
Abstract
Background Coronavirus disease 2019 (COVID-19) is a pandemic affecting millions around the world. There is no existing pharmaceutical treatment that is known to be effective. Preliminary data shows that San Yao San Fang (SYSF) has clinical benefits in patients with COVID-19. The aim of this paper is to review existing data regarding the use of formulas within San Yao San Fang in the treatment of COVID-19
Search Strategy We searched through EMBASE, Pubmed, Cochrane, Wanfang and China National Knowledge Infrastructure (CNKI) for studies on SYSF and patients with COVID-19 through April 2020.
Eligibility Criteria We included studies that included a formula within San Yao San Fang with or without Western interventions against Western interventions.
Main results We included 7 studies involving 532 patients. 3 retrospective observational studies and 1 randomised control trial reported on Lian Hua Qing Wen Jiao Nang, 1 randomised control trial on Jin Hua Qing Gan Ke Li, 1 retrospective observational study on Xue Bi Jing Zhu Se Ye and 1 randomised control trial on Qing Fei Pai Du Tang.
SYSF combined with Western interventions improved the recovery rate of symptoms such as fever (Risk Ratio (RR) 0.40 (95% CI 0.24 to 0.66, P < 0.01)), cough (RR 0.56 (95% CI 0.38 to 0.82, P < 0.01)) and fatigue (RR 0.61 (95% CI 0.47 to 0.78, P < 0.01)) and other symptoms such as headache, gastrointestinal symptoms, myalgia, dyspnoea and chest tightness (RR 0.63 (95% CI 0.47 to 0.83, P < 0.01)) as compared to the control group.
SYSF combined with Western interventions reduced the duration of fever as compared to the control group. (Mean difference (MD) -1.18 (95% CI -1.45 to -0.91, P < 0.01))
In regards to adverse events, there is no statistical difference between the treatment group treated with SYSF and Western interventions and the control group. (RR 1.62 (95% CI 0.83 to 3.17, P = 0.16)).
SYSF combined with Western interventions did not show to significantly reduce duration of hospitalisation as compared to the control group. (MD -0.73 (95% CI -5.19 to 3.73, P = 0.75))
Conclusion SYSF appears to be clinically effective and safe. Further research is required to ensure the efficacy of SYSF.
Introduction
Coronavirus disease 2019 (COVID-19) is a novel disease first identified in Wuhan, China, before spreading to the rest of the world.1 Since then, WHO has declared it as a Public Health Emergency of International Concern on the 30th Jan 2020. COVID-19 patients are usually asymptomatic but could clinically manifest with flu-like symptoms like fever, fatigue, dry cough, anorexia, myalgia and dyspnea. In severe cases, it can progress to Acute Respiratory Distress Syndrome (ARDS) and death.2,3 Emerging studies have also demonstrated hypercoagulable states and Kawasaki disease as possible complications of COVID-19.4,5
Researchers in Wuhan have found death rates to be around 1%.6 The risk increases in patients who are older, male or who have other comorbidities like hypertension, diabetes, cardiovascular diseases and chronic lung diseases.7 As of 04 May 2020, the total number of confirmed deaths stands at 239,604.8 Till date, there is no definite treatment that has proven to be effective in the treatment of COVID-19. Remdesivir developed by GILEAD is one of the more promising medications for the treatment of COVID-19. A recent study done by Chinese researchers showed that patients did not benefit clinically from Remdesivir.9 It was however, refuted to be an underpowered trial which resulted in inconclusive findings.10
With the exponential rise in patients around the world, healthcare providers are under immense pressure to find a possible treatment to speed up the recovery of the patients and prevent a possible collapse of the healthcare system.
During the Severe Acute Respiratory Syndrome (SARS) epidemic in 2003, Traditional Chinese Medicine (TCM) practitioners found herbal medicine to be successful in the prevention and treatment of SARS.11 With this precedence, TCM practitioners are turning towards TCM in hopes of finding a treatment plan that can help prevent and treat COVID-19. TCM has been utilized with success in several reports for the treatment of COVID-19 pneumonia.12 More recently, a new class of herbal formulations known as San Yao San Fang (SYSF) (三药三方)) has been gaining widespread use for treatment in China.
SYSF refers to 3 existing formulas (San Yao) that are thought to be effective in the management of COVID-19 and 3 new formulations (San Fang) created during this pandemic for the treatment of COVID-19. San Yao includes 1. Jin Hua Qing Gan Ke Li (Formula J) (金花清感颗粒), 13 2. Lian Hua Qing Wen Jiao Nang (Formula L) (连花清瘟胶囊)14-15 and 3. Xue Bi Jing Zhu Se Ye (Formula Xb) (血必净注射液).16,17
How the intervention might work
Formula J and Formula L are oral herbal formulations that are typically used for flu like symptoms.18 Formula J targets inflammatory and apoptosis regulation by targeting various mechanisms such as PI3k-Akt, HIF-1, TNF, MAPK and NF-κB.19 On the other hand, Formula L works by inhibiting COVID-19 replication in Vero E6 cells and reduce production of pro-inflammatory cytokines such as TNF-α, IL-6, CCL-2/MCP-1 and CXCL-10/IP-10. 20,21
Formula Xb is an intravenous formulation typically used for fever, dyspnoea, palpitations and in cases like Systemic Inflammatory Response Syndrome (SIRS) and multi-organ failure.22 It has been employed in moderate-severe cases of COVID-19 in China.
San Fang includes 1. Hua Shi Bai Du Fang (Formula H) (化湿败毒方), 2. Qing Fei Pai Du Tang(Formula Q) (清肺排毒汤)23-25 and 3. Xuan Fei Bai Du Fang(Formula Xf) (宣肺败毒方).26 All 3 formulas were recently developed during the COVID-19 crisis to target the different clinical manifestations of COVID-19. Clinical trials are ongoing to identify the underlying mechanism behind the 3 different formulas.
Objective of study
As early studies of SYSF seem to be promising, uncertainty remains about its effectiveness due to empirical usage in treatment of COVID-19 pneumonia. Thus, this study aims to review existing data regarding the use of formulas within SYSF in the treatment of COVID-19, and provide evidence for widespread recommendation and usage of SYSF as part of the management of COVID-19.
Methods
Criteria for considering studies for this review
Types of studies
Trials including the use of any of six Chinese formulas (1. Hua shi bai du fang 2. Jin Hua Qing Gan Ke Li 3. Lian hua qing wen jiao nang 4. Qing Fei Pai Du Tang 5. Xuan Fei Bai Du Tang 6. Xue Bi Jing Zhu She Ye) administered with or without Western medicines for COVID-19 patients were included.
Types of participants
COVID-19 cases diagnosed using any national diagnostic criteria, or by clinical impression of the physician-in-charge were included.
Types of interventions
We included trials administering
Hua shi bai du fang
Jin hua qing gan ke li
Lian hua qing wen jiao nang
Qing fei pai du tang
Xuan fei bai du tang
Xue bi jing zhe she ye
with or without Western medicines for COVID-19 patients, regardless of comparator.
Types of outcome measures
We assessed primary and secondary outcome measures at the end of treatment and/or at the end of follow-up.
Primary outcomes
Persistence of fever, cough and fatigue post0 treatment
Secondary outcomes
Persistence of other symptoms (excluding fever, cough and fatigue) post treatment
Duration of each symptom.
Number of days in hospital
Adverse events/side effects
Hospitalization rate
Search methods for identification of studies
Electronic searches
For this review we searched EMBASE, Pubmed, Cochrane, Wanfang and China National Knowledge Infrastructure (CNKI) (2019-2020)
EMBASE, Pubmed And Cochrane
Jin hua qing gan AND Covid OR Coronavirus
Lian hua qing wen AND Covid OR Coronavirus
Xue bi jing zhu AND Covid OR Coronavirus
Qing fei pai du tang AND Covid OR Coronavirus
Xuan fei bai du tang AND Covid OR Coronavirus
Xue bi jing zhu AND Covid OR Coronavirus
Traditional Chinese Medicine AND Covid OR Coronavirus
CNKI (overseas CNKI) And Wanfang (based on the translations of the keywords used in English medium)
金花清感颗粒 AND 新冠状病毒/冠状病毒/新冠肺炎
连花清瘟胶囊 AND 新冠状病毒/冠状病毒/新冠肺炎
血必净注射液 AND 新冠状病毒/冠状病毒/新冠肺炎
化湿败毒方 AND 新冠状病毒/冠状病毒/新冠肺炎
清肺排毒汤 AND 新冠状病毒/冠状病毒/新冠肺炎
宣肺败毒方 AND 新冠状病毒/冠状病毒/新冠肺炎
中药 AND 新冠状病毒/冠状病毒/新冠肺炎
Searching other resources
We did not impose any language or publication restrictions.
Data collection and analysis
Selection of studies
Four review authors (ZY, L, RS, RM) independently reviewed the titles, abstracts and keywords of all records retrieved to determine the studies to be assessed. We retrieved full articles for further assessment if the information given suggested that the study:
Included COVID-19 patients;
And administered any of six Chinese herbs (1. Hua shi bai du fang 2. Jin hua qing gan ke li 3. Lian hua qing wen jiao nang 4. Qing fei pai du tang 5. Xuan fei bai du tang 6. Xue bi jing zhu she ye) for the treatment of COVID-19
A fifth review author (LH) acted as arbiter and resolved any differences in opinion.
Data extraction and management
Four review authors (ZY, L, RS, RM) independently extracted data from each included trial using a standard extraction form, which included the following items.
General information: published/unpublished, language, authors, article title, journal title and year, volume, issue, page, funding source.
Design of the trial: prescribed size, generation of randomisation sequence, allocation concealment method, blinding information, statistical methods and attrition.
Participants: diagnostic criteria, total number and number in comparison groups, baseline characteristics, age, gender, inclusion criteria, exclusion criteria, study setting.
Intervention: type of herbs and (if any) Western medicine, the content of herbal formulas, duration, times, dose, co-intervention, control, withdrawals, drop out, loss to follow-up.
Outcome: all outcomes.
Conclusion: positive/negative.
Assessment of risk of bias in included studies
We assessed risk of bias following the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions.27 We used a #x2018;Risk of bias’ table to assess the methodological quality of the trials.
Sequence generation: describes the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce
Allocation concealment: describes the method used to conceal the allocation sequence in sufficient detail to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment.
Blinding of participants, personnel and outcome assessors. Assessments should be made for each main outcome (or class of outcomes): describes all measures used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. Provide any information relating to whether the intended blinding was effective.
Incomplete outcome data. Assessments should be made for each main outcome (or class of outcomes): describes the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis. State whether attrition and exclusions were reported, the numbers in each intervention group (compared with total randomised participants), reasons for attrition/exclusions where reported, and any reinclusions in analyses performed by the review authors.
Selective outcome reporting: state how the possibility of selective outcome reporting was examined by the review authors, and what was found.
Other sources of bias: state any important concerns about bias not addressed in the other domains in the tool. If particular questions/entries were pre-specified in the review’s protocol, responses should be provided for each question/entry.
Two review authors (ZY, LH) independently assessed each trial. We resolved disagreements by discussion.
Measures of treatment effect
We extracted both dichotomous data and continuous data with 95% confidence intervals (CIs). We used risk ratios (RR) for dichotomous data. We calculated mean differences (MD) for continuous data. We calculated overall results based on the random-effects model if heterogeneity existed between studies. If no heterogeneity was detected between studies, we used the fixed-effect model.
Unit of analysis issues
We analysed the data using Review Manager (RevMan 2011) software. We summarised data statistically if they were available and of sufficient quality and similarity. We performed meta-analyses within comparisons where individual trials compared the same trial intervention versus the same control intervention.
Results
Description of studies
Results of the search
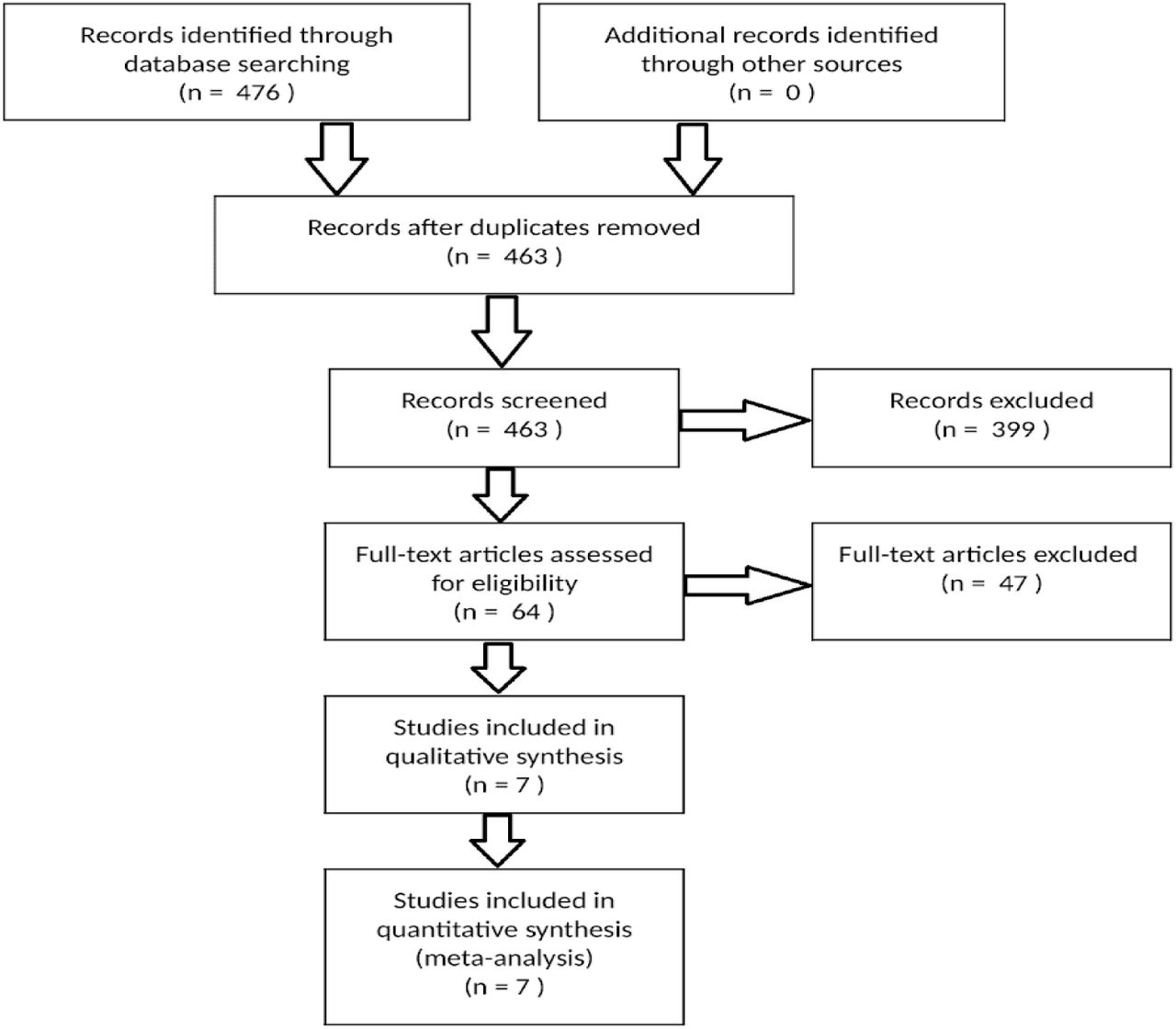
The initial search of electronic databases yielded 476 studies. After scanning the results, 3 RCT and 4 observational trials were identified, which appeared to meet the inclusion criteria as shown in Figure 1.

Study flow diagram
Assessment of heterogeneity
We tested heterogeneity using the Z score and the Chi2 test with significance being set at P < 0.1 and planned to explore possible sources of heterogeneity by subgroup and sensitivity analysis.
Data synthesis
We calculated overall results based on the random-effects model if heterogeneity existed between trials. If no heterogeneity was detected between studies, we considered the fixed-effect model. Hypothesis tests used the Z test. We considered the results had achieved statistical significance if P ≤ 0.1. If P > 0.1, we considered that the results had not achieved statistical significance. CIs were set at 95%.
Subgroup analysis and investigation of heterogeneity
We planned to do a subgroup analysis between RCTs and retrospective observational trials.
Included trials
Seven studies were included for meta-analysis - Cheng et al., 2020 28; Duan et al., 2020 13; Lv et al., 2020 29; Li et al., 2020 24; Wang et al., 2020 30;Yao et al., 2020 31; and Zheng et al., 2020 16. Contents of the formulas and their commonly used indications are specified in Table 1. Summary of the trials are shown in Tables 2-5.
SYSF formulas and respective herb constituents
Summary of existing evidence of Jin Hua Qing Gan Ke Li in the treatment of Covid-19
Summary of existing evidence of Lian Hua Qing Wen Jiao Nang in the treatment of Covid-19
Summary of existing evidence of Qing Fei Pai Du Tang in the treatment of Covid-19
Summary of existing evidence of Xue Bi Jing Zhu She Ye in the treatment of Covid-19
Excluded trials
13 records were duplicates and were removed after the initial search. 447 of the remaining studies were removed because they were either
Discussing the pharmacological properties of SYSF and not clinical studies,
Discussing how SYSF would theoretically work, or
Case reports on individual patients
Risk of bias in included studies
Allocation
The three RCT trials (Duan et al., Cheng et al., Yao et al.) described the methods used to generate random allocation sequences. The other four trials did not mention how allocation was conducted.
Blinding
Single blinding was used in all three of the RCTs (Duan et al., Wang et al., Li et al.).
Selective reporting
Wang et al. reported an improvement by using a criteria which includes symptoms, clinical signs and laboratory results, there were no further breakdown of the data.
Other potential sources of bias
No other potential sources of bias were identified.
Effects of intervention
1. Persistence of symptoms post treatment
a. Fever
Three studies reported this outcome and were analysed - Cheng et al., 2020; Lv et al., 2020 and Yao et al., 2020.
The total population analysed comprised 220 patients, 124 in the SYSF and Western medicine arm, and 96 in the Western medicine alone arm. This gave a statistically significant risk ratio of 0.40 (95% CI 0.24 to 0.66, P < 0.01) in favour of the SYSF and Western medicine arm, with an I2 of 0% (Fig. 2), suggesting that patients receiving SYSF and Western medicine recover from fever sooner after the initiation of treatment.

Persistence of fever post treatment between combined therapy vs Western treatment alone
b. Cough
Three studies reported this outcome and were analysed - Cheng et al., 2020; Lv et al., 2020 and Yao et al., 2020.
The total population analysed comprised 177 patients, 96 in the SYSF and Western medicine arm, and 81 in the Western medicine alone arm. This gave a statistically significant risk ratio of 0.61 (95% CI 0.47 to 0.78, P < 0.01)in favour of the SYSF and Western medicine arm, with an I2 of 0% (Fig. 3), suggesting that patients receiving SYSF and Western medicine recover from cough sooner after the initiation of treatment.

Persistence of cough by post treatment between combined therapy vs Western treatment alone
c. Fatigue
Three studies reported this outcome and were analysed - Cheng et al., 2020; Lv et al., 2020 and Yao et al., 2020.
The total population analysed comprised 199 patients, 106 in the SYSF and Western medicine arm, and 93 in the Western medicine alone arm. This gave a statistically significant risk ratio of 0.56 (95% CI 0.38 to 0.82, P < 0.01) in favour of the SYSF and Western medicine arm, with an I2 of 28% (fig. 4), suggesting that patients receiving SYSF and Western medicine recover from fatigue sooner after the initiation of treatment.

Persistence of fatigue post treatment between combined therapy vs Western treatment alone
2. Duration of fever
Four studies reported this outcome and were analysed - Cheng et al., 2020; Li et al., 2020; Lv et al., 2020 and Zhang et al., 2020.
The total population analysed comprised 259 patients, 148 in the SYSF and Western medicine arm, and 111 in the Western medicine alone arm. This gave a statistically significant mean difference of -1.18 (95% CI -1.45 to -0.91, P < 0.01) in favour of the SYSF and Western medicine arm, with an I2 of 46% (fig. 5), suggesting that patients receiving SYSF and Western medicine had fevers for a shorter duration.

Duration of fever between combined therapy vs Western treatment alone.
In addition, we performed subgroup analyses of prospective and retrospective studies separately.
The prospective studies comprised only Li et al., 2020 thus meta-analysis was not conducted. This study had 60 patients, 30 in the SYSF and Western medicine arm, and 30 in the Western medicine alone arm. This gave a statistically significant mean difference of -1.51 (95% CI -1.92 to -1.09, P < 0.01) in favour of the SYSF and Western medicine arm (Fig. 5), suggesting that patients participating in studies performed prospectively and received SYSF and Western medicine had fevers for a shorter duration.
The retrospective studies analysed were Cheng et al., 2020; Lv et al., 2020 and Zhang et al., 2020 comprising 199 patients, 118 in the SYSF and Western medicine arm, and 81 in the Western medicine alone arm. This gave a statistically significant mean difference of -0.94 (95% CI -1.29 to -0.59, P < 0.01) in favour of the SYSF and Western medicine arm, with an I2 of 46% (Fig. 5), suggesting that patients who participated in studies performed retrospectively and received SYSF and Western medicine had fevers for a shorter duration.
3. Persistence of other symptoms post treatment
Five studies reported this outcome and were analysed - Cheng et al., 2020; Duan et al., 2020; Lv et al., 2020; Wang et al., 2020 and Yao et al., 2020.
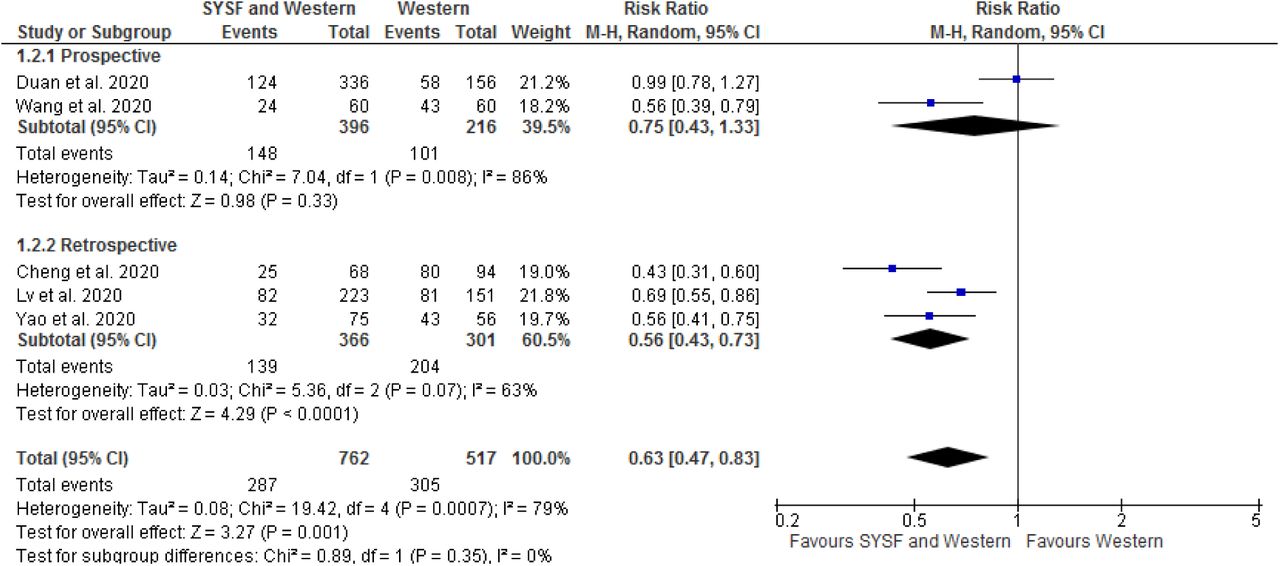
The total population analysed comprised 1279 patients, 762 in the SYSF and Western medicine arm, and 517 in the Western medicine alone arm. This gave a statistically significant risk ratio of 0.63 (95% CI 0.47 to 0.83, P < 0.01) in favour of the SYSF and Western medicine arm, with an I2 of 79% (Fig. 6), suggesting that patients receiving SYSF and Western medicine had symptoms such as headache, gastrointestinal symptoms, myalgia, dyspnea and chest tightness for a shorter duration.

Persistence of other symptoms post treatment between combined therapy vs Western treatment alone.
In addition, we performed subgroup analyses of prospective and retrospective studies separately.
The prospective studies analysed were Duan et al., 2020 and Wang et al., 2020 comprising 612 patients, 396 in the SYSF and Western medicine arm, and 216 in the Western medicine alone arm. This gave a risk ratio of 0.75 (95% CI 0.43 to 1.33, P = 0.33) with an I2 of 86% (Fig. 6), suggesting no statistically significant difference in the persistence of symptoms between the two arms in studies performed prospectively.
The retrospective studies analysed were Cheng et al., 2020; Lv et al., 2020 and Yao et al., 2020 comprising 667 patients, 366 in the SYSF and Western medicine arm, and 301 in the Western medicine alone arm. This gave a statistically significant risk ratio of 0.56 (95% CI 0.43 to 0.73, P < 0.01) in favour of the SYSF and Western medicine arm, with an I2 of 63% (Fig. 6), suggesting that patients who participated in studies analysed retrospectively and received SYSF and Western medicine had symptoms such as headache, gastrointestinal symptoms, myalgia, dyspnea and chest tightness for a shorter duration.
4. Adverse reactions
Four studies reported this outcome and were analysed - Duan et al., 2020; Li et al., 2020; Lv et al., 2020 and Zhang et al., 2020.
The total population analysed comprised 328 patients, 197 in the SYSF and Western medicine arm, and 131 in the Western medicine alone arm. This gave a risk ratio of 1.62 (95% CI 0.83 to 3.17, P = 0.16) with an I2 of 80% (Fig. 7), suggesting that there is no statistically significant difference in reported adverse reactions between the two arms.

Adverse events during the management of patients
In addition, we performed subgroup analyses of prospective and retrospective studies separately.
The prospective studies analysed were Li et al., 2020 and Duan et al., 2020 comprising 183 patients, 112 in the SYSF and Western medicine arm, and 71 in the Western medicine alone arm. This gave a statistically significant risk ratio of 5.32 (95% CI 1.55 to 18.28, P = 0.006) in favour of the Western medicine alone arm, with an I2 of 87% (Fig. 7), suggesting that patients participating in studies performed prospectively who received SYSF and Western medicine reported more adverse events.
The retrospective studies analysed were Lv et al., 2020 and Zhang et al., 2020 comprising 145 patients, 85 in the SYSF and Western medicine arm, and 60 in the Western medicine alone arm. This gave a risk ratio of 0.39 (95% CI 0.14 to 1.06, P = 0.06) with an I2 of 62% (Fig. 7), suggesting that there is no statistically significant difference in adverse events reported by patients in the two arms in studies performed retrospectively.
5. Duration of hospitalisation
Two studies reported this outcome and were analysed - Li et al., 2020 and Zhang et al., 2020.
The total population analysed comprised 96 patients, 49 in the SYSF and Western medicine arm, and 47 in the Western medicine alone arm. This gave a mean difference of -0.73 (95% CI -5.19 to 3.73, P = 0.75) with an I2 of 91% (Fig. 8), suggesting that there is no statistically significant difference in the duration of hospitalisation between the two arms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hospitalization duration between combined therapy vs Western treatment alone
Discussion
This review evaluates the effectiveness of SYSF in the management of COVID-19 symptoms. We describe the individual components of SYSF as shown in table 1.
Formula J
In this review, it showed that Formula J combined with conventional treatment of COVID-19 can effectively improve fever, cough, fatigue, sputum production, and relieve patient anxiety. (Table 2). Looking at hospitalisation rate and improvement of other symptoms such as headache, sore throat, rhinorrhoea and nausea, there was no statistical difference between the treatment group and the control group. However, there is a significant difference in regards to adverse events experienced by the treatment group. 32.39% of the patients in the treatment group developed diarrhea symptoms in this study, as compared to 0% of patients in the control group experiencing adverse events. This may be due to the high dose of Formula J used in this study (2 sachets of 5g each time, 3 times a day), as compared to the usual dose of 1 sachet of 5g each time, 3 times a day.32 There is no research comparison of the degree of adverse reactions caused by high and low doses of Formula J, and whether diarrhea is an adverse reaction of Formula J is still to be further discussed. Although Formula J may meet current treatment needs, it should be pointed out that there are still deficiencies as patients in the study were not treated according to syndrome differentiation. Treatment using Formula J based on syndrome differentiation is a potential direction for further research.
Formula L
Comparing 4 different papers on Formula L (Table 3), the treatment groups in all 4 papers demonstrated a faster recovery of fever, cough and fatigue. Formula L was also effective in the normalization of inflammatory markers like CRP and ESR, as well as both lymphocyte and neutrophil count. Importantly, Lv et al showed no statistical difference in terms of adverse events between the treatment and control groups. The adverse events that patients in the treatment group experienced are diarrhoea and loss of appetite which subsequently resolved with the stoppage of the management plan, with no long term sequelae. This is a promising first step into the safety aspect of Formula L, and future research can focus in this direction in order to establish the full safety profile of Formula L.
Formula Q
Li et al showed that Formula Q with conventional antiviral management led to significant improvement in terms of resolution of symptoms such as cough and fever (Table 4), and decreased hospitalisation duration as compared to the control group. Resolution of CT Thorax findings was also quicker in the treatment group. There were no statistical differences in the worsening of symptoms between the treatment and control groups, even though the treatment group had fewer patients deteriortating (6 patients in treatment group; 12 patients in control group). Looking at the safety profile of Formula Q, one patient experienced nausea during treatment. This was resolved after the introduction of pantoprazole into the management of this patient.
Formula Xb
Zhang et al demonstrated significant rates of recovery and resolution of CT thorax in the treatment group. (Table 5) There was however, no significant difference in resolution of inflammatory markers and nucleic acid conversion rate across the both groups after treatment. As the criteria for effective recovery stated in the study is defined as an improvement in symptoms, nucleic acid conversion and resolution of CT Thorax, it would suggest that the recovery rate in the treatment group is limited by the nucleic acid conversion rate. In addition, there was no significant difference in adverse events as compared to the control group. As such, it would be an interesting research direction to study the mechanism of action of Formula Xb, especially on its potential impact on ARDS in other diseases.
Overall analysis of SYSF and Western treatment
The combination of Formula L and Western interventions led to a speedier and more favourable outcome in the treatment of COVID-19 patients, specifically for symptoms like fever, cough and fatigue. (Fig. 2-4) Low heterogeneity was observed in the three studies done.
In addition, the combination of Formula L or Q with Western interventions resulted in a shorter duration of fever, and improvement of various other symptoms such as musculoskeletal pain, nausea, vomiting, rhinorrhoea and chest tightness. Similar results were not shown in Formula J and Xb. (Fig. 5-6)
In terms of overall safety profile, more research would have to be done in terms of interaction between SYSF and Western medications, specifically Formula J. The prospective study done by Duan et al showed a statistically significant increase in adverse events in the treatment group as compared to the control group. (Table 2) This might suggest possible interactions between Formula J and western medications.
The study done by Lv et al. showed a lower rate of adverse effects when Formula L was used in conjunction with western medications as opposed to a higher rate when Formula Xb was used demonstrated by Zhang et al.. (Fig. 7) However, as a whole, there was no statistical significant difference in adverse events between the combined SYSF and Western interventions compared to Western interventions alone. (Fig. 7).
There was no significant difference to the duration of hospitalisation between combined SYSF and Western interventions as compared to Western interventions alone. (Fig. 8) However when the data was further analysed, Formula Q (T: -2.80 days) as opposed to Formula Xb (T: +1.70 days) resulted in shorter stay within the hospital. Both papers reported a high degree of heterogeneity when comparing the duration of hospitalisation between the treatment and control group.
This review is limited by the lack of randomised control trials and prospective studies for each formula in SYSF. This is expected due to the ongoing and sudden pandemic of COVID-19, making trials difficult to conduct due to the lack of manpower available. This is compounded by new formulas that have been specifically concocted for COVID-19. As such, a mixed method review was employed, analysing both prospective and retrospective studies with a comparator. Even though there is high heterogeneity among the analysed papers due to different formulas being studied, we can use these papers to understand the overall effects of SYSF on patients with COVID-19 from multiple angles.
In this review, Formula L and Q showed promising results on the management of symptoms of COVID-19 patients with possibly lower levels of adverse events when combined with Western medications. Formula J and Xb do not appear to be effective, and might result in an increased number of adverse events and duration of stay when used. Further studies including a larger cohort size should be included to further evaluate the effects and safety of SYSF.
Data Availability
NA
Footnotes
Copyright: The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a world-wide licence to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future), to i) publish, reproduce, distribute, display and store the Contribution, ii) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or, abstracts of the Contribution, iii) create any other derivative work(s) based on the Contribution, iv) to exploit all subsidiary rights in the Contribution, v) the inclusion of electronic links from the Contribution to third party material where—ever it may be located; and, vi) licence any third party to do any or all of the above.
Competing Interest Statement: All authors have completed the Unified Competing Interest form and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Contributor Detail:
Guarantor: Zhang Yong Tai
Planning of review was done by all authors.
Searching for articles in all databases was done by all authors.
Statistical analysis was done by all authors
All authors played a vital role in the writing of the report
Pang Ong Wong is responsible for proofreading of the report.
Transparency declaration: The lead author affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Ethical Approval: No ethical approval is needed for this review.
Funding: There is no funding for this paper.



