
Abstract
Importance Understanding the mechanisms of primary resistance to immune checkpoint blockade therapy is of paramount importance for treatment selection. Somatic mutations in STK11 and KEAP1, frequently co-mutated in nonsquamous non–small cell lung cancer, have been associated with poor response to immune checkpoint blockade. However, previous reports lack non–immune checkpoint blockade controls needed to properly ascertain the predictive nature of those biomarkers.
Objective To evaluate the predictive vs prognostic effect of STK11 or KEAP1 mutations across different treatment classes in nonsquamous non–small cell lung cancer.
Design A retrospective, real-world data cohort from the Flatiron Health network linked with genetic testing from Foundation Medicine, from January 1, 2011, through December 31, 2018.
Setting Multicenter, including academic and community practices.
Participants Patients diagnosed with stage IIIB, IIIC, IVA, or IVB nonsquamous non–small cell lung cancer who initiated first-line treatment within 90 days after diagnosis.
Main Outcomes and Measures Real-world, progression-free survival and overall survival calculated from time of initiation of first-line treatment.
Results We analyzed clinical and mutational data for 2276 patients with advanced, nonsquamous non–small cell lung cancer (mean age at advanced diagnosis, 66.3 years [SD 10.3], 54.4% female, 80.1% with a history of smoking), including patients treated with anti–programmed death-1/anti–programmed death ligand 1 inhibitors at first line (n = 574). Mutations in STK11 or KEAP1 were associated with poor outcomes across multiple therapeutic classes and were not specifically associated with poor outcomes in immune checkpoint blockade cohorts. There was no observable interaction between STK11 mutations and anti–programmed death-1/anti–programmed death ligand 1 treatment on real-world, progression-free survival (HR, 1.05; 95% CI, 0.76-1.44; P = .785) or overall survival (HR, 1.13; 95% CI, 0.76-1.67; P = .540). Similarly, there was no observable interaction between KEAP1 on real-world, progression-free survival (HR, 0.93; 95% CI, 0.67-1.28; P = .653) or overall survival (HR, 0.98; 95% CI, 0.66-1.45; P = .913). Results were consistent in KRAS-mutated patients.
Conclusion and Relevance Our results show that STK11-KEAP1 mutations are prognostic, not predictive, biomarkers for anti–programmed death-1/anti–programmed death ligand 1 therapy.
Question Are loss-of-function somatic mutations in STK11 and KEAP1 predictive of response to immune checkpoint blockade or simply prognostic?
Findings In this observational real-world cohort totaling 2276 patients, including 574 treated with immune checkpoint blockade, we find that mutations in STK11 and KEAP1 are associated with poor prognosis across multiple first-line treatment classes.
Meaning Mutations in STK11 and KEAP1 are prognostic biomarkers of poor response to both immune checkpoint blockade and chemotherapy.
Introduction
Advances in personalized medicine have significantly changed clinical decision-making in the treatment of non–small cell lung cancer (NSCLC). Drugs for patients carrying an epidermal growth factor receptor (EGFR) or BRAF p.V600E mutation, or anaplastic lymphoma kinase (ALK) or ROS1 rearrangements, have significantly improved survival and established the importance of molecularly defined therapies.1 However, not all patients with NSCLC have benefited, as a fraction of patients do not carry such actionable mutations. More recently, immunomodulatory cancer drugs such as anti–programmed death-1 (PD-1) have shown significant clinical benefit in NSCLC,2 however many patients do not show such benefit, highlighting the need for predictive biomarkers to guide patient stratification strategies.
Measuring tumor programmed death ligand 1 (PD-L1) protein expression using immunohistochemistry assays has been proposed as a rational and biologically sound approach to patient stratification.3 Indeed, multiple PD-L1 assays are approved as companion or complementary diagnostics in NSCLC. However, PD-L1 expression alone does not always correlate with response, and additional biomarkers are needed.
Tumor mutational burden (TMB), typically assessed by tallying up all nonsynonymous mutations, has also been explored as an independent predictive biomarker of response to anti–PD-1 treatment.4 This measure serves as a proxy for the number of putative neoantigens that could be recognized by immune cells to trigger an immune response.
In addition to markers such as TMB and PD-L1, studies have assessed the role of frequently mutated genes in NSCLC as drivers of primary resistance to immunotherapy. Somatic mutations in serine/threonine kinase 11 (STK11)5-7 and kelch-like ECH-associated protein 1 (KEAP1)8 have been proposed as potential modulators of immune response in non-squamous NSCLC. STK11 has been linked to multiple cellular processes, notably in lipid, glucose, and cholesterol metabolism via activation of 5’ AMP-activated protein kinase (AMPK),9 and has been associated with immune escape in a murine model.10 KEAP1 functions as a negative regulator of nuclear factor erythroid 2-related factor 2 (NRF2),11 and loss-of-function mutations may contribute to an overactive cytoprotective program. However, genomic data sets from controlled clinical studies are not adequately powered to dissect effects of specific mutations or lack a non–immune checkpoint blockade (ICB) arm to ascertain the predictive nature of those biomarkers. Thus, those studies are challenging to translate into clinical practice to inform treatment options. To assess the predictive or prognostic nature of STK11 and KEAP1 mutations in non-squamous NSCLC, we leveraged real-world data from the Flatiron Health Clinico-Genomic Database (CGDB), which includes patients with detailed clinical information and genomic testing by Foundation Medicine.
Methods
From the CGDB for NSCLC12 (April 2019 release; Flatiron Health, New York, NY), we selected patients who had tumor-based genetic testing performed on the FoundationOne CDx or FoundationOne assay (Foundation Medicine Inc, Cambridge, MA). To mitigate the risk of prior treatments affecting results, we focused our analyses on first-line treatment. To ensure that treatment sequencing was correct, we excluded patients with an advanced diagnosis before January 1, 2011, and those who had initiated first-line treatment after 90 days following their advanced diagnosis date. Patients were further selected to have a nonsquamous histology and by their first-line treatment, resulting in 2276 patients across 5 treatment classes (eTable 1, eMethods). We performed time-to-event analysis on real-world, progression-free survival13 (rwPFS) and overall survival (OS),14 as previously defined.
Results
Consistent with previous estimates, STK11 and KEAP1 mutations were found in 20% (454 of 2276 and 451 of 2276, respectively) of patients and were frequently co-mutated (eFigure 1). Thirty percent (674 of 2276) of patients had tumors which carried either STK11 and/or KEAP1 mutations (STK11-KEAP1) and were enriched for male patients (53.4% vs 42.3%, P < .001, chi-square test), younger age at advanced diagnosis (64.9 vs 66.9 years, P < .001, Student’s t-test), smoking history (96% vs 73.3 %, P < .001, chi-square test), and higher TMB (13.1 vs 7.94 mutations per megabase, P < .001, Student’s t-test) (Table 1). Those results were consistent even when excluding EGFR-mutated patients (eTable 2). KRAS mutations were found in 39% (263 of 674) of STK11-KEAP1 patients (eFigure 1). First-line treatment class was associated with STK11-KEAP1 mutational status, explained by the finding that EGFR mutations are mutually exclusive with STK11-KEAP1 and patients carrying EGFR mutations received EGFR tyrosine kinase inhibitors (TKIs) (eFigure 1, Table 1, eTable 3). In a comparison of STK11-KEAP1 vs wild-type patients, excluding EGFR-mutated patients, first-line treatment was not associated with STK11-KEAP1 status (eTable 2).
STK11 mutations were previously reported to be associated with low levels of T-cell inflammation and tumor PD-L1 expression.6 Consistent with previous reports, patients with STK11-KEAP1 mutations were enriched for negative PD-L1 staining (75.8% vs 60.8%, P < .001, chi-square test; Table 1), as were patients with EGFR mutations (eTable 3).
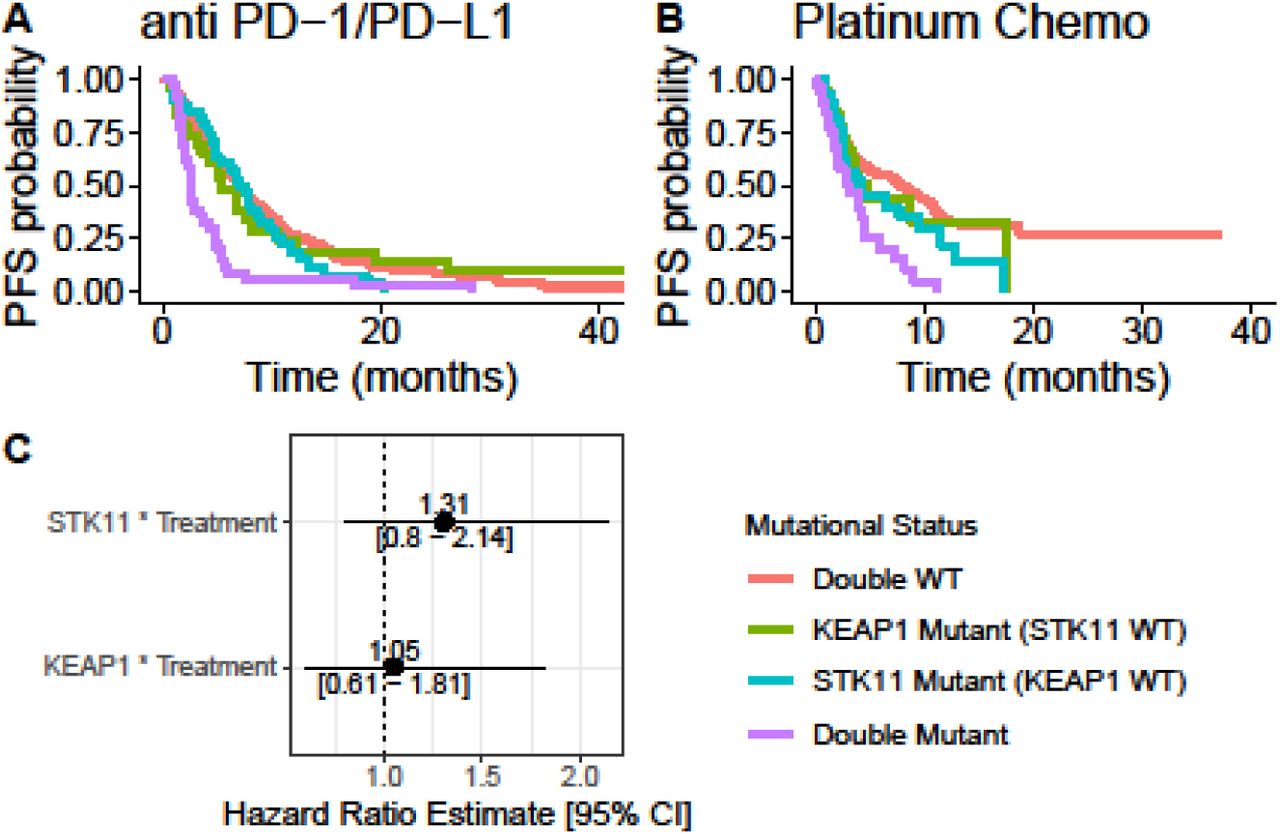
We performed multivariate Cox proportional hazards modeling, including age at advanced diagnosis, gender, TMB (continuous variable), and STK11-KEAP1 mutational status for rwPFS for each treatment class independently. STK11 and KEAP1 mutations were both associated with poor prognosis for rwPFS across treatment classes (Figure 1A). We then focused on anti–PD-1/PD-L1 and chemotherapy treatment classes and tested whether STK11-KEAP1 mutations showed a treatment-specific effect by including an interaction term (STK11-KEAP1 * treatment) in our previous Cox model. Consistent with the previous model, STK11 and KEAP1 mutations were prognostic and did not show different treatment-specific effects (Figure 1B).

(A) Forest plot of the hazard ratios of mutations in STK11 or KEAP1 across different treatment classes. (B) Forest plot of the hazard ratios of the interaction terms of STK11 or KEAP1 mutations and treatment (platinum chemotherapy vs PD-1/PD-L1). (C) Kaplan-Meier curves of PD-1/PD-L1–treated patients according to STK11-KEAP1 status. (D) Forest plot of the hazard ratios of STK11 and KEAP1 in PD-1/PD-L1–treated patients. (E) Kaplan-Meier curves of platinum chemotherapy–treated patients according to STK11-KEAP1 status. (F) Forest plot of the hazard ratios of STK11 and KEAP1 in platinum chemotherapy–treated patients.
EGFR, epidermal growth factor receptor; KEAP1, kelch-like ECH-associated protein 1; PD-1, programmed death-1; PD-L1, programmed death ligand 1; rwPFS, real-world progression-free survival; STK11, serine/threonine kinase 11; TKI, tyrosine kinase inhibitor; VEGF, vascular endothelial growth factor; WT, wild-type.
We tested the independent contributions of STK11 and KEAP1 mutations to poor prognosis by testing them in a multivariate model including the interaction between mutations in the two genes. Both genes were associated with lower rwPFS, and KEAP1-only patients fared worse than patients with STK11-only mutations, while patients with double-mutational status had the worst outcomes (Figure 1C-F). The interaction term was not associated with rwPFS, suggesting that STK11 and KEAP1 mutations have an additive effect. Those results were consistent across anti–PD-1/PD-L1 and chemotherapy treatment classes (Figure 1C-F).
We then performed an analogous analysis using OS as the endpoint and observed the prognostic nature of STK11-KEAP1 mutations to be highly consistent with observations for rwPFS (Figure 2A-F).

(A) Forest plot of the hazard ratios of mutations in STK11 or KEAP1 across different treatment classes. (B) Forest plot of the hazard ratios of the interaction terms of STK11 or KEAP1 mutations and treatment (platinum chemotherapy vs PD-1/PD-L1). (C) Kaplan-Meier curves of PD-1/PD-L1–treated patients according to STK11-KEAP1 status. (D) Forest plot of the hazard ratios of STK11 and KEAP1 in PD-1/PD-L1–treated patients. (E) Kaplan-Meier curves of platinum chemotherapy–treated patients according to STK11-KEAP1 status. (F) Forest plot of the hazard ratios of STK11 and KEAP1 in platinum chemotherapy–treated patients.
EGFR, epidermal growth factor receptor; KEAP1, kelch-like ECH-associated protein 1; OS, overall survival; PD-1, programmed death-1; PD-L1, programmed death ligand 1; STK11, serine/threonine kinase 11; TKI, tyrosine kinase inhibitor; VEGF, vascular endothelial growth factor; WT, wild-type.
We performed the analyses described above in KRAS-mutated patients to test the utility of STK11-KEAP1 mutations as a predictive biomarker for this patient population (eFigure 2). STK11-KEAP1 mutations were associated with poor prognosis in this patient subset in both anti–PD-1/PD-L1- and chemotherapy-treated populations, consistent with our overall findings.
Discussion
Our comprehensive profiling of STK11 and KEAP1 mutations in nonsquamous NSCLC demonstrated that these mutations confer a poor prognosis, regardless of treatment class. Our results complement previous reports suggesting that STK11-KEAP1 patients respond poorly to ICB by highlighting that this effect is observed across all treatment classes and is not specific to ICB cohorts.5,6,8
Limitations
Real-world data are retrospective and observational and thus may not offer the same robustness as prospective randomized clinical trials. Factors that influence clinical decision-making but are not explicitly captured by real-world data sets may exist and thus confound analyses. Other factors such as tumor evolutionary dynamics between specimen collection, diagnosis, and treatment start or during treatment may influence the associations. Moreover, although the cohort was large, it might not be sufficiently powered to capture a low-effect-size interaction between STK11 and KEAP1 mutations.
Conclusion
Our results provide evidence against previous reports suggesting that STK11-KEAP1 mutations are predictive biomarkers for anti–PD-1/PD-L1 therapy.5,6,8 Using a cohort of 2276 patients with NSCLC, we show that STK11 and KEAP1 mutations are associated with poor prognosis across all therapy classes and should not be used as a patient selection marker for ICB.
Data Availability
Data was licensed from Flatiron Health.
eMethods
Treatment Consolidation
First-line treatment data were aggregated in 5 broad treatment classes according to Flatiron Health rules. In summary, regimens that contained anti–PD-1 or anti–PD-L1 were considered “PD-1/PD-L1–based therapies”, those that contained EGFR TKIs as “EGFR TKIs”, and those that contained anti-VEGF as “anti-VEGF–based therapies”. Regimens including a platinum-based and any other chemotherapeutic agent, but not drugs from the above-mentioned class, were classified as “platinum-based chemotherapy combinations”. Regimens with a single chemotherapeutic agent were considered “single-agent chemotherapies”.
Genomic Assay
We selected patient specimens profiled on bait sets DX1, T4b, T5a, or T7 of the Foundation Medicine FoundationOne CDx or FoundationOne assay, as they are performed on tumor material (as opposed to blood) and they contain tumor protein p53 (TP53), STK11, KEAP1, and KRAS in their gene panel.
STK11, KEAP1, and TP53 Mutations
We aggregated gene-specific alterations, filtering for missense mutations, truncations, and deletions. For OncoPrint visual display, all mutations were considered. For Cox proportional hazards and Kaplan-Meier modeling, patients were labeled as mutant for a gene if they had at least 1 qualifying (missense, truncation, and deletion) mutation in that gene. OncoPrint plots were created using ComplexHeatmap R package.15
KRAS Mutations
For simplicity, we labeled only patients who carried a missense mutation in the hotspot locus G12-13 as KRAS-mutated, whereas patients carrying other alterations were considered as KRAS–wild type.
Time-to-Event Analysis
We performed rwPFS and OS analysis using Cox proportional-hazards modeling in R. Kaplan-Meier curves were displayed using the R package survminer.
PD-L1 Harmonization
To obtain PD-L1 immunohistochemistry data for as many patients as possible, we harmonized the PD-L1 immunohistochemistry data from different tests by considering numerical values >50% tumor cell scoring as positive.
Supplementary Tables and Figures

Abbreviations: EGFR, epidermal growth factor receptor; KEAP1, kelch-like ECH-associated protein 1; NSCLC, non–small cell lung cancer; STK11, serine/threonine kinase 11; TP53, tumor protein p53.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Kaplan-Meier curves of PD-1/PD-L1–treated patients according to STK11-KEAP1 status. (B) Kaplan-Meier curves of platinum chemotherapy–treated patients according to STK11-KEAP1 status. (C) Forest plot of the hazard ratios of the interaction terms of STK11 or KEAP1 mutations and treatment (platinum chemotherapy vs PD-1/PD-L1).
Abbreviations: KEAP1, kelch-like ECH-associated protein 1; PD-1, programmed death-1; PD-L1, programmed death ligand 1; rwPFS, real-world progression-free survival; STK11, serine/threonine kinase 11; WT, wild-type.
Acknowledgements
Contribution of authors: SP-C and AMW performed analyses. All authors participated in writing the article. Editorial assistance was provided by Michelle Utton-Mishra, PhD, and Jay Rathi, MA, of Spark Medica Inc, according to Good Publication Practice guidelines, funded by Bristol-Myers Squibb. All authors are BMS employees and shareholders. PD is a J&J shareholder, RD is a Merck and J&J shareholder.
References



