
Abstract
Introduction Diabetes mellitus (DM) is a metabolic disorder with inappropriate hyperglycemia either due to an absolute or relative deficiency of insulin secretion or reduction in the biologic effectiveness of insulin or both. An inflammatory basis for Diabetes & its complications has attracted interest. Among several markers of inflammation, C reactive protein (CRP) is found to be significant in people with diabetes. Diabetic nephropathy may be associated with abnormally high levels of CRP.
Materials & Methods This study was performed for 1 year over 100 type 2 diabetic patients (n=100) aged 30-70 years in Calcutta National Medical College & Hospital. Necessary clinical & Diabetes related laboratory investigations were done as the routine procedure.
Results Among 100 study population, all macro-albuminuria patients were found to have high CRP. 63% of Stage 3 chronic kidney disease (CKD) patients were having high CRP in our study. High CRP values were also found among patients with higher spot urine ACR (329.50±259.40 mg/gram).(P<0.05)
Conclusion CRP is a marker which increased in inflammatory reactions. Low grade inflammation as indicated by high CRP was an important predictor of diabetic nephropathy.
Introduction
Diabetes mellitus (DM) is a metabolic disorder with inappropriate hyperglycemia either due to an absolute or relative deficiency of insulin secretion from beta cells of langerhans of endocrine part of pancreas or reduction in the biologic effectiveness of insulin or both or the outer receptors are malfunctioning. It is one of the most common non-communicable diseases worldwide and is a growing concern. Diabetes prevalence had increased by 64% across India over the last quarter century according to November 2017 report by Indian Council for Medical Research, Institute for Health Metrics and Evaluation, both research institutes and the Public Health Foundation of India, an advocacy. Genetics, Aging, Obesity, Lifestyles & many other factors have contributions to the development of Diabetes and its complications. Nevertheless an inflammatory basis for Diabetes and its complications has attracted interest. Among several markers of inflammation, hs–CRP is found to be significant in people with diabetes. CRP, a pentameric protein produced by the liver has emerged as the ‘golden marker for inflammation’. Proteinuria is a marker of vascular endothelial damage. Additionally, it is reported that high serum levels of CRP is a novel cardiovascular risk factor that impairs endothelial function. So diabetic nephropathy may be associated with abnormally high levels of CRP.
Diabetic nephropathy is a leading cause of CKD, end stage renal disease(ESRD). It is diagnosed based upon the detection of proteinuria in diabetic patients in absence of other obvious cause such as infection1.
Definition of diabetic nephropathy by albuminuria2:
In our study, we used spot urinary albumin-Creatinine ratio for detection of albuminuria. We tested spot urine sample after excluding conditions that could transiently increase albumin excretion and same test was repeated 2 times at three months interval. If two out of three tests were positive, we considered the people having diabetic nephropathy.
Non-diabetes related conditions that might increase albuminuria are urinary tract infection(UTI), haematuria(RBC>5 RBC/hpf), prostate disease, heart failure, febrile illness, severe hypertension and vigorous exercise.
Microalbuminuria and macroalbuminuria may be present when patient is diagnosed of having type 2 DM first reflecting its long asymptomatic period. To institute effective therapy at an early stage, albuminuria should be detected. But some individuals with type 1 and type 2 DM have a decline glomerular filtration rate (GFR) in the absence of albuminuria. So measurement of the serum Creatinine & estimation of GFR should also be performed.
For patients with type 2 diabetes mellitus in NHANES III (THIRD NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY; n=1197), low GFR (60 ml/min/1.73 m2) was present in 30% of patients in absence of micro or macroalbuminuria and retinopathy3.
GFR can be measured by specific techniques, example-lnulin clearance. But the recommended equation by the National Kidney Foundation is that of the MDRD (Modified Diet In Renal Disease):estimated GFR (ml/min/1.73m2)=186* (Serum creatinine in mg/dl)-1.154 *(age in years)-0.203. In female, it should be multiplied by 0.742.
Compared to MDRD formula, Inulin clearance slightly overestimates the glomerular functions. In early stage of renal disease, Inulin clearance may remain normal due to hyperfiltration in the remaining nephrons4.
GFR can also be accurately measured using radioactive substances, in particular Chromium-51 and Technetium-99m. These come close to ideal properties of Inulin but can be measured more practically with only a few blood or urine samples5. However we did not use such sophisticated procedures considering the financial burden to the patients.
Stage of chronic kidney disease based on e GFR
But one point should also be noted that glomerular hyperperfusion and renal hypertrophy occur in the first years after the onset of DM and are associated with increase in GFR.
We did not include haemodialysis patients in our study as it was seen that there were some dialysis related alterations in the immune and host defence system. Moreover the type of dialysis membrane had been suggested to play a role. So haemodialysis might exert an impact on C-Reactive protein level.
Creatinine clearance using CockCroft-Gault equation is less accurate. Creatinine clearance (ml/min)= {(140-age in years)* weight in kg}/(72* serum creatinine in mg/dl). It should be multiplied by 0.85 in females. Normal creatinine clearance for healthy men is 97-137 ml/min and for healthy women is 88-128 ml/min6.
Nephropathy may be present due to conditions other than diabetes mellitus in people living with type 2 Diabetes. To establish diabetic nephropathy, some points should be kept in mind.
Duration of diabetes and glycemic status
Presence of hypertension
Associated retinopathy
Absence of haematuria and RBC (red blood cells) casts
Absence of strong family history of kidney disease due to etiology other than diabetes
Absence of rapid rise of creatinine.
We have only included patients clinically and biochemically suspected to have diabetic kidney disease.
Normal blood value of CRP is considered as <4 mg/l according to laboratory reference range of our hospital.
Objectives
To correlate CRP level in relation to normo albuminuria, micro albuminuria and macro albuminuria.
To correlate CRP protein levels with diabetic nephropathy based on estimated glomerular filtration rate.
To assess the influences of various clinical and biochemical factors on development of diabetic nephropathy.
Materials & Methods
Total 100 type 2 diabetic patients (n=100) aged 30-70 years were studied for 1 year in Calcutta National Medical College & Hospital.
Inclusion criteria-Previously diagnosed or recently diagnosed type 2 Diabetes mellitus patients (age 30-70 years) were included in this study.
Exclusion criteria:
Patient with a history of urinary tract infections/ pyelonephritis, nephrolithiasis (kidney or bladder stone), catheterization, severe uncontrolled hypertension(HTN) (> 160/100 mm Hg), sickle cell anaemia, patients on haemodialysis, cancer (prostate, bladder and kidney), benign prostatic hypertrophy, polycystic kidney disease(PKD), prolonged use of analgesics, any recent infection which was caused by an infectious etiology and any type of surgery were excluded from the current study.
Inflammatory processs like systemic lupus erythematosus, inflammatory bowel disease, rheumatoid arthritis, giant cell arteritis, osteomyelitis, rheumatic fever and tuberculosis were also excluded.
▪ Clinical examinations & necessary laboratory investigations were done including blood for CRP, HbA1C, lipid profile, Creatinine and spot urine ACR. CRP was measured by turbidimetry method.
All statistical analyses were performed using Graph Pad Instat software (Version 3.10, 32 bit for Windows). The chi-square test and the Fisher exact test were used to evaluate the differences in proportions between the two groups. One way ANOVA test was used to compare groups for continuous variables. Tukey Kramer Multiple Comparison test was done after ANOVA if results were significant overall to find out which specific group’s mean was different. P-value <0.05 was taken as the level of significance.
Results
Table 3 & Figure 1 are showing distributions of CRP among patients with proteinuria in our study population. Of 17 patients having normoalbuminuria, 16 patients were having normal CRP (94.12%). Of 28 patients having macroalbuminuria, all were having raised CRP (100%). However raised CRP was found in 26 patients out of 55 patients having microalbuminuria (47.3%). (P<0.05)

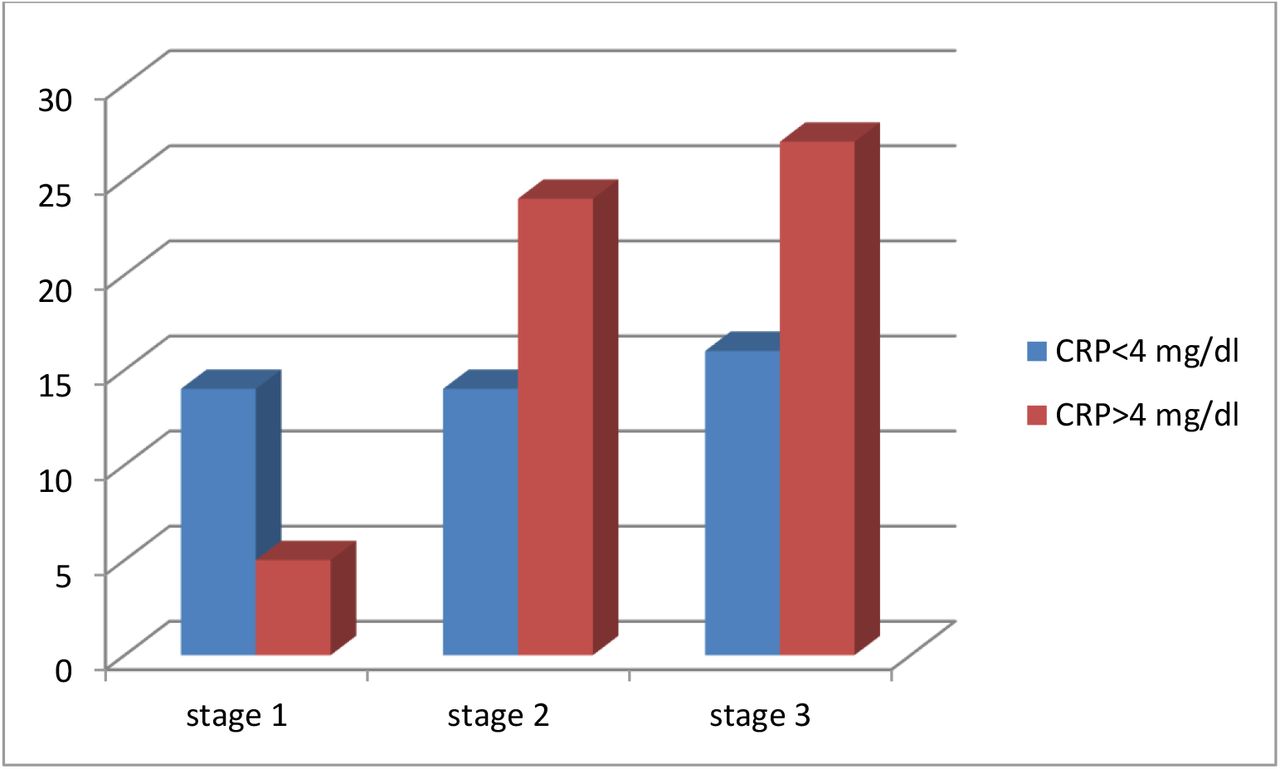
Table 4 & Figure 2 are showing 26.3% of Stage 1 chronic kidney disease patients were having high CRP. 63% of Stage 2 chronic kidney disease patients were having high CRP. 63% of Stage 3 chronic kidney disease patients were having high CRP. (P<0.05) Association of eGFR with CRP was significant.








High CRP values were found in older people (P<0.05) and with higher triglyceride & LDL value (P<0.05). High CRP values were also found among patients with higher spot urine ACR (329.50±259.40 mg/gram) (P<0.05) & with higher creatinine values (P<0.05). However CRP values did not correlate with BMI (P=0.5), HbA1C (P=0.2) (Table 5)
The clinical & biochemical characteristics of diabetic patients with proteinuria were represented in Table 6. Patient with macroalbuminuria (spot urine ACR >300 mg/gm) were older & having higher LDL and Serum creatinine and CRP values in comparison to patient with normal urine ACR (<30 mg/gm).
Proteinuria was significantly associated with age, serum creatinine, LDL and CRP values overall. But further post hoc analysis (Table 7) showed that age had no significant association while comparing normoalbuminuria with microalbuminuria. The data comparing normoalbuminuria & microalbuminuria which were nearly age matched, HbA1c & triglyceride matched, significant rise of CRP was evident in microalbuminuric patients in comparison to normoalbuminuric patients. So CRP may have significant role in early stages of diabetic nephropathy.
Discussion
Acute phase proteins are a class of proteins & their plasma concentrations increase or decrease in response to inflammations. Previous studies had demonstrated that inflammation played an important role in the pathogenesis of DM7-9.
CRP induces impaired self-regulation of glomerular pressure(GP) and dysfunction of glomerular endothelium10. So there is loss of albumin in urine through damaged glomeruli. These observations suggest that low-grade inflammation, reflected by high serum hs-CRP levels, may play a role in the induction of proteinuria11.
The study of Stehouwer CD et al in 2002 concluded that in type 2 diabetes, increased urinary albumin excretion, endothelial dysfunction, and chronic inflammation were interrelated processes that would develop in parallel & would progress with time12. Chronic inflammation as evidenced by high CRP was significantly associated with duration of diabetes mellitus according to Mojahedi et al13.
As proteinuria & CRP are the markers of systemic endothelial dysfunction & preclinical arterial inflammation as well13,14, they may have a role to develop other macrovascular complications including cardiovascular diseases15. We had also studied serum triglyceride level & serum LDL level in association with CRP. Serum triglyceride is associated with atherosclerosis16 & serum LDL is associated with coronary heart disease17. There were significant associations between CRP & serum triglycerides as well as between CRP and LDL in our study. Our findings were supported by Manoj Sigdel et al18. However Mojahedi et al13 found significant association of CRP with serum triglyceride only, not with LDL.
Few previous studies showed higher HbA1C was associated with higher CRP & they had significant association19. But we did not find any association between HbA1C & CRP possibly because of the presence of fairly controlled HbA1C in a tertiary hospital with proper follow up.
In some studies, they had found that there was a relationship between proteinuria and age20-23. We found similar result too. But there was also an association between CRP & age in our study. It might be the possibility that chronic inflammation, being a background process of diabetic nephropathy which in turn increased with advancement of the age, was leading to rise in CRP. It was very well understood that the levels of hs-CRP significantly associated with age and positively related to insulin resistance as concluded by Safiullah Amanullah et al24. Besides Aronson et al. reported that CRP levels among middle-aged people were higher in those with Diabetes mellitus when compared with the healthy subjects25.
We did not find any association of proteinuria or hs-CRP with body mass index similar to Mojahedi et al13. But it is opposing other studies26,27including Stehouwer CD et al12.
Serum creatinine in this study was also associated with proteinuria & CRP opposing the finding of Mojahedi et al13.
Conclusions
In our present study, we found that low grade inflammation as indicated by high CRP was an important predictor of diabetic nephropathy.
It was also found that advanced age in diabetics, dyslipidemia (higher triglycerides and LDL values), higher serum creatinine were also the major correlates with high CRP values.
Proteinuria is now widely accepted as an independent risk factor for cardiovascular morbidity and mortality28,29. Thus measurement of CRP in diabetic nephropathy can also estimate the cardiovascular risks.
As our study population was from a tertiary hospital with fairly controlled HbA1C, we found no significant difference in HbA1C levels across proteinuria levels.
Limitations of the study
Small study population
A tertiary hospital based study
Study period was short.
Mostly lower income group & those belong to rural areas were represented in government hospital, so this study was not the true representative to the society as a whole.
Few studies also demonstrated that antidiabetic drugs (Metformin/Pioglitazone) and statins might have effects to reduce inflammation30. We could not exclude the patients from our study whom were already on antidiabetic &/or Statin treatment.
This was a cross-sectional study. So we could not follow up the study population to assess the further consequences of inflammation and interventions.
Data Availability
WE HAVE INCLUDED ALL THE DATA FROM THE TEST REPORTS OF THE PATIENT. WE HAVE USED ANNOVA STATISTICAL SOFTWARE FOR STATISTICAL ANALYSIS. ALL THE DATA AND CALCULATIONS ARE CORRECT AND VALID. TESTS ARE DONE FROM VALID LABS.PATIENT CONSENT IS ALSO TAKEN.
FUNDING
No Funding is present for this research
Author
Dr. Kausik Mondal, MBBS, MD (Internal Medicine). Senior Resident (SR) in Jhargram Super specialty hospital, West Bengal, India.
Dattatreya Mukherjee, 5th year MBBS student and Researcher in Jinan University, P.R China.
Ethical Approval

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgement
We are thankful to the professors of Internal Medicine department and labs of Calcutta National Medical College, West Bengal University of Health Science, India. We are also thankful to the professors of Jinan University for supporting in the research work.
Bibilograph



