (n = 29). SF-36 scores range from 0 to 100, with higher scores indicating better hrQoL. * p < .05, ** p < .01. Asterisks indicate significant group differences between HC and iRBD in the post-hoc Mann-Whitney-U tests. All group differences between iRBD and PD were significant (all p < .01).
Factors associated with health-related quality of life in iRBD
To analyze relevant factors linked to HrQoL in patients with iRBD, we correlated HrQoL domains and the SF-36 total score with outcomes of the clinical and non-motor assessment. Most prominently, we observed a close link between pronounced neuropsychiatric symptoms and reduced hrQoL in various domains. When correcting for age and sex with partial correlation analysis, PSQI, RIS, ESS, BAI, BDI-II, AES, FMSC, SCI, SCOPA-AUT, and NMSQ scores were negatively correlated with hrQoL in patients with iRBD (all r = -.25 to -.76, all p < .05, see Figure 2). MoCA was positively correlated with vitality in patients with iRBD (r = .25, p = .039). Interestingly, incipient motor symptoms were not associated with hrQoL in patients with iRBD (all r = -.02 to -.12).

{kind=link}
{kind=link}
Note. N = 62. The significance level for all Spearman partial correlations was set to .05. Bigger dots indicate more significant correlations, with blue-colored dots showing negative correlations and red-colored dots illustrating positive correlations. MDS-UPDRS-III = MDS-Unified Parkinsońs Disease Rating Scale Part III; MoCA = Montreal Cognitive Assessment; PSQI = Pittsburgh Sleep Quality Index; RIS = Regensburg Insomnia Scale; ESS = Epworth Sleepiness Scale; BAI = Beck Anxiety Inventory; BDI-II = Beck Depression Inventory II; AES = Apathy Evaluation Scale; Fatigue = Fatigue Scale for Motor and Cognitive Functions; SCI = Subjective Cognitive Impairment; SCOPA-AUT = Scales for Outcomes in Parkinsońs Disease - Autonomic questionnaire; NMSQ = Non-Motor Symptoms Questionnaire.
Based on the significant bivariate correlation analyses (p < .05), PSQI, RIS, ESS, BAI, BDI-II, AES, FMSC, SCI, SCOPA-AUT, and NMSQ were selected as potential candidates for the multiple linear regression analyses. The adjusted R2 of the multiple regression analyses controlling for age and sex using a stepwise approach to evaluate the independent influence of the clinical scales ranged from .345 to .805. PSQI, RIS, AES, and NMSS were each a predictor of singular SF-36 domains: total score, body role, vitality, and emotional role, respectively (see Table 2). However, fatigue and depressive symptoms were significant determinants of a large set of hrQoL subdomains of the SF-36.
4 Discussion
This study identified reduced hrQoL in patients with iRBD independent of emerging PD motor symptoms. In particular, hrQoL was lower in patients with iRBD than HC in the SF-36 total score and the domains general health, vitality, and psychological well-being. In line with the affected hrQoL domains, diminished hrQoL in patients with iRBD was primarily correlated with more self-reported neuropsychiatric symptoms, sleep-wake disturbances, and autonomic symptoms. Multiple regression analyses revealed that significant factors linked to poorer hrQoL in patients with iRBD were more severe fatigue and depressive symptoms.
In patients with PD, sleep-wake disorders, including insomnia and excessive daytime sleepiness, are prevalent comorbidities closely related to poorer hrQoL35. Similarly, fatigue is reported by approximately half of the patients with PD36,35,37 and is associated with an increased α-synuclein oligomer level in the cerebrospinal fluid38. Lintel et al.39 argue that symptoms of fatigue overlap with the diagnostic criteria for depression and hence challenging to separate. This thinking aligns with our results that identify these two symptoms as the most significant factors associated with poorer hrQoL in patients with iRBD. Patients with iRBD reported more autonomic symptoms than HC but fewer than patients with PD. This finding indicates that non-motor symptoms, including autonomic complaints, may precede motor symptoms in emerging PD11,40. Other studies in PD patients support our results showing a pronounced link between non-motor symptoms and reduced hrQoL13,14,35.
Psychological well-being emerges as the most influential factor affecting self-reported hrQoL in prodromal PD. Depressive symptoms, in particular, have also been shown to be the most substantial contributor to hrQoL in patients with PD and are a well-known feature of prodromal PD41,42,12. Hence, clinicians should be highly attentive to these symptoms when assessing patients with (prodromal) PD. In line with our study, motor symptoms are less associated with poor hrQoL in patients with PD14, affirming the importance of non-motor symptoms for hrQoL in (prodromal) PD, irrespective of motor symptoms.
Strikingly, non-motor symptoms of patients with iRBD and PD are often overlooked and rarely treated in the clinical routine43,44. A study by Shulman et al.44 revealed that physicians were least sensitive to symptoms of fatigue in patients with PD. As a result, this clinically relevant symptom is at risk of being neglected. It is, however, essential to assess non-motor symptoms as this study underpins the impact on hrQoL in early disease stages. A positive correlation between non-motor symptom severity and a physician’s diagnostic sensitivity44 implies that patients with iRBD in the prodromal phase of PD might not receive treatment for their symptoms as they might still be mild. However, adequate treatment of non-motor symptoms is crucial due to the close link to increased functional disability, cognitive impairment, caregiver burden, and poor subjective hrQoL45,46.
Careful assessment of non-motor symptoms in patients with iRBD may also open the opportunity for treatment options for patients in the context of a missing disease-modifying therapy. This aspect is of utmost importance in the context of ethical considerations regarding an early diagnosis of PD – especially in its prodromal stage47–49. In a retrospective survey, most patients with PD were skeptical about early risk disclosure given missing pharmacological options50. However, a recent study by Pérez-Carbonell and colleagues demonstrated that most patients with iRBD appreciated an honest risk disclosure at the time of iRBD diagnosis51. Patients with early PD, who remained untreated, showed a decline of hrQoL over the next 18 months, whereas patients with initiated treatment showed a trend towards better hrQoL52. Together with our study linking reduced hrQoL to treatable neuropsychiatric non-motor symptoms in prodromal PD, this disease phase should not be solely regarded as a phase of watchful waiting but point physicians to provide adequate and prompt medical care to restore hrQoL.
A limitation of our study is the lack of longitudinal data. Additionally, the study was conducted in recently diagnosed “de novo” patients with iRBD. As a result, the self-reported depressive symptoms may have been aggravated due to the recent diagnosis16,53. Also, sample sizes regarding the PD and HC participants were relatively small. Still, a considerable advantage of the current study is the possibility to compare HC, patients with iRBD, and patients with PD to assess hrQoL across healthy aging, prodromal and manifest PD. Another strength of the present study is the well-characterized sample due to the comprehensive clinical assessments. Our results warrant further analysis of hrQoL in iRBD in larger data sets.
In summary, in clinical practice, careful screening for non-motor symptoms in patients with iRBD is crucial as present non-motor complaints might complicate diagnosis and treatment. Depressive symptoms, particularly fatigue, are the most relevant therapeutic targets in the prodromal stage of PD to enhance patients’ quality of life. Various treatment options for non-motor symptoms are available and their use is likely to increase patients’ well-being.
Authors’ Roles
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical analysis: A. Design, B. Execution, C. Review and critique; (3) Manuscript: A. Writing of the first draft, B. Review and critique.
S.R.: 2A, 2B, 3A
M.-S. L.: 1B, 1C, 3B
A.S.: 1B, 1C, 3B
J.K.: 1B, 1C, 3B
K.-L.W.: 2C, 3B
C.E.J.D.: 1A, 1B, 1C, 2C, 3B
G.R.F.: 1A, 2C, 3B
A.O.: 2A, 2B, 3B
M.S.: 1A, 1B, 1C, 2A, 2C, 3A
Financial Disclosures of all authors (for the preceding 12 months)
S.R., M.-S.L., A.S., J.K. and K.-L.W. report no disclosures. C.E.J.D. received grants from the Clinician Scientist Program (CCSP), funded by the German Research Foundation (DFG, FI 773/15-1). G.R.F. receives royalties from the publication of the books Funktionelle MRT in Psychiatrie und Neurologie, Neurologische Differentialdiagnose, and SOP Neurologie and received honoraria for speaking engagements from Forum für medizinische Fortbildung FomF GmbH as well as grants from Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), Project-ID 431549029, SFB 1451. A.O. received a grant from the Koeln Fortune Program (grant-no. 329/2021), Faculty of Medicine, University of Cologne, and the “Novartis-Stiftung für therapeutische Forschung”, both outside the submitted work. M.S. received grants from the Else Kröner-Fresenius-Stiftung (grant number 2019_EKES.02), and the Koeln Fortune Program, Faculty of Medicine, University of Cologne. M.S. receives funding from the program “Netzwerke 2021”, an initiative of the Ministry of Culture and Science of the State of Northrhine Westphalia. The sole responsibility for the content of this publication lies with the authors.
Funding agencies
S.R., M.-S.L., A.S., J.K., and K.-L.W. report no disclosures. C.E.J.D. is supported by the Clinician Scientist Program (CCSP), funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation, FI 773/15-1). G.R.F. receives royalties from the publication of the books Funktionelle MRT in Psychiatrie und Neurologie, Neurologische Differentialdiagnose, and SOP Neurologie and received honoraria for speaking engagements from Forum für medizinische Fortbildung FomF GmbH as well as grants from Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), Project-ID 431549029, SFB 1451. A.O. received a grant from the Koeln Fortune Program (grant-no. 329/2021), Faculty of Medicine, University of Cologne, and the “Novartis-Stiftung für therapeutische Forschung”, both outside the submitted work. M.S. received grants from the Else Kröner-Fresenius-Stiftung (grant number 2019_EKES.02), and the Koeln Fortune Program, Faculty of Medicine, University of Cologne. M.S. receives additional funding from the program “Netzwerke 2021”, an initiative of the Ministry of Culture and Science of the State of Northrhine Westphalia. The sole responsibility for the content of this publication lies with the authors.
Acknowledgments
We thank all study participants for their participation.
References



