
ABSTRACT
Introduction Suicide is one of the leading causes of preventable death worldwide. Evidence reported in the literature seems to support the impact of providing active contact for people that have attempted suicide. The current systematic review and meta-analysis aim to investigate the effects of suicide prevention strategies implemented through remote and synchronous technology-based interventions.
Methods The systematic review and meta-analysis followed the PRISMA 2020 guidelines. The searches were conducted in PubMed, PsycInfo, Scopus, and Web of Science. Screening, selection process, data extraction, and risk of bias (RoB) assessment have been performed independently by two reviewers. A systematic review and narrative synthesis of the data has been performed. Data on adherence to treatment and suicide-related factors to explain heterogeneity were extracted. A meta-analysis was conducted to determine effect sizes (Hedge’s g) for suicidal ideation, odds ratios (OR) and 95% confidence intervals (95% CI) for lethal and non-lethal suicide behaviours. Data were pooled using a random-effects model. Subgroup analyses were performed by classifying the studies according to the evaluation period.
Results A total of 26 publications were finally included. Synchronous remote-based interventions were effective in preventing repeated suicide attempts (OR = 0.75; 95% CI 0.62 – 0.90) and suicide deaths (Peto OR = 0.37; 95% CI 0.18 – 0.77); however, considerable heterogeneity was reported. The effects on suicidal ideation were not confirmed (Hedge’s g = 0.23; 95% CI −1.54 – 1.07).
Conclusions The observed heterogeneity suggests that the effects should be considered under caution. Methodological and procedural guidelines are proposed to improve the quality of future research studies.
INTRODUCTION
The World Health Organization (WHO) estimates that over 703,000 people die annually from suicide worldwide [1, 2]. Suicide is a complex behaviour with multiple etiological factors that has become a serious public health problem. Every suicide is a major grievous blow that affects families, communities and entire countries and has lasting effects on the people left behind [1]. Suicide occurs across the lifespan; although, in 2019, it was the fourth leading cause of death among individuals aged 15-29 years worldwide [2, 3]. For each death by suicide, there are twenty suicide attempts [4], which is one of the major disease burden causes in the world [5, 6, 7]. Moreover, a history of suicide attempts is considered a robust predictor of completed suicide, supporting prevention efforts during the acute period following an episode of suicidal behaviour [8, 9, 10, 11].
Suicide prevention is emerging as a priority for the public health system [12]. Increasing evidence in the literature suggests that post-discharge follow-up contacts can be an effective suicide prevention strategy [13–17]. Information and communication technology-based interventions (ICT) have created opportunities and challenges in prevention, research, and clinical practice. Brief Intervention and Contact (BIC), 24/7 hotlines, letter/postcard delivery, or telephone follow-up have been classified as active contact interventions to prevent repeat suicidal behaviour in patients admitted to an Emergency Department (ED) [18, 19]. There is a wide range of eHealth-based treatments that are commonly classified into two categories: real-time synchronous therapy – such as telephone contact or telepsychiatry via videoconferencing – or digital self-help programs without human guidance, often asynchronous [20, 21].
An essential component of the effects of suicide prevention interventions is adherence to treatment, a factor at the core of mental health care [22]. The evaluation of therapeutic adherence in clinical care is critically important since poor adherence results in adverse outcomes, such as relapses and hospitalizations, among people with mental health disorders worldwide [22, 23, 24]. The multivariate character of treatment adherence has been emphasized in the literature as a facilitator for optimizing the benefits of all current therapies [22]. Accordingly, most post-discharge suicide prevention programmes reinforce contact with mental health professionals. Brief contact interventions have three rationales: first, allows for repeated suicide risk assessments; second, reduce feelings of social isolation and provide emotional support; third, improve adherence to treatment and reduce dropout from mental health care [25–28]. In recent decades, studies have been published with promising results implementing follow-up contact interventions for at-risk individuals as a suicide prevention strategy [29,30]. Along these lines, Milner et al. [31] propose that large-scale clinical trials would be appropriate to examine the cost-effectiveness and usefulness of implementing brief contact intervention programs and, at present, they are not recommending generalized clinical implementation. In 2016, Noh et al. [32] reviewed five randomized controlled trials (RCTs) comparing telephone-delivered interventions after suicide attempts with a control group. The results suggest that more intensive, structured, evidence-based telephone interventions led by mental health professionals should be developed. In a recent scoping review, Shin et al. [33] present several trends of the ICT-based intervention for suicide prevention applied in clinical settings and identify a need for future research to strengthen the evidence for improving implementation. Luxton et al. [34] suggest that repeated follow-up contacts appear to reduce suicidal behaviour, reporting in their systematic review four studies that showed mixed results with trends toward a preventive effect and two studies that showed no preventive effect.
The present review aims to systematically explore the evidence on remote suicide prevention strategies implemented through synchronous technology-based interventions (i.e., via remote, interactive, real-time communication).
METHODS
The protocol of the systematic review and meta-analysis was registered in the Prospective International Registry of Systematic Reviews (PROSPERO), with the identification number CRD42021275044. The review was developed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) criteria [36]. The method is briefly described as follows; more information can be found in the published study protocol [35].
Eligibility criteria
Types of studies
Randomized control trials (RCT), and non-randomized clinical trials (nRCT)– e.g., quasi-experimental trials.
Types of participants
Adolescents over 12 years of age and adults with reported suicidal ideation or prior suicide attempts. Individuals with non-suicidal self-injury were excluded.
Types of interventions
Secondary suicide prevention interventions delivered via synchronous distance communication technologies– i.e., telephone contact, 24-hour telephone hotlines, videoconferencing therapy, immediate text messaging, etc. Interventions based on asynchronous telecommunication devices were excluded.
All comparison groups identified– e.g., treatment as usual (visits to mental health services, pharmacotherapy, etc.)– were included. Non-reporting of an intervention group was a reason for exclusion.
Data collection and analysis
Information sources
Bibliographic searches were conducted in PubMed, PsycInfo, Scopus, and Web of Science for studies published before June 2023. ClinicalTrials.gov and Google Scholar were searched for gray literature and unpublished records. Reference lists of previous systematic reviews on the subject and references cited in eligible articles were consulted for data collection.
Search strategy
The general structure of the search syntax and the electronic search strategy developed for the PubMed database are available in Supplementary file 1 of the study protocol [35]. The search was unrestricted by year of publication, limited to English or Spanish, and developed with the collaboration of a health sciences librarian (GC), adhering to the Peer Review of Electronic Search Strategies (PRESS) [39].
Selection process
The results of the literature search were imported into Mendeley (version 1.19.8), and Rayyan Systems Inc [40]. Duplicate articles were removed automatically by Rayyan Systems Inc. and manually by the first reviewer (LC). After, two authors (LC and MPJ) blind-screened all articles based on titles, abstracts, and keywords. Then, two reviewers (LC and MPJ) independently evaluated the full-text articles according to the eligibility criteria. Discrepancies were resolved through discussion with a third author (AS) until reaching consensus.
Data collection process
Two authors (LC and MPJ) performed the data extraction independently, applying an ad hoc extraction form in Microsoft Excel (version 16.56).
Data items
Data were extracted on participants and intervention characteristics, outcomes related to suicidal behaviour for intervention and comparison groups– for all measures, time points, analyses, etc.–, and limitations. In addition, therapeutic adherence– specifically, the moderating effect of adherence on the efficacy of the intervention, the description of measures to maximize adherence to treatment, and predictor or moderator variables of adherence– were examined.
Risk of bias (RoB) assessment
Two reviewers (LC and MPJ) performed the RoB assessment independently, using the Revised Cochrane risk-of-bias tool for randomised trials (RoB 2.0) [41] and Risk-of-bias In Non-randomised Studies of Interventions (ROBINS-I) [42]. Disagreements were resolved by consensus with a third blinded reviewer (AS).
Effect measures
Systematically examined all types of psychometric measures used in the selected trials (e.g., risk ratio, mean difference) for the effects of each intervention group on suicidal ideation, repeated suicide attempts, and death by suicide.
Synthesis methods
A systematic review, meta-analysis, and narrative synthesis were performed. First, a systematic review was employed to collect and synthesize the empirical evidence that complied the eligibility criteria. Second, a meta-analysis using a random-effects model was calculated. To ensure that the combined numerical data from the different studies are comparable and can be adequately synthesized, subgroup analyses by sorting studies with the same evaluation measures time frame were performed for each outcome, and a narrative synthesis approach was adopted when a quantitative combination of the studies was not feasible.
Three types of meta-analyses were performed: a random-effects model with Hedges’ g [43] as the effect size measure and 95% confidence intervals (CI) was calculated for suicidal ideation. Effect sizes are considered small (g ≥ 0.2), medium (g ≥ 0.5) or large (g ≥ 0.8) [43]; a random-effects model with the effect estimates weighted by the inverse of the variance was calculated for suicide attempts. As proposed by Daly [44] and Zhang and Yu [45], the odds ratio (OR) and 95% CI were analysed; and a random-effects model with the effect estimates weighted by the Peto et al. method [46] was calculated for suicide deaths, since the observed frequencies are relatively low. Statistical heterogeneity was accounted for using I2 statistic. Heterogeneity was considered substantial if I2 was greater than 30%. All analyses were performed using the Meta-Essentials tool for Microsoft Excel (version 16.56) [47].
In trials with multiple assessment measurement periods, the trials were included as two separate studies; to avoid double counting, the control group data were shared between the two study comparisons [48].
RESULTS
Study selection
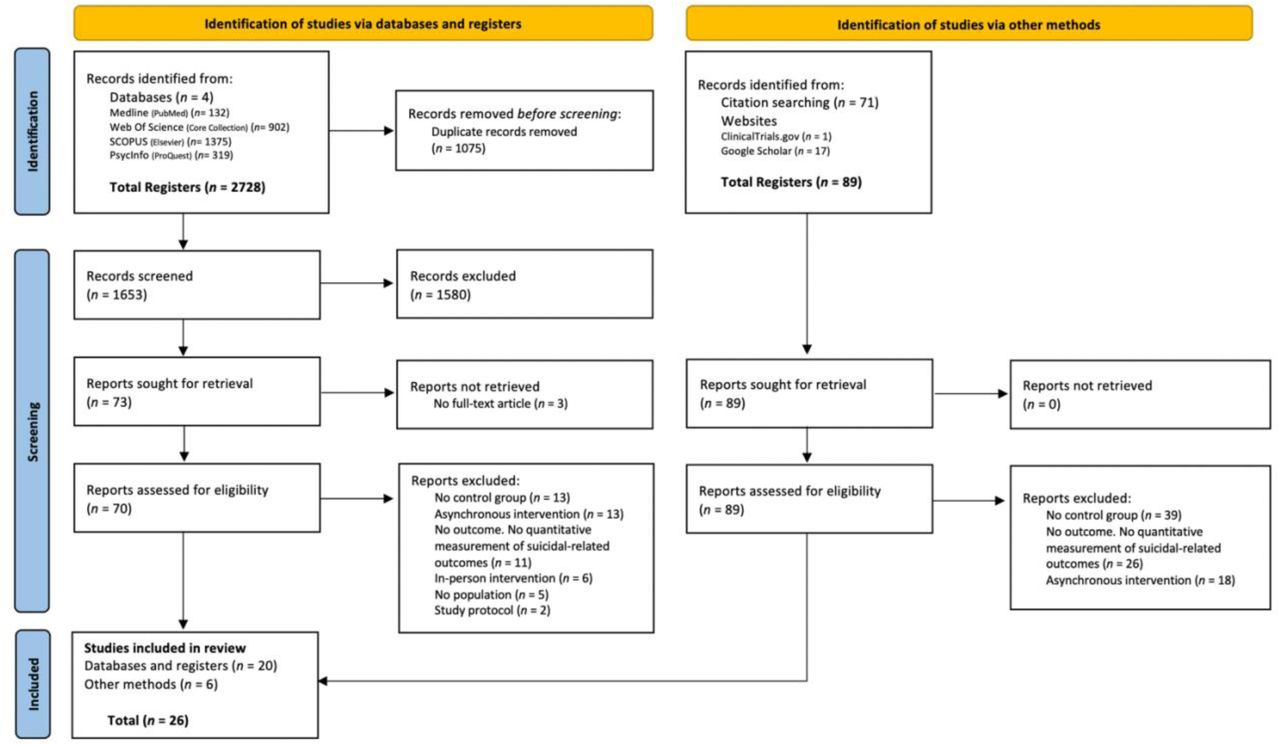
The initial search retrieved 2817 studies. After removing duplicates, 1742 articles were screened for title, abstract, and keywords. Of these, 159 studies were selected for full-text review. Finally, 26 publications were included in the review [49–74]. The article selection process was described in a PRISMA flowchart [75] (Figure 1). Inter-rater agreement was calculated for initial screening using Delta (δ = .91, CI 95%: 0.88 – 0.94) [76], and for eligibility and extraction process using Cohen’s Kappa (κ = .82, CI 95%: 0.62 – 1.01; κ = .91; κ = .98, CI 95%: 0.97 – 0.99, respectively) [77].

Study characteristics
A descriptive summary of the characteristics of the included studies is presented in Table 1. The studies were classified into two categories: 15 trials in the Active Contact and Follow-up group, and 11 studies in the Multi-Component Interventions group (Supplemental File 1: Table S1). The present review included 18 RCT (69.2%) [49, 50, 53–55, 57, 60, 62, 63, 65–68, 70–74]. The sample size ranges from 10 to 3068 in the intervention group (IG) and from 10 to 3694 in the control group (CG). The mean age ranged from 23 to 45 years in the IG and from 23 to 47 years in the CG. The proportion of women in most of the studies was above 50% in both IG and CG, except in three studies [55, 70, 73]. The participants in 23 studies were patients discharged from ED for suicidal behaviour [49–53, 56–69, 71–74], the participants in the remaining studies were callers to a national 24h-helpline service with moderate-to-high psychological distress [54], or patients identified as being at risk of suicide [55, 70]. The eligible articles were from 11 countries: France [56, 63, 65, 69, 71, 72], Spain [51, 52, 58, 59, 61], United States of America (USA) [55, 64, 70, 73], Iran [60, 62, 66, 67], Brazil, India, Sri Lanka, Iran, China [50, 57], French Polynesia [49], Sweden [53], Australia [54], United Kingdom (UK) [68], and China [74].
As for outcomes variables, seven studies reported outcomes relating to suicidal ideation [53–55, 68, 70, 73, 74], 24 studies reported the proportion of participants who reattempted suicide [49–53, 55, 56, 58–74], and 12 reported the proportion of suicide deaths [49, 52, 55, 57, 59–62, 64, 65, 71, 72]. There was a high heterogeneity in the diagnostic methods used to identify suicide behaviours: European Parasuicide Study Interview Schedule (EPSIS), Scale for Suicide Ideation (SSI), General Health Questionnaire (GHQ-28), Columbia Suicide Severity Rating Scale (CSSRS), Beck Scale for Suicidal Ideation (BSS), Suicide Attempt Self-Injury Count (SASI-Count), Beck’s Suicide Intent Scale (SIS), Multisite Intervention Study on Suicidal Behaviours (SUPRE-MISS), forensic records of suicide deaths, data from electronic medical records, etc. The secondary outcomes assessed included: sociodemographic and clinical characteristics (e.g., physical health status, clinical psychopathology, alcohol and drug use, psychosocial difficulties, quality of life, psychological distress, hopelessness, anxiety, depression, etc.) [49–74], method and characteristics of the index suicide attempt (psychiatric hospitalization, lethality of the suicide attempt, concomitant consumption of toxic substances before the suicide behaviour, personal and family history of previous suicidal behaviour, etc.) [50, 57, 60, 61, 63, 65–69, 71, 72, 74], time to relapse [51, 52, 58], adherence to treatment as usual (TAU) [55, 58, 70, 73], social connectedness, support from a significant other, family, and friends [70], and self-injurious behaviours [73].
The interventions were categorised as (a) telephone follow-up intervention (n = 15; 57.7%) [51–53, 56, 58, 59, 61–63, 66, 67, 69, 71, 72, 74], (b) BIC (n = 5; 19.2%) [49, 50, 57, 60, 70], (c) 24-hour call-in services (n = 1; 3.8%) [54], (d) instant text messages (n = 1; 3.8%) [55], (e) Emergency Department Safety Assessment and Follow-up Evaluation (ED-SAFE intervention; n = 1; 3.8%) [64], (f) postal cards, 24-hour telephone, and telephone follow-up (n = 1; 3.8%) [65], (g) Safety Planning and telephone follow-up intervention (SAFETEL intervention; n = 1; 3.8%) [68], and (h) Dialectical Behaviour Therapy Skills-Based Intervention (DBT-BSI) and telephone follow-up (n = 1; 3.8%) [73]. On the other side, the control group in most studies was TAU (n = 24; 92.3%) [49–67, 68–72], except for two studies which were an active control group: relaxation training condition [73] and cognitive therapy group [74]. Most interventions were performed by nurses (n = 7; 26.9%) [51, 52, 53, 56, 58, 59, 61], psychologists (n = 6; 23.1%) [55, 62, 63, 68, 70, 72], psychiatrists (n = 5; 19.2%) [65, 66, 67, 69, 71], physicians (n = 1; 3.8%) [64], and by a combination of health professionals– i.e., medical doctor, psychiatric nurse, psychologist, or social work, in some cases (n = 4; 15.4%) [49, 50, 57, 60]– although, few interventions were undertaken by non-health professionals (n = 2; 7.7%) [54, 74] or not reported (n = 1; 3.8%) [73]. The onset of the intervention– i.e., initial contact– could be categorised in a time interval of days (n = 3; 11.5%) [55, 65, 68], weeks (n = 19; 73.1%) [49–52, 54, 56–63, 66, 67, 69, 72–74], months (n = 2; 7.7%) [53, 71], or not reported (n = 2; 7.7%) [64, 70]. The total number of contacts ranged from 1 [63, 71, 72] to 14 [62], with a minimum duration of 5 minutes [51, 52, 57] and a maximum of 40 minutes [74]. In addition, the follow-up period ranged from 2 months [56] to 5 years [52], with 12 months being the most prevalent research period range (n = 10; 38.5%) [51, 53, 54, 55, 58, 59, 61, 62, 64, 65], reflecting that suicide risk is high within the first year of a suicide attempt [32].
Risk of bias in studies
The results of the RoB 2.0 [41] evaluation is presented in Table 2, in addition, the ROBINS-I [42] evaluation is shown in Table 3. Inter-rater agreement was calculated using Cohen’s Kappa (κ = .94, CI 95%: 0.87 – 1.02) [77]. The overall RoB ratings were classified as low, moderate, or serious. A total of 7 (26.9%) studies met the criteria to be classified as low risk of bias; in 12 (46.2%) studies the risk of bias was moderate; while in 7 (26.9%) studies the risk of bias was high.
Results of individual studies
Suicidal ideation
The results of the meta-analysis of the effects of synchronous remote-based intervention on suicidal ideation are shown in Figure 2. Among the 26 trials, three studies reported the effects of the intervention on suicidal ideation within 1 month [54, 73, 70], two studies within 3 months [70, 73], two studies within 6 months [54, 68], and three studies within 12 months [53–55]. There was a small, non-statistically significant effect (Hedge’s g = −0.23; 95% CI −1.54 – 1.07) on the prevention of suicidal ideation.

Suicide attempts
The results of the meta-analysis of the effects of synchronous remote-based intervention on suicide reattempts are shown in Figure 3. Among the 26 trials, five studies reported the effects of the intervention on suicidal ideation within 1 month [56, 66, 67, 70, 73], four studies within 3 months [67, 70, 73, 74], 8 studies within 6 months [60, 63, 66–69, 72, 74], 10 studies within 12 months [51, 55, 58, 59, 61, 62, 64, 65, 69, 74], four studies within 13 months [53, 63, 71, 72], and two studies within 18 months [49, 50]. There was a statistically significant effect (OR = 0.75; 95% CI 0.62 – 0.90) on the reduction (25%) of suicide attempt, although there was severe heterogeneity (78.8%).

Suicide death
The results of the meta-analysis of the effects of synchronous remote-based intervention on suicide deaths are shown in Figure 4. Among the 26 trials, two studies reported the effects of the intervention on suicide deaths within 6 months [60, 72], five studies within 12 months [55, 59, 61, 64, 65], two studies within 13 months [71, 72], and two studies within 18 months [49, 57]. There was a statistically significant effect (Peto OR = 0.37; 95% CI 0.18 – 0.77) on the reduction (63%) of suicide deaths.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results of narrative synthesis
Effects of Telephone Contact Interventions on Suicidal Behaviours
A total of 14 articles examined the efficacy of Telephone Follow-up Interventions in the prevention of suicidal ideation, suicide attempts, and suicide deaths [51–53, 56, 58, 59, 61, 62, 66, 67, 69, 71, 72, 74]. The studies by Cebrià et al. [51], Exbrayat et al. [56], Malakouti et al. [62], Plancke et al. [69], and Vaiva et al. [71] reported differences for suicide reattempts in the intervention group compared to the control group, and a significant effect of the intervention group in reducing the rate of reattempts. Cebrià et al. [52], after a 60-month follow-up, indicated that there was no significant difference in either group in terms of suicide reattempts (31.4% vs. 34.4%, p = .40). The reattempt prevention effect observed in the first 12 months of follow-up was not sustained over 5 years of follow-up.
Cedereke et al. [53] and Mousavi et al. [67] found significant reductions for suicidal ideation, regardless of the intervention condition, although no significant differences between groups were reported. On the other hand, Wei et al. [74] compared a telephone intervention with a cognitive therapy group and a control group, showing reductions in the number of suicide reattempts between intervention and control groups (1.3% vs. 6.5%, p = .08), although the differences were marginally significant. No statistically significant differences in suicidal ideation were shown between the three groups at any assessment point (baseline: p = .43, 3-month: p = .72, 6-month: p = .75, 12-month: p = .67).
Gabilondo et al. [58], Goñi-Sarriés et al. [59], López-Goñi & Goñi-Sarriés [61], Mousavi et al. [66], Mousavi et al. [67], and Vaiva et al. [72] reported no significant differences between intervention and control groups for suicide reattempts. In addition, Goñi-Sarriés et al. [59] informed that there were no significant differences for suicide deaths. More detailed information in Table 1.
Effects of Text Message Interventions on Suicidal Behaviours
Comtois et al. [55] conducted a follow-up text-messaging intervention with soldiers and marines targeted as being at risk for suicide. Eleven contacts were made by mental health clinicians, with participants’ text message responses monitored 24 hours a day. The authors reported no significant effect of the intervention on the presence or severity of current suicidal ideation; furthermore, the intervention did not significantly decrease the odds of a suicide risk incident during the 12 months follow-up period.
Effects of Multi-component Interventions on Suicidal Behaviours
A total of 11 articles examined the efficacy of a multi-component Synchronous Telepsychiatry Strategies– e.g., 1-hour psychoeducational session plus telephone contacts– in the prevention of suicidal ideation, suicide attempts, and suicide deaths [49, 50, 54, 57, 60, 63–65, 68, 70, 73]. Miller et al. [64] evaluated the ED-SAFE intervention, which consisted of a risk screening and 7 post-ED telephone calls. No significant differences in risk reduction were found between the TAU and screening phases (22.9% vs. 21.5%, p = .99). Mouaffak et al. [65] delivered postcards, in combination with the possibility of calling a 24-hour telephone, and with telephone follow-up at 2 weeks, 1, and 3 months after discharge from the ED. No significant differences were found between the intervention and control groups for suicide reattempts (14.5% vs. 14%, OR = 1.01, 95% CI 0.52 – 1.97, p = .89). Messiah et al. [63] evaluated the effectiveness of the AlgoS Algorithm, which consisted of a telephone follow-up for multi-attempters or a crisis card for first-attempts versus TAU. Telephone follow-up was conducted at 10 and 21 days by a psychologist. There was no significant difference for multi-attempters in the intervention group compared to the control group for suicide reattempts at 6 (Relative Risk; RR = 0.84, 95% CI 0.57 – 1.25) and 14 months (RR = 1.00, 95% CI 0.73 – 1.37).
Amadéo et al. [49], Bertolote et al. [50], Fleischmann et al. [57], and Hassanzadeh et al. [60] investigated the efficacy of BIC, using brief 1-hour educational intervention combined with telephone contacts at 1, 2, 4, 7, 11 weeks, 4, 6, 12, and 18 months delivered by physicians, psychiatric nurses, psychologists, psychiatrists, or social workers. No significant reduction was found in the intervention group compared to the control group for suicide reattempts, although, a significant reduction in suicide deaths in the intervention group compared with the control group (0.2% vs. 2.2%, p < .001) at 18-months was reported in the study by Fleischmann et al. [57]. In a similar intervention protocol, Riblet et al. [70] contacted by telephone or video over 3 months, mailed educational materials, and performed a 1-hour educational intervention on suicide prevention also by telephone or video. A reduction in suicidal ideation was found in the intervention group compared with the control group at 1 and 3 months, with effect sizes in the medium to large range for suicidal ideation (Hedges’ g = 0.71). No suicide attempts occurred during the study.
Christensen et al. [54] conducted a web-based CBT intervention combined with telephone follow-up compared with a CBT-only intervention and a TAU group. CBT was delivered in five modules and telephone contacts were provided weekly by a 24h telephone counselling service. Significant reductions in suicidal ideation, in the telephone call condition, at 1-month post-intervention (p = .003), 6-month follow-up (p = .03), and 12-month follow-up (p = .01) were found. Similarly, Ward-Ciesielski et al. [73] conducted a single-session Dialectical Behaviour Therapy Skills-Based Intervention (DBT-BSI) and telephone follow-up at 1, 4, and 12 weeks, compared with a control group. A significant reduction in levels of suicidal ideation was reported in both conditions, although there were no significant differences between conditions for suicidal ideation and number of suicide attempts. O’Connor et al. [68] evaluated the effects of the SAFETEL intervention against TAU. A safety planning intervention (SPI) session and 5 weekly optional telephone calls were conducted. No significant differences were found between the intervention group and the control group for suicide attempts (Incidence Rate Ratio; IRR = 1.10, 95% CI 0.43 – 2.79, p = .85).
Effects of Synchronous Remote-Based Interventions on Treatment Adherence
Seventeen studies reported on outcomes relating to treatment attendance [49–53, 57–63, 68, 71–74]. In relation to the moderating effect of adherence on the efficacy of the intervention: Gabilondo et al. [58] observed that the intervention group showed significantly higher adherence to outpatient follow-up (p < .001); in addition, Hassanzadeh et al. [60] revealed an increase in patients’ perceived need for support (p < .001) and positively influenced attitudes toward seeking support from services and family.
According to Cebrià et al. [52], suicide attempters tend to be ambivalent to treatment, do not attend treatment, or drop out prematurely; complementary, López-Goñi & Goñi-Sarriés [61] showed in their study that completion of the Telephone Follow-up Programme (TFP) correlated with a reduction in suicidal behaviours. Ward-Ciesielski et al. [73], and Wei et al. [74] also mention that the 75% retention rate underscores the acceptability and effectiveness of the study in engaging a historically hard-to-reach and difficult-to-retain population. Fleischmann et al. [57] mention that BIC operates similarly to psychosocial counselling, providing temporary social support and fostering feelings of connectedness through systematic follow-up contacts.
Moreover, Vaiva et al. [71] reported that participants in the intervention group discussed their suicide attempt with their primary care physician more frequently than controls. As mentioned by Messiah et al. [63] telephone calls could complement a multimodal strategy, providing a surveillance tool to drive more aggressive interventions.
In relation to the predictor or moderator variables of adherence: Amadéo et al. [49], López-Goñi & Goñi-Sarriés [61], O’Connor et al. [68], Vaiva et al. [71], and Vaiva et al. [72] concurred that patients lost to follow-up were more likely to be male. Gabilondo et al. [58], Goñi-Sarriés et al. [59], López-Goñi & Goñi-Sarriés [61], Vaiva et al. [71], and Vaiva et al. [72] concluded that the intervention could be more effective for higher risk populations requiring additional support; in these studies, patients who completed PTF demonstrated higher severity of suicide attempts, greater psychopathological severity, used more violent methods, and experienced predominantly affective disorders. In contrast, Ward-Ciesielski et al. [73] found that participants lost to follow-up reported higher levels of depression and anxiety. On the other hand, four studies [57, 62, 68, 74] discussed stigma around suicide as a factor that may affect patients’ attitudes toward seeking support from mental health services and family. More detailed information in Supplemental File 2: Table S2.
Causes of heterogeneity among study results
The investigations on the possible causes of heterogeneity between the outcomes of suicidal ideation (I2 = 34.5%) and suicide attempts (I2 = 78.8%) of the selected studies raise the pertinence of qualitatively synthesizing the results due to heterogeneity in: a) the evaluation measures time frame of the outcomes (Supplementary File 3. Table S3), b) the protocol of intervention design and the characteristics of the intervention and control group– i.e., target effect, measures of effect, method of implementation, administrator-participant interaction, periodicity, number and duration of the intervention, professional delivering the intervention, setting, participants, etc. – (Supplementary File 1. Table S1), c) assessment of risk of bias and study design– differences were observed in the result of RCT versus nRCT studies for suicide attempts and suicide deaths outcomes– (Supplementary File 4. Figure S1; Figure S2). Conclusions regarding the efficacy of synchronous and remote interventions for suicide prevention are complex, given the large heterogeneity reflected in the studies conducted to date.
DISCUSSION
Innovation in the prevention and management of suicidal behaviour is a therapeutic challenge [86]. The present research outlines emerging evidence on suicide prevention through telemedicine in reducing suicidal ideation and behaviours; however, it is not possible to confirm the effectiveness of the interventions, as the methodological and procedural heterogeneity of the available articles does not allow for a quantitative synthesis of the accumulated scientific evidence.
The studies considered investigate the provision of information and counselling to people with suicidal ideation and a history of suicide attempts, (1) assessing the current risk of suicidal behaviour; (2) reinforcing adherence to treatment and follow-up by a health professional; (3) contributing to psychoeducation and identification of factors related to suicidal behaviour; and (4) providing crisis intervention in case of detection of an immediate risk situation. The neologism “connectivity” serves as the central concept in the majority of studies [34]. In addition, the importance of a high frequency of follow-up contacts, earlier intervention, and involvement in the most critical period– i.e., 6 months post-discharged from ED– is also underlined [10, 13, 34, 71]. Reducing loss to follow-up is a critical challenge in suicide prevention, especially during the post-discharge period [13, 87], given historical problems with treatment completion among people involved in suicidal behaviour [88–91]. According to Gabilondo et al. [58] BIC reduce loneliness, increase knowledge about suicide prevention, and improve adherence to routine treatment. Along the same lines, Ward-Ciesielski et al. [73] reported that a notable percentage of participants engaged with mental health services, or initiated psychotherapy, or pharmacotherapy during the synchronous remote intervention follow-up, suggesting a significant benefit of these interventions with a treatment-unengaged population. Nevertheless, Cedereke et al. [53] argued that more research is needed to establish the relationship between adherence to treatment and reduction in suicidal behaviour.
The wide variety of distance programmes for suicide prevention, and the current lack of treatment guidance on their implementation warrant further research to improve and standardise patient care. As concluded in the systematic review by Noh et al. [32] more structured and theory-based interventions for the prevention of suicidal behaviours should be conducted and examined, emphasizing the importance of a conceptual and theoretical framework in the development of interventions and to increase measurable impacts on key outcomes in complex interventions [92]. Despite the common prevention approach, significant variations were found in the procedure of the intervention, and comparison group– i.e., periodicity, number of contacts, moment of assessment, content, practitioner, setting, type of usual treatment, etc.–, as well as in the methodology– i.e., study design, and RoB– of the reviewed studies. Heterogeneity of results could be due to differences in the length of follow-up, the methods used in the different programmes, variability in the number of sessions, or different patient inclusion criteria. Replication of these interventions according to a standardised protocol would facilitate more consistent results [93]. In addition, the lack of adequate reporting of information on the intervention group, comparison group, and TAU components of the studies constitutes an important gap in the literature and opens new lines of research.
Recommendations
In accordance with the synthesis of information and the articles collected on the topic of the review, the authors would like to provide a series of recommendations to standardise the implementation and development of these interventions to obtain data that can be meta-analysed in the future. Firstly, the authors of future studies should consider describing in detail a minimum set of component characteristics of the intervention and comparison groups– particularly for TAU group– as there is considerable heterogeneity between studies. A comprehensive quality checklist is presented in Supplementary file 5. Table S4. In addition, it should be evaluated not only for efficacy and effectiveness, but also for cost-effectiveness, adherence to the intervention and TAU, etc.
Secondly, a universal intervention design protocol should be adopted according to the characteristics of the studies in which an effect has been observed and the recommendations of the authors of previous studies on the topic [51, 54, 56, 57, 62, 69, 71, 72]. Overall, the recommendation is for RCT study designs that provide early interventions after discharge from the ED–maximum 7 days– with long-term follow-up– approximately 12 months–, often as concomitant therapy to TAU– i.e., emergency medical care and follow-up based on severity of suicidal behaviour; psychopharmacology and/or psychotherapy– conducted by a mental health professional to promote suicide risk assessments, clinician-patient connection, and adherence to routine treatment.
Strength and limitations
The main limitation of the present review is the lack of efficacy measurement to determine which protocol of telemedicine for suicide prevention is the most recommendable. The present review is not intended to criticize the selected articles, but to offer opportunities for improving future research. Therefore, we propose recommendations for methodological and practical guidance in developing synchronous remote interventions for suicide prevention (Supplementary file 5. Table S4).
The focus of the present review was synchronous remote-based interventions; therefore, many studies using asynchronous telecommunication devices– i.e., crisis card, self-directed web-based programmes, etc.– were excluded. In addition, the limitation of using ED medical data records or the authorities’ forensic registry is the possibility of underreporting the actual number of nonfatal suicidal behaviours [94]; additionally, suicide is a rare event, making the design of studies with high statistical power particularly difficult. Finally, the included trials used intervention and comparison groups that received TAU; these treatments are often different across studies.
Conclusions
Promoting comprehensive mental health treatment, emphasising follow-up and continuity of care after discharge from the ED may help prevent repeat suicide attempts; however, the precise mechanisms by which interventions reduce repeated suicidal behaviour are unclear, and more protocolised research is required. The effects of telemedicine-based interventions in multicomponent programs remain difficult to assess.
ETHICS AND DISSEMINATION
Ethics approval is not needed, as systematic reviews are based on published studies. The results will be disseminated through peer-reviewed publications.
Ethics statements
Patient consent for publication Not applicable.
Contributors
AS is the guarantor. LC, JML, DP, AC, and AS: Writing - Original Draft. LC, AS, MPJ, JPS, and CM: Software. LC, JML, DP and AS: Project administration, Supervision. All authors: Conceptualization, Methodology, Writing - Review & Editing. JML, AS, JPS, and CM provided statistical expertise. DP and AC provided expertise on suicidal behaviours. All authors approved the final manuscript.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Funding
This research was funded by the Instituto de Salud Carlos III, Subdirección General de Evaluación y Fomento de la Investigación (ISCIII) and Fondo Europeo de Desarrollo Regional (FEDER). The APC was funded by the Instituto de Salud Carlos III, Subdirección General de Evaluación y Fomento de la Investigación (ISCIII) and Fondo Europeo de Desarrollo Regional (FEDER). The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. The Department of Mental Health of Hospital Universitari Parc Taulí, Unitat Mixta de Neurociència Traslacional I3PT-INc-UAB, is the sponsor.
Competing interests
D.P. has received grants and also served as a consultant or advisor for Rovi, Angelini, Janssen, Lundbeck and Servier. The other authors declare no conflicts of interest.
Patient consent for publication
Not applicable.
Supplemental material
Supplementary File 1. Information on the components and characteristics of the intervention and comparison groups (DOCX 29 KB).
Supplementary File 2. Information on therapeutic adherence (DOCX 29 KB).
Supplementary File 3. Evaluation measures time frame of the selected studies (DOCX 31 KB).
Supplementary File 4. Forest plot comparing effects of synchronous – remote interventions on suicidal behaviours with subgroup analysis according to the study design (DOCX 677 KB).
Supplementary File 5. Report of the minimum set of component characteristics (DOCX 23 KB).
Open access
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes are made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Acknowledgements
Authors’ thanks Guillem Cebrián (GC), director of the Library Hospital Universitari Parc Taulí and head of the Unitat de Gestió del Coneixement de l’Institut d’Investigació i Innovació Parc Taulí (I3PT-CERCA), for his invaluable support in the refinement of the search strategies. Authors’ gratitude goes to Universitat Autònoma de Barcelona and Hospital Universitari Parc Taulí for critically analysing the study proposal and motivational support to conduct this protocol. DP thanks the support of Spanish Ministry of Science and Innovation/ISCIII/FEDER (PI21/01148); the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement of the Generalitat de Catalunya (2021 SGR 01431); the CERCA programme of the I3PT; the Instituto de Salud Carlos III; and the CIBER of Mental Health (CIBERSAM). The research has been previously presented at a conference and has been published as a conference abstract [76].
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.
- 16.
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.↵
- 87.↵
- 88.↵
- 89.
- 90.
- 91.↵
- 92.↵
- 93.↵
- 94.↵



