
ABSTRACT
Background Steroid hormones are essential signaling molecules in prostate cancer (PC). However, many studies focusing on liquid biomarkers fail to take hormonal status of these patients into account. Because steroid measurements are sensitive to bias caused by matrix effects, thus assessing potential matrix effects is an important step in combining ctDNA analysis with hormone status.
Methods We investigated the accuracy of multi-steroid hormone profiling in mechanically-separated plasma tubes (MSP) and in CellSave Preservative plasma tubes (CS), that are typically used to obtain ctDNA. We performed multiplex steroid profiling in samples obtained from ten healthy controls and ten castration-resistant prostate cancer patients
Results Steroid measurements were comparable between the MSP and serum tubes. A small but consistent decrease of 11 – 18% compared to serum was observed in CS tubes, which was considered to be within the acceptable margin. The minimally residual testosterone levels of castrate patients could be sensitively quantified in both CS and MSP samples.
Conclusions We validated the use of MSP and CS tubes for multi-steroid profiling by LC-MS/MS. The optimised use of these samples used in clinical trials will allow us to gain further insight into the steroid metabolism in PC patients.
INTRODUCTION
Prostate cancer is a steroid-hormone dependent disease where androgens play a pivotal role in the evolution of the disease. Targeting the androgen signaling pathway through androgen deprivation therapy (ADT) in locally advanced and metastatic prostate cancer is a highly effective way to inhibit tumour growth1. However, tumour cells will eventually become resistant to these low androgen concentrations and show disease progression. Resistance mechanisms include androgen receptor (AR) modifications, like mutations and overexpression2,3, and changes in androgen biosynthesis and metabolism, thereby increasing intratumoural androgen availability4-6. The continued importance of the androgen signaling pathway in castration-resistant prostate cancer (CRPC) is underlined by the survival benefits observed with second-line therapies such as the anti-androgen enzalutamide and adrenal steroidogenesis inhibitor abiraterone 7-10. Circulating steroid levels are measured to verify efficacy of hormonal treatment and have a prognostic value in patients with prostate cancer11-13.
The assessment of circulating steroid hormones relies heavily on sensitive, specific and accurate measurement techniques, especially at castrate levels. Liquid-chromatography tandem mass spectrometry (LC-MS/MS) combines multi-steroid profiling capabilities with superior sensitivity and specificity14,15 over older techniques16,17, while maintaining high sample throughput18,19. Extensive MS-based steroid panels have been successfully developed in recent years to improve the detection and diagnosis of disorders associated with abnormal steroid hormones concentrations20-23.
Steroid measurements are predominantly performed in serum samples. Previous LC-MS/MS studies have shown that steroids can be quantified reliably across different blood matrices24-26, but there are differences observed between plasma and serum, glass and plastic tubes, or when using tubes with different stabilizing agents or with gel-separators24-29. Consequently, alternative collection tubes and extraction methods must be validated before they can reliably be used for steroid profiling.
The use of CellSave (CS) tubes in population- and patient-based cohorts has grown as this specialised ‘cell-stabilizing’ blood collection tube preserves both circulating tumour cells (CTCs) and cell-free circulating tumour DNA (ctDNA)30,31. These biomarkers allow for the assessment of tumour cell genomic characteristics such as genomic instability in these patients32. These samples are now extensively collected in (cancer) biobanks and could potentially also be used to measure patient steroid profiles.
Mechanical separation methods of blood are similarly gaining popularity in clinical chemistry due to their easy applicability compared to those that use a separation gel. The BD Vacutainer Barricor is amechanically-separated plasma (MSP) tube, and it has shown no obvious bias in steroid hormone measurements versus a gel-based plasma tube in a single study33, but this was confined to a select number of five steroids, warranting further investigation.
Previous studies have identified matrix effects, interference caused by a contaminant from serum or collection tube that leads to false high or low quantification, as a potential source of bias25,26,28, and it is therefore imperative to assess the quality of steroid measurements in CS tubes and MSP tubes. In this study, we aimed to determine if plasma obtained with these tubes is suitable for multiplex steroid profiling. To this end, we performed LC-MS/MS analysis on serum obtained with standard SST™ II Advance Vacutainer® tubes and plasma samples obtained with MSP and CS tubes from healthy control (HC) subjects and patients with CRPC.
RESULTS
Comparison of blood collection tubes
Baseline characteristics of the study participants are shown in Table 1. Circulating steroid levels of 16 steroids were determined by LC-MS/MS in 10 HCs and 10 mCRPC patients in all three collection tubes. Quantification and concentration ranges for the steroids are reported in Table 2. Most steroids could be quantified in healthy controls at the level of the lowest calibration sample (0.25 ng/ml), with the exception of androstenedione (0.5 ng/ml), DHEA (1 ng/ml) and DHT (1 ng/ml). Serum DHEA values below the LLOQ were detected (HC: n =1, CRPC: n = 4) and excluded from further analysis.
Abbreviations: mCRPC – metastatic castration-resistant prostate cancer
Relative differences are shown as mean ± SD. Statistical analysis was performed by repeated measurement 1-way ANOVA with post-hoc Dunnett’s Test. *p<0.05, ** p<0.01, ***p<0.001. Abbreviations: CS – CellSave Preservative, DHEA – dehydroepiandrosterone, DHT – dihydrotestosterone, HC – Healthy Control, mCRPC – metastatic castration-resistant prostate cancer, MSP – mechanically seperated plasma tube
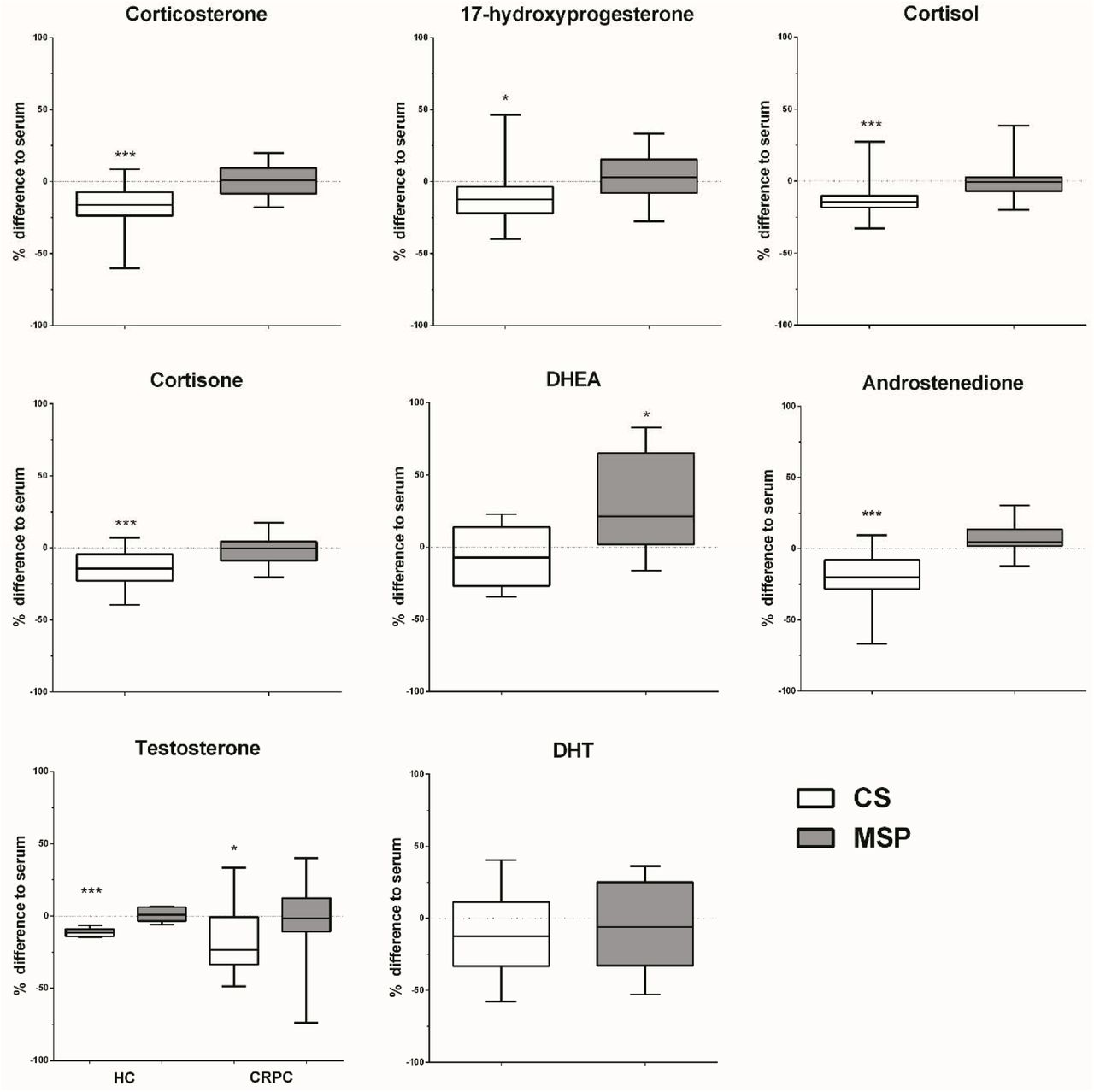
The values observed in MSP samples were comparable to those found in serum for most steroids. The only exception was DHEA, which was higher (21.3 % ± 32.9 % p<0.05) in the MSP samples than in serum (Figure 1). In CS samples, significantly lower concentrations compared to serum were observed for corticosterone (-16.2 % ± 15.2 %, p<0.01), 17-hydroxyprogesterone (-11.0 % ± 20.03 %, p<0.05), cortisol (-13.2 % ± 13.0 %, p<0.001), cortisone (-14.4 % ± 13.1 %, p<0.001), androstenedione (-18.4 % ± 13.6 %, p<0.01). No significant differences were found for DHEA compared to serum.

Steroid concentrations from serum, CS and MSP samples obtained from ten healthy controls and ten mCRPC patients measured by LC-MS/MS. Relative difference of CS and MSP measurements compared to serum is shown. *p<0.05, **p<0.01, ***p<0.001, compared to serum matrix. Repeated Measurements 1-way ANOVA with post-hoc Dunnett’s Test. Abbreviations: CS – CellSave Preservative, DHEA – dehydroepiandrosterone, HC – Healthy Control, mCRPC – metastatic castration-resistant prostate cancer, MSP – mechanically seperated plasma tube
Similar steroid concentrations between HC and mCRPC subjects were observed for corticosterone, cortisol and cortisone (Figure 2). Lower concentrations were observed for 17-hydroxyprogesterone, androstenedione and testosterone in mCRPC subjects. This was likely due to a combination of castration (testosterone) and age-related effects, as the mCRPC subjects were older than those the healthy control subjects.

Steroid hormone concentrations in healthy controls (n = 10) and mCRPC patients (n = 10). Four patients received no additional treatment, four received antiandrogens (enzalutamide (n=3) or apalutamide (n=1)), one received abiraterone and prednisone and one received prednisone. Line and error represent mean ± SEMs. Abbreviations: 17OHP – 17-hydroxyprogesterone, A4 – androstenedione, B – corticosterone, DHEA – dehydroepiandrosterone, CRPC – castration-resistant prostate cancer, E – cortisone, F – cortisol, T – testosterone
Androgen levels in mCRPC patients are >10 fold lower than in healthy men due to ADT, requiring sensitive techniques to accurately measure residual androgens. The calibration series was expanded to include lower concentrations (0.01 – 0.25 ng/ml) to allow quantification of castrate testosterone levels.
Accurate quantification at 0.01 ng/mL was achieved for testosterone. Similar to the other steroids, lower testosterone concentrations compared to serum were detected in CS samples, but not in MSP samples, at normal HC concentrations (-11.5 % ± 2.8 %, p<0.001) and at castrate concentrations (-16.9 % ± 24.2 %, p<0.05) (Figure 1). Low signal-to-noise ratios limited the reliability of DHT quantification which could not be accurately quantified in the CRPC subjects with our assay.
Correlation of steroid measurements between matrices
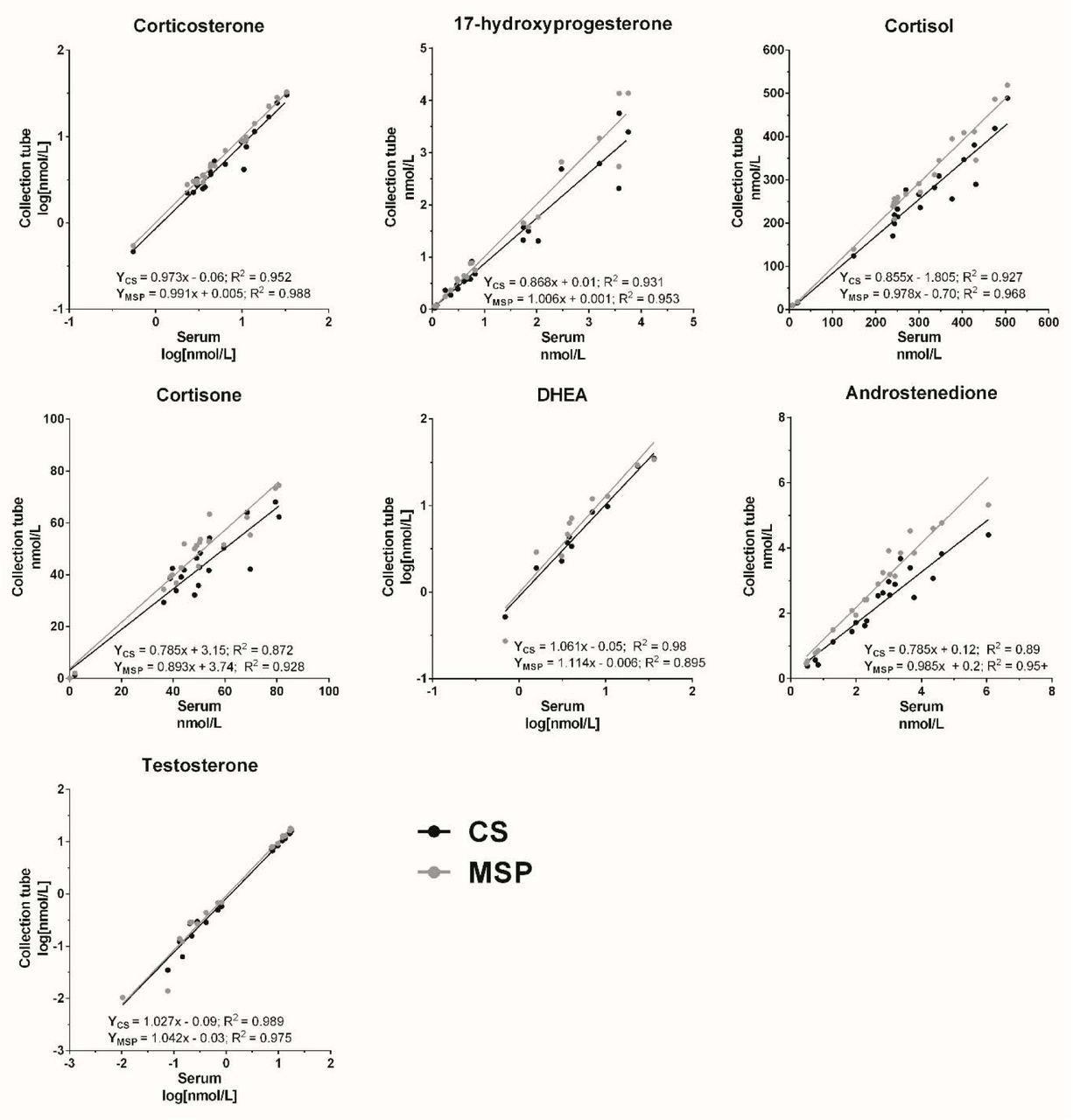
The correlations between results obtained MSP and CS samples, respectively, compared to those obtained in serum were determined by linear regression (Figure 3). For the DHT analysis only HC samples were included. Corticosterone, DHEA and testosterone were normally distributed after log-transformation. Significant correlation (p<0.001) between both matrices and serum was observed for corticosterone, 17-hydroxyprogesterone, cortisol, DHEA and testosterone. High correlation was also observed for cortisone and androstenedione, but with a more than 20% deviation from the optimal slope (p<0.05) with the CS matrix: both 0.79x. The analysis also revealed a poor correlation for DHT between CS and serum (R2 = 0.60) and between MSP and serum (R2 = 0.45).

{kind=link}
{kind=link}
{kind=link}
Linear regression analysis between serum and CellSave measurements and between serum and MSP measurements in healthy controls and mCRPC patients combined. Corticosterone, DHEA and testosterone values did not pass normality testing (D’Agostino and Pearson), but did so after logarithmic transformation. Abbreviations: CS – CellSave Preservative Tube, DHEA – dehydroepiandrosterone, MSP – mechanically separated plasma tube.
DISCUSSION
In this study, we investigated whether collected samples that are abundantly present in biobanks obtained from PC patients such as mechanically separated plasma or CS-derived plasma are suitable for multiplex steroid profiling by LC-MS/MS. We compared them to the current standard collection method using SST™ II Advance Vacutainers. We showed that measurements in MSP are equal to serum. When collecting in CS tubes 11-18% lower concentrations were observed for all steroids. The Guideline on Bioanalytical Method Validation (2011) of the European Medicines Agency advises that accuracy must be within 15 % of the nominal concentration and within 20 % at the LLOQ34. The decreases observed for most steroids in CS tubes using serum as a reference were within this acceptable range (Table 2). Therefore, we conclude that CS samples are suitable for steroid profiling, which can be combined with analysis of CTCs or ctDNA. However, caution is advised when interpreting results obtained in CS samples against reference values that were obtained in serum, and direct comparison to samples collected in other tubes should be avoided. Nevertheless, these findings may reduce patient burden and open up the possibility to add detailed steroid profiling of large collections of biomaterial already collected for ctDNA analysis.
In this study, most steroids could be quantified accurately within the range of the calibration series. Most of the Δ4-steroids, such as cortisol or testosterone, ionise more easily and so can be accurately quantified at low levels (0.03 – 0.15 nM). This allows for the quantification of testosterone in mCRPC patients (typically <0.5nM)11. Δ5-steroids such as DHEA and saturated steroids such as DHT are poor ionisers and quantification at lower concentrations is beyond the sensitivity of the mass spectrometer22. Like testosterone, DHT levels are suppressed in castrated patients and the concentrations in these patients could not be accurately assessed. DHEA levels in men decline with age35, and the mCRPC subjects in this study were older than the HC subjects. Consequently, values below the LLOQ were detected in four CRPC patients and were excluded from the analysis. Derivatization, for example to form an oxime, increases ionizability, and therefore sensitivity allowing low level quantification of Δ5- and 5a-reduced steroids22. However, the derivatization method is not suited for routine clinical diagnostic measurements due to increased sample preparation time and cost. In addition to this, fragmentation produces multiple derivatives for some steroids adding to the complexity of the analysis.
Matrix effects and cross-reactivity are established sources of interference in steroid hormone profile studies with immunoassay and LC-MS/MS24-29. Previous studies have identified the type of blood sample tube as a potential source of interference. MSP tubes like BD Vacutainer Barricor utilise mechanical separation which makes them easily applicable, but the accuracy of steroid hormone measurements in these tubes has not been validated. One study33 showed no differences to gel-based plasma tubes, but these measurements were performed on a single platform with a limited number of steroids, namely cortisol, DHEAS, oestradiol, progesterone, and testosterone. Our study shows that multi-plex steroid quantification in MSP sample tubes is comparable to the reference serum tubes. We detected no significant differences, with the exception of DHEA. This seemed to be largely driven by samples in the HC group. Quantification of DHEA at low concentrations with LC-MS/MS remains a challenge as its structure contributes to poor MS ionization22,36. This challenge could be overcome by using a more sensitive mass spectrometer or with the use of derivatization. Prior to using MSP tubes for clinical studies however, full validation looking at accuracy, precision and recovery is recommended.
CS tubes are optimised for the measurement of circulating nucleic acids or tumour cells30,31. The use of this matrix for liquid biopsies has increased exponentially over the last years due to the successful genomic characterization of CTCs or free circulating nucleic acids, but no studies have investigated if CS tubes are suitable for quantification of circulating steroid hormone levels. Our experiments indicate that steroid measurements in CS tubes are affected by a mild bias which resulted in an approximate 10 – 20% decrease compared to serum. We observed similar effects in both HCs and mCRPC subjects. CS tubes contain 300 μl of Na2EDTA anticoagulant as well as an undisclosed preservative to stabilise cells in the sample. Due to the presence of the Na2EDTA there may be an inherent dilution of the sample, which amounts to approximately 3-4 % on a 7.5 – 10 ml volume. This dilution factor is insufficient to account for the difference in circulating steroid hormone levels however. Consequently, it is possible that other factors also contribute towards the observed difference.
This decrease was observed across a variety of different polarity steroids with different molecular weights. It is therefore unlikely that the preservative co-elutes with one of the steroids and suppresses the MS signal. Either there is an unidentified contaminant in the tubes which affects all steroids or the steroids themselves are being retained/bind to the tube itself. Steroids have been long recognised to stick to plastics37, which may contribute to the lower values in CS samples.
Currently, CS tubes are most commonly utilised in oncological studies to obtain CTCs and ctDNA. Hormonal treatment options in breast and prostate cancer involve potent suppression of oestrogens or androgens. For example, inhibition of testicular steroidogenesis by ADT will typically lower testosterone levels by >90 %11. Interpretation of such changes is unlikely to be affected by the difference observed in CS samples. Especially within the context of a single study the relative difference should affect all samples identically as long as a single collection tube is used. As such, the observed difference is acceptable for most clinical purposes, including the use of CS samples for steroid profiling in prostate cancer patients. Steroid profiles and analysis of CTCs or ctDNA investigation will decrease costs and reduce patient burden.
In conclusion, mechanically-separated plasma samples are suitable for steroid quantification, including castrate range of androgens. Similarly, CellSave samples are suitable for steroid measurements, although there is a consistent bias of –11-18% lower steroid hormone levels. Because of this, all samples in a research study should be collected in the same sample tubes to avoid potential variation due to effects from the tubes themselves.
MATERIALS AND METHODS
Subjects
At the Erasmus MC Cancer Institute in Rotterdam, The Netherlands, healthy controls (HCs) and patients were included within study EMC-2016-761, which was approved by the medical ethical committee of our institute. HCs were all adult male subjects. Patients were adult subjects with metastatic castration-resistant prostate cancer (mCRPC), treated with ADT. Patients were eligible to start treatment with or were currently treated with second-line hormonal therapy (abiraterone with prednisone, enzalutamide or apalutamide). For all subjects the following exclusion criteria were applied: 1) endocrine disease with altered activity of the hypothalamic-pituitary-adrenal or hypothalamic-pituitary-gonadal axis; 2) the use of medications, excluding those used to treat prostate cancer, that interfered with circulating steroid levels or dysregulated the hypothalamic-pituitary-adrenal or hypothalamic-pituitary-gonadal axis. All subjects provided written informed consent before any study procedure.
Samples
Blood was collected from HCs and mCRPC patients in SST™ II Advance Vacutainer® (serum; BD, Franklin Lakes, NJ, USA), Barricor Vacutainer® (BD) and CellSave Preservative (Menarini Sillicon Biosystems Inc, Huntington Valley, PA, USA) blood collection tubes. All samples were processed within 96 hours after blood collection. All tubes were centrifuged at 1,711g for 10 minutes at room temperature. Plasma from CellSave tubes was subsequently centrifuged at 12,000g for 10 minutes at 4°C. Samples were stored at - 80°C until extraction.
Steroid extraction
Calibration series (0.25 ng/ml – 500 ng/ml for HC, and 0.01 ng/ml – 500 ng/ml for mCRPC) were prepared in phosphate buffered saline (PBS) with 0.1% bovine serum albumin (BSA) or in charcoal-stripped pooled human serum (Goldenwest Diagnostics, Temecula, CA, USA). Steroids investigated were 17-hydroxyprogesterone, androstenedione, cortisol, cortisone, corticosterone, dehydroepiandrosterone (DHEA), dihydrotestosterone (DHT) and testosterone. The stripped-serum calibration series was used to quantify all steroids with the exception of androstenedione, due to a high background signal in stripped serum but not in PBS-BSA. An internal standard solution was prepared in methanol/water 50/50 with equal concentrations (1 μg/ml) of the following deuterated steroids: 17-hydroxyprogesterone-d8, cortisol-d4, corticosterone-d8, DHEA-d6, DHT-d3, testosterone-d3. All steroids were obtained from Sigma Aldrich, UK.
400 μl of sample was transferred to hexamethyldisilazane-treated (Thermo Fisher) glass tubes (VWR, Amsterdam, The Netherlands). 20 μl of the internal standard solution was added and all samples were thoroughly vortexed. Liquid-liquid extraction was performed by adding 2 ml methyl-tert butyl ether (MTBE, Sigma Aldrich, Zwijndrecht, The Netherlands) to each tube and vortexing. The samples were left at room temperature for 30 minutes to allow phase separation. The upper organic layer was transferred and the MTBE was evaporated under nitrogen at 50° C. The samples underwent a second liquid-liquid extraction with 2 ml MTBE. Samples were reconstituted in 125 μl LC-MS grade 50% methanol (CHROMASOLV, Sigma Aldrich, Zwijndrecht, The Netherlands) before measurement.
LC-MS/MS
Steroid concentrations were measured by mass spectrometry (Xevo TQ-XS, Waters, Milford, MA, USA) after separation on an ACQUITY uPLC (Waters) with a Waters HSS T3 column (2.1 mm × 50 mm, 1.8 μm, Waters)38-43. The mobile phases consisted of water (A) and methanol (B) both with 0.1% formic acid and a 5-minute linear gradient was used (45 – 75% B) with a flow rate of 0.6 m l/min. The multiple reaction monitoring settings and validation of these LC-MS/MS methods were previously reported38,42. Steroids were quantified against the linear calibration series relative to an internal standard and were only included in the final analysis if the calibration series R2 was > 0.99 and appropriate lower limits of quantification were reached. The lower limit of accurate quantification (LLOQ) was set to the lowest calibration concentration that had a clearly defined peak and a signal-to-noise ratio > 10. Samples with concentrations below the LLOQ were detectable, but not accurately quantifiable.
Statistics
LC-MS/MS raw data was processed using MassLynx (v4.1, Waters). Statistical analysis was performed using GraphPad Prism (Version 5). Normality of data was analysed with D’Agostino & Pearson’s test. Comparisons of steroid hormone concentrations across the blood collection tubes were performed with repeat measurements 1-way ANOVA with post-hoc Dunnett’s test. Correlations in hormone levels were determined by linear regression. Group concentrations and differences are shown as mean ± SD, unless specified otherwise. P values were considered significant if <0.05.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Information
These authors contributed equally: Gido Snaterse and Lisanne F van Dessel.
Author Contributions
G.S. performed the LC-MS/MS experiments, data analysis, prepared figures/tables and wrote the manuscript. L.F.D. collected the patient samples, performed data analysis, prepared figures/tables and wrote the manuscript. A.E.T. oversaw the LC-MS/MS experiments and analysis of the data, and critical revision of the manuscript. W.A. was involved in interpretation of the data and critical revision of the manuscript. M.P.L. was involved in the design of the work, collection of the samples and critical revision of the manuscript. J.A.V and J.H. were involved in the design of the work, interpretation of the data, critical revision of the manuscript.
All authors reviewed and approved the final version of the manuscript.
Conflict of Interest
M. P. L. is the recipient of grants of Sanofi, Johnson & Johnson and Astellas. Other authors did not declare a conflict of interests.
Acknowledgements
Funding for this project was provided by the Daniel den Hoed foundation.
The authors thank the volunteers and patients who made this study possible.
General Abbreviations
- ANOVA
- Analysis of variance
- CRPC
- Castration resistant prostate cancer
- CS
- CellSave Preservative tube
- CTC
- Circulating tumour cell
- ctDNA
- circulating tumour DNA
- HC
- Healthy Control
- LOQ
- Limits of quantification
- MS
- Mass spectrometry
- MSP
- Mechanically separated plasma tube
- MTBE
- Methyl-tert butyl ether
- PC
- Prostate cancer
- S/N
- Signal-to-noise
- LC-MS/MS
- Liquid chromatography tandem mass spectrometry
- PBS-BSA
- phosphate-buffered saline with bovine serum albumin
Steroid abbreviations
- 17OHP
- 17-hydroxyprogesterone
- A4
- Androstenedione
- B
- Corticosterone
- DHEA
- Dehydroepiandrosterone
- DHT
- Dihydrotestosterone
- E
- Cortisone
- F
- Cortisol
- T
- Testosterone
References



