
Abstract
The paper will attempt to estimate factors which determine the variability of case fatality rates of COVID-19 across OCED countries in recent time. The objective of the paper is to estimate the impact of government health policy on fatality rates (Case fatality rates) of COVID-19 in countries while controlling for other demographic and economic characteristics. The analysis is of done using non-parametric regression method, i.e. Quantile regression. The result from quartile regressions analysis shows that a policy of Austerity (health expenditure cuts) significantly increases the mortality rates of COVID-19 in OCED countries. The policy implication of the study is the need for a robust public-funded health system with wider accessibility to deals with a major public health crisis like a COVID-19 pandemic.
JEL: I18, I38, C31
1. Introduction
The contemporary world is facing an unprecedented public health crisis of emerging from Covid-19. Covid-19 has spread to 200 countries and infected 877422 people across the world. Out of total infected people across the globe, nearly 43537 has died, and 185241 has recovered till 1st April 2020(CSSE, 2020). After the outbreak of Covid-19 and declaration of its being Pandemic by WHO, there has been a massive increase in the volume of research on Covid-19 (Heymann & Shindo, 2020; Novel, 2020). However, most research is limited to clinical perspective including SARS Cov-2 reproduction rate (Liu et al., 2020), fatality ratio (Onder et al., 2020; Wu & McGoogan, 2020), asymptotic transmission mode (Bai et al., 2020) and other epidemiological characteristics (Atkeson, 2020; Lipsitch et al., 2020; Remuzzi & Remuzzi, 2020; Rothan & Byrareddy, 2020; Xu et al., 2020). The countries across the globe have responded with various measures including rapid testing of population, isolating suspected individuals, imposing strict social distancing norms, totally shut down of economic activities in the form of lockdowns (Ebrahim et al., 2020; Kupferschmidt & Cohen, 2020; Tanne et al., 2020; Wong et al., 2020). The economic impact of Covid-19 for different regions and countries are studied using different (Abiad et al., 2020; Atkeson, 2020; Fernandes, 2020; Hartley & Makridis, 2020; McKibbin & Fernando, 2020; Ruiz Estrada, 2020).
2. Objective of Research
Review of existing literature on Covid-19 shows the dynamic interplay between the Covid 19 and the country-specific health policy is still missing. This paper attempts to fill this gap by highlighting the interrelationship between the long term structural health policies and the Covid 19 fatality rates among Organisation for Economic Co-operation and Development (OECD) countries 2. Definition of Austerity policies is a widespread cut on government expenditure which is targeted to reduce government fiscal deficit and enhance economic growth(Konzelmann, 2014;). Such a significant reduction in government spending has a disproportionately negative impact on government social sector expenditure (Health, Education, social security etc.) The negative impact of austerity policies in terms of lowering employment, economic growth and increasing inequality is well studied (Blyth, 2013; Krugman, 2015; Stiglitz, 2012; UNCTAD, 2017). In the post.-2008 crisis period and under the impact of rising debts burdens, many countries in European counties imposed a policy of austerity in 2010. The most severe austerity policies were implemented in Greece, Hungary, Ireland, Latvia, Spain and Portugal (Leschke et al., 2015). Among the OCED group, there is variation in the extent of reduction in their health expenditure in pursuit of Austerity policies(fiscal consolidation) across countries (Van Gool & Pearson, 2014). The negative impact of such drastic funding cuts on access to health facilities and health indicators is well documented in many OCED countries (Antonakakis & Collins, 2014; Ayuso-Mateos et al., 2013; Ifanti et al., 2013; Kentikelenis et al., 2014, 2014, 2014; Loopstra et al., 2016, 2016; McKee et al., 2012, 2012; Reeves et al., 2014, 2014; Ruckert & Labonté, 2017; Stuckler et al., 2017). So under the background of such drastic cuts in health expenditure, the papers will evaluate the impact of austerity policies (health expenditure cuts) on fatality rates of Covid-19 after controlling for other socio-demographic characteristics which have a significant impact on fatality rates of covid-19. The fatality rates are measured by crude Case fatality rates (CFC), which is the ratio of confirmed death to confirmed positive cases of covid-19 for each country.
3. Data source and Methodology
The data source for analysis is taken from different data sources. Following is the table providing a list of variable and their data source.
The data for analysis is from thirty-six countries3 from the OECD group.
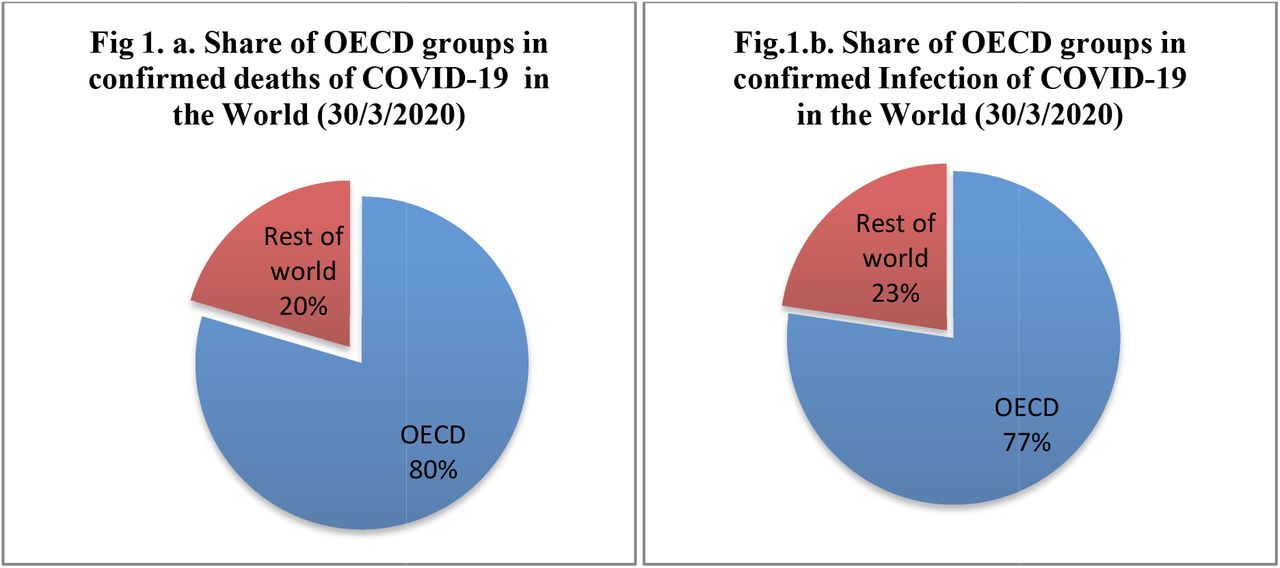
Moreover, the figure1 (a, b) shows that large part of infection and deaths from Covid-19 in the world is concentrated in OECD regions only.
The analysis of the impact of austerity on covid-19 fatality rates is done using Quantile regression after controlling for all other socio-demographic characteristics which have an impact on Case fatality rate(Novel, 2020; Onder et al., 2020; Porcheddu et al., 2020; Wu & McGoogan, 2020). The advantage of quantile regression over normal Ordinary least square regression (OLS) regression is that it gives a rich picture of the relationship between variables not only around mean value but across the distribution of variables(Koenker & Hallock, 2001). It is distribution-free, robust to outliers, capable of modelling entire conditional distribution (Baum, 2013; Cade & Noon, 2003; Yu et al., 2003).
4. Statistical Analysis
The table 2 shows that descriptive statistics of all the variables. The mean value of Case fatality rate (of 30 March 2020) is 2.554 with a standard deviation of 2.79. The highest value taken by case fatality rate (cfr30march) is 11.6, whereas the smallest value is 0. Similarly, the other variable for case fatality rate, cfr3daymedian, also has a similar kind of mean and standard deviation as the previous cfr30march variable.
The average value of public spending in health to GDP variable, publichelathgdp, is 5.95 % and it has a minimum value from 0.9 per cent and the maximum value of 14.4 per cent. The existing clinical research shows that fatality rate of Covid-19 is influenced by the existence of pre-medical complication and the share of older adults in the population (Onder et al., 2020; Wu & McGoogan, 2020). The crucial demographic variable, population share above 65 years (popu65), has a mean value of 15 per cent and a standard deviation of 5.4. The share of the population having hypertension (above 18 years age) has a minimum value of 13 % and a maximum value of 38.2 %.
b. Quantile Regression
Table 3 shows the result of Quantile regression. The first model has a case fatality rate from March 30 as the dependent variable. In the second model, the dependent variable is the three-day median case fatality rate. The result from both models shows that the coefficient of the dummy variable for high fund cut has a positive impact on CFR and is significant at one per cent level of significance. The result shows that a country which has a history of drastic health fund cut is increasing the fatality rates from covid-19. Similarly, the coefficient of the variable of public health GDP is negative and significant at one per cent level of significance.
It shows that countries which have a higher share of the public-funded health system have a lower case fatality rate.
The impact of good health infrastructure (measured by bed per 1000 population and doctor per 1000 population) on case fatality rates is negative. As expected in exiting literature higher population having a higher old age has higher fatality rates. Also, the higher share of pre-existing medical condition in the overall population, higher is the fatality rate from COVID-19.
The presence of model specification error is done using the link test. If the regression model does not contain specification error, then the variable _hatsq will be statistically insignificant. Table 4 shows the result of the link test for Model -1. The P-value of variable _hatsq is 0.16, and hence it is statistically insignificant. So model-1 does not contain specification error.
Similarly, the link test result of model-2 also shows that variable _hatsq is not statistically significant. Hence model-2 does not contain specification error.
In order to gets idea about coefficient of Quantile regression of independent variables across quantile of case fatality rates following two figure has been calculated using the Azevedo method (Azevedo, 2011). It shows how the impact of each independent variable varies across quantiles.
Figure 1 and 2 shows that the coefficient of Dummy variable (for health fund cut) of Quantile regression is positive and increases across quantiles of case fatality ratio. Only for the third quantile, the coefficient is negative. So the impact of Austerity is positive on Case fatality rate of Covid-19 except for the third quantile.



{kind=link}
{kind=link}
{kind=link}
The coefficient of the public fund on health to GDP variable is negative(except for the first quantile) across the distribution of case fatality ratio. It indicates that higher public expenditure on health reduces fatality rates of Covid-19. The coefficient of doctor per 1000 population is negative across the distribution of case fatality ratio (except for the second quantile). The coefficient of hospital bed per 1000 population is negative across the distribution of case fatality ratio (except till the fourth quantile).
5. Conclusion
The result from the Quantile regression analysis shows that country which has pursued austerity policies has significantly higher fatality rates from COVID-19 after controlling for all other socio-demographic factors which influence case fatality rate of COVID-19. Higher public funding share, higher doctors per population, higher bed availability is associated with lower fatality rates from COVID-19. A higher share of the population with pre-medical conditions (diabetics, hypertension) and older age population increase fatality rates. So the policies of austerity (at least in terms of reduction in health expenditure) can significantly worsen health system ability to fight pandemic live COVID-19 and can lead to a severe negative health outcome. The policy implication of the study is the need for a robust public-funded health system with wider accessibility to deals with a major public health crisis like a covid-19 pandemic.
Data Availability
Research is based on secondary data which is publicly available.
Footnotes
↵2 Member countries of OECD groups include Australia, Austria, Belgium, Canada, the Czech Republic, Denmark, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Italy, Japan, Korea, Luxembourg, Mexico, The Netherlands, New Zealand, Norway, Poland, Portugal, the Slovak Republic, Spain, Sweden, Switzerland, Turkey, the United Kingdom, and the United States.
References



