
Abstract
Study Objectives Sleep problems are common during chemotherapy for breast cancer (BC). We evaluated whether combined brief cognitive behavioral and bright light therapy (CBT+) is superior to treatment as usual with relaxation audio (TAU+) for insomnia symptoms and sleep efficiency (primary outcomes).
Methods We randomized women receiving intravenous chemotherapy, stratified by tumor stage and insomnia severity index (ISI), to 6-weeks CBT+ or TAU+. CBT+ included one in-person session, one telephone call, seven emails, and 20 minutes bright light each morning. TAU+ comprised usual treatment and two emails with relaxation audio tracks. Patient-reported outcomes were assessed at baseline, midpoint (week 3), post (week 6) and 3-month follow-up.
Results Women (N = 101) were randomly assigned to CBT+ or TAU+. Insomnia symptoms declined significantly more from baseline to post with CBT+ versus TAU+ (−5.06 vs -1.93, P = .009; effect size [ES] = .69). At 3-month follow-up, both groups had improved insomnia symptoms but did not differ (ES = .18, P = .56). CBT+ had higher patient-reported sleep efficiency than TAU+ after the start of intervention (P = .05) and more improvement in fatigue (ES = .59, P = .013) and daytime sleep-related impairment (ES = .61, P = .009) from baseline to post.
Conclusions CBT+ had a clinically significant impact on insomnia and fatigue with moderate effect sizes. Results support offering cognitive behavioral therapy for insomnia and bright light therapy during chemotherapy for breast cancer to help manage sleep and fatigue.
Clinical trial information Registered with the Australian New Zealand Clinical Trials Registry (http://anzctr.org.au/), Registration Number: ACTRN12618001255279
Statement of Significance Poor sleep is prevalent after cancer diagnosis, especially during chemotherapy. Although cognitive behavioral therapy for insomnia (CBT-I) has been shown to be effective, including in cancer survivors, chemotherapy is unique with significant, ongoing, exogenous factors disrupting sleep (e.g., pain, nausea, and steroids used to manage side effects from chemotherapy). We showed statistically and clinically significant improvements in insomnia and fatigue symptoms in the CBT-I plus bright light therapy (CBT+) treatment condition compared to the control in women receiving chemotherapy for stage 1–4 breast cancer. Waiting until cancer treatment completion may result in prolonging poor sleep and our findings suggest is not necessary. Future studies are needed to evaluate whether combined CBT+ is superior to CBT-I or light alone.
Introduction
Sleep disturbance affects up to 80% of women with breast cancer (BC)1-4 and a large, prospective study found 43% of people during chemotherapy met criteria for insomnia syndrome5. Three broad domains contribute to sleep disturbance in BC: (1) treatments (e.g., surgery, radiotherapy, chemotherapy, hormonal therapy) and their side effects6, (2) psychological challenges of diagnosis and treatment (e.g., stress, depression, and anxiety)2,7,8; and (3) circadian rhythm disruption9-12, with chemotherapy as a potential cause13,14. Although sleep complaints are reported throughout the BC trajectory1, the period surrounding chemotherapy is notable for the development and exacerbation of insomnia symptoms15. Untreated, sleep disturbance and insomnia symptoms are associated with physical and psychological consequences including: depression, anxiety, cognitive decline, impaired daily functioning, productivity and quality of life, and increased physical morbidity4,16-18. Despite the prevalence and consequences of poor sleep, there are few trials of sleep interventions during chemotherapy19-21.
To improve sleep in women with BC, multiple contributing domains need to be targeted. Cognitive Behavioral Therapy for Insomnia (CBT-I), the first-line treatment for insomnia22 including insomnia comorbid with cancer4, is a multi-component intervention that targets psychological and behavioral factors. CBT-I comprises sleep restriction, stimulus control, sleep hygiene, cognitive restructuring and can include relaxation training. CBT-I can be effective even when factors outside of an individual’s control (e.g., chemotherapy) interfere with sleep2. Further, there are benefits to a non-pharmacological approach, given the known consequences of pharmacological sleep-aid use23 and the potential for interactions between sleep-aids and chemotherapy drugs24. Limitations of CBT-I include delivery demands and limited accessibility25-27. A few trials have tested brief delivery formats of CBT-I in cancer (internet and video-based programs) showing efficacy25,28. However, CBT-I does not directly target circadian rhythm disruptions. Bright light (BL) therapy is a low-cost treatment for circadian rhythm disruption29-31. Three small studies showed that BL can prevent worsening fatigue and circadian rhythm deterioration during chemotherapy32-34; however, the impact of BL for sleep, during chemotherapy remains unclear.
To address these gaps, we developed a combined brief CBT-I and BL (CBT+) intervention that targets multiple mechanisms of poor sleep and conducted a randomized, controlled trial of CBT+ versus treatment as usual plus relaxation audios (TAU+) in women receiving chemotherapy for BC. Women with metastatic BC often have been excluded from previous sleep trials19,21 so that even less is known about the efficacy of sleep interventions in this high-risk group. We purposefully included metastatic BC to aid generalizability. The primary aim was to test the efficacy of CBT+ compared to TAU+ for the dual primary outcomes of patient reported insomnia symptoms and sleep efficiency (time asleep divided by time spent in bed for sleep). Secondary aims were to compare the effects of CBT+ versus TAU+ on sleep parameters from sleep diary and accelerometry and on patient reported outcomes (PROs) of fatigue, sleep-related impairment, sleep disturbance, and psychological symptoms. We hypothesized that women randomized to CBT+ (versus TAU+) would show greater improvements on the above outcomes.
Methods
Study Design
Detailed methods are in the published trial protocol35.Reporting follows CONSORT guidelines for social and psychological interventions and PROs. The Peter MacCallum Cancer Centre (PMCC) ethics committee (#17/159) approved the trial in accordance with the Declaration of Helsinki. This was a randomized, two-group, parallel, non-blinded, controlled, single-center, superiority trial, conducted at PMCC. After providing written informed consent and screening, eligible participants were randomized to CBT+ or TAU+ and commenced the 6-week intervention. PROs were assessed at baseline prior to the intervention, intervention mid-point (3 weeks), post-intervention (6 weeks) and 3-months post-intervention completion follow-up. Objective and self-report sleep parameters were measured continuously for the 6-week intervention period commencing the night after the first intervention session.
Study participants
Eligible women were diagnosed with any stage of BC; aged ≥18 years; receiving intravenous chemotherapy at study entry; English speaking; able to access emails; able and willing to wear BL glasses. Exclusion criteria were male; receiving only neoadjuvant chemotherapy; and diagnosed with a severe psychiatric or substance use disorder via the MINI36 interview. History of migraines and very advanced (early), delayed (late), or highly variable sleep timing, or non-24 sleep and wake pattern, based on the Duke structured sleep interview37, were exclusions.
Interventions
All intervention components were delivered by a provisional psychologist trained in CBT-I at Monash University Healthy Sleep Clinic. Sessions were recorded and reviewed by a senior CBT-I clinician.
CBT+ comprised one 60-minute face-to-face session at the PMCC Chemotherapy Day Unit; one 20-minute telephone call at study mid-point and seven, weekly CBT-I content emails. Light boxes and glasses produce comparable effects38. Participants wore Luminette® light glasses for 20 minutes (per manufacturer recommendation) each morning at the brightest setting (see Supplementary methods). Women reported the duration and timing of light in daily diaries. Reported light use ≥20min and within -1 to +4 hours of habitual rise time was considered adherent. CBT+ content included: general information and skills for better sleep (e.g., sleep hygiene, relaxation exercises, cognitive and behavioural strategies for dealing with night-time worries); fostering healthy attitudes and expectations about sleep following cancer diagnosis and during treatment; managing sleep challenges specific to cancer patients (e.g., physical discomfort, pain, daytime consequences of poor sleep); and identifying and managing symptoms of insomnia (e.g., stimulus control, bed restriction).
TAU+ was presented as an “audio relaxation group”. TAU+ comprised two emails with relaxation audio tracks developed by the Australian Cancer Council to assist in coping with cancer during the 6-week intervention period and a mid-point telephone call. Content included general relaxation strategies to be used at any time with no sleep-specific information. After the final follow-up, TAU+ participants received all CBT+ emails.
Primary Outcomes
Insomnia Symptoms
The first primary outcome was change from baseline through mid-point to post intervention on the Insomnia Severity Index (ISI)39, widely used and validated, comprising 7 patient-reported items (e.g., “difficulty falling asleep”), rated from 0 (none) to 4 (very severe), yielding a total score from 0-28. Scores of 0-7 indicate no clinical insomnia, 8-14 subthreshold insomnia, 15-21 clinical insomnia, and 22-28 severe clinical insomnia39.
Sleep Efficiency
Our second primary outcome was Sleep Efficiency (SEdiary), the ratio of self-reported total sleep time to total time spent in bed for sleep, from the consensus sleep diary40.
Secondary Outcomes
Sleep Parameters
Self-reported sleep diaries and the wrist-worn accelerometer (ActiGraph model wGT3X-BT) measured sleep onset latency (SOL), time spent awake after sleep onset (WASO) and total sleep time (TST), which has shown minimal average bias compared to polysomnography for TST, SE, and WASO in multiple studies41,42. Accelerometry data scoring followed a standard protocol, integrating estimates from an algorithm43, ambient light, and sleep diaries.
Random Assignment
REDCap (Research Electronic Data Capture) was used by a study member (BB) not involved in recruitment, to generate a 1:1 randomization scheme in advance, stratified by ISI scores (≤7, ≥8) and cancer stage (≤2, ≥3). Random seeds were generated, and variable block sizes used to assure concealment.
Statistical Analyses
Power analyses based on t-tests showed that 35 women completing each group would provide >80% power at α=.05 (two-sided) to detect a standardized mean difference of 0.70, a clinically meaningful difference.
Descriptive statistics are frequencies and percentages for discrete variables and means and standard deviations for continuous variables. Baseline group differences were tested using t-tests or chi-square tests to verify successful randomization. Due to non-normality, sleep efficiency was transformed as: and SOL and WASO were square root transformed, which normalized their distributions. SOL and WASO were winsorized at the 0.5% percentiles address outliers.
and SOL and WASO were square root transformed, which normalized their distributions. SOL and WASO were winsorized at the 0.5% percentiles address outliers.
Analyses followed a pre-specified plan35 and were intention-to-treat, conducted in R (v3.6) and MPlus (v8) with MplusAutomation47 on transformed variables. Tests were two-sided. Graphs are on the original scale. Analyses were piecewise latent growth models with an intercept and two linear slopes capturing (1) change from baseline through mid-point to post-treatment (primary hypothesis) and (2) maintenance from post-treatment to follow-up. Sleep diary and actigraphy analyses were mixed-effects models with a random intercept and linear slope of days since start of intervention. Analyses allowed freely estimated means, variances, and covariances of random intercepts and slopes and assumed a homogenous, independent residual variance. A constrained longitudinal analysis approach was taken48,49 and stratification factors were included as covariates50,51. Effect sizes (ES) between assigned groups were adjusted, standardized mean differences, standardized by the combined residual and intercept variance. Missing data were addressed using maximum likelihood52. Exploratory analyses examined results (1) in the subgroup with ISI≥8 at screening and (2) in sleep parameters by including weekday-weekend status and dexamethasone use as covariates.
Results
Patient Characteristics and Adherence
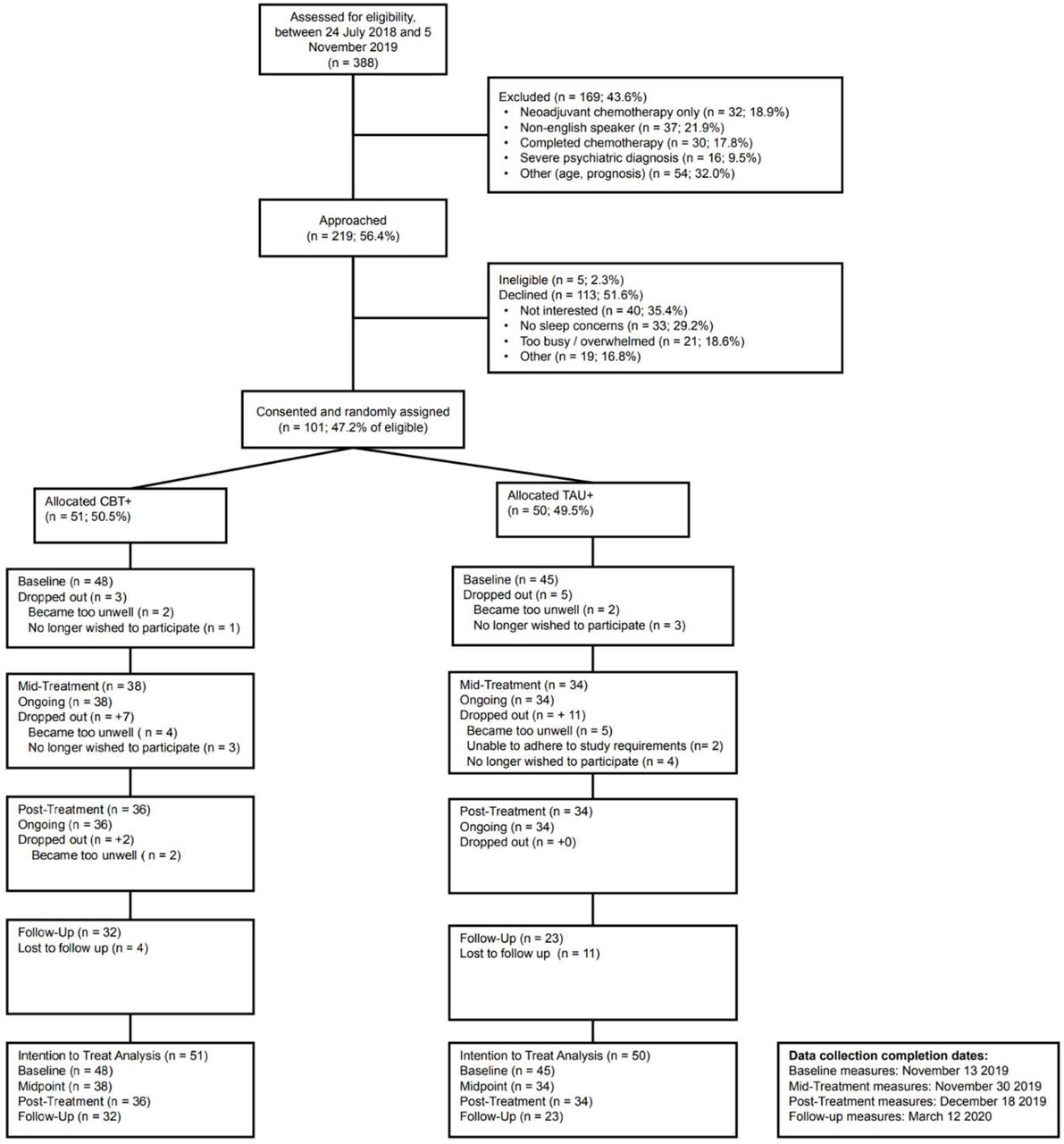
Between July 2018 and November 2019, 101 women receiving intravenous chemotherapy for breast cancer were randomized a median of 16 weeks post self-reported diagnosis (Figure 1). At randomization, 51.5% were stage ≤2 and 48.5% stage ≥3; 73.3% had subthreshold or more insomnia (ISI ≥8) and 26.7% had no clinical insomnia (ISI ≤7). There were no significant groups differences in sociodemographics, cancer treatments, or PROs at baseline (Table 1) nor in dropout across the study (Figure 1; additional results in Supplement). Self-reported credibility and expected benefit of the two interventions did not differ at baseline (see Supplement).

CONSORT diagram and recruitment flow chart.
Baseline Sample Characteristics by Group
CBT+ and TAU+ had comparable intervention email open rates (84% vs 87%). On average, self-reported intervention strategy use was 3-4 times per week in both groups. BL adherence was 4.18 mornings per week counting missed daily reports as non-adherence or 6.28 mornings per week excluding missed reports. There were no reported adverse events deemed to be a direct result of trial participation.
Primary Outcomes
All PROs had excellent reliability with Cronbach’s α ≥0.87 across all timepoints. Insomnia symptoms declined significantly in both groups from baseline to post-intervention; CBT+ declined -5.06 versus -1.93 in TAU+ (3.13 points more, P = .009; see Table 2). Figure 2 Panel A presents adjusted means, effect sizes, and group differences. To evaluate heterogeneity in treatment response, percent change from baseline to post-intervention in insomnia symptoms for each participant was calculated (Figure 3) showing that more women improved in CBT+ vs TAU+ (89% vs 68%), more women showed at least a 50% symptom reduction in CBT+ vs TAU+ (49% vs 15%), and fewer women had worsened insomnia symptoms in CBT+ vs TAU+ (9% vs 26%). From post-intervention to 3-month follow-up, there was no change in the CBT+ group, but the TAU+ group showed a further 2.52-point reduction (P = .023; Table 2). There were no group differences at 3-month follow-up (Figure 2 Panel A).
Changes by Treatment Group

Changes in mean patient reported outcome measures at baseline, mid-point, post-intervention and 3-month follow up by group. Insomnia Symptoms (Panel A) is the primary outcome, all others (B - F) are secondary outcomes. Values are adjusted means and 95% confidence intervals from the primary analyses. Dashed grey line indicates population average values, where available, or minimal symptoms (insomnia symptoms only). The number of non-missing scores available in each group at each assessment are at the bottom. Baseline was completed just prior to week 0 (intervention start), midpoint at week 3, post at week 6, and follow-up 3-months after the completion of the intervention. CBT+ = cognitive behavioral therapy + bright light therapy. TAU+ = treatment as usual + relaxation audios. ES = effect size; n.s. = not significant; * p < .05; ** p < .01

Individual participant change scores for insomnia symptoms from baseline (just prior to week 0, the intervention start) to post intervention (week 6) assessment points. CBT+ = cognitive behavioral therapy + bright light therapy. TAU+ = treatment as usual + relaxation audios. Arrows indicate the median change for CBT+ and TAU+.
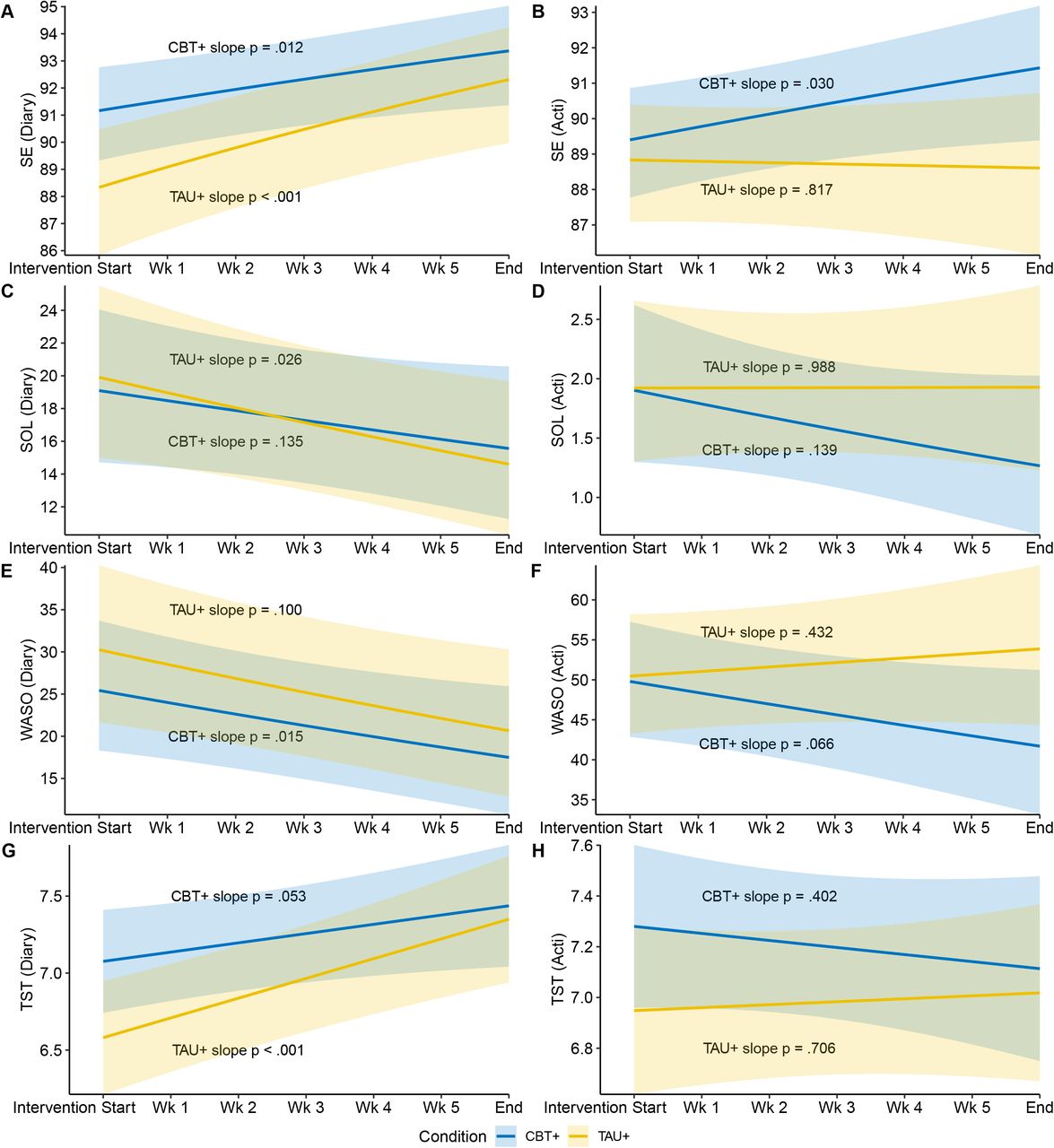
Our second primary outcome, SEdiary, was significantly higher in the CBT+ vs TAU+ group after the start of the intervention (P = .05; Online Table 3; Figure 4 Panel A). Both groups increased significantly over time (both P < .05) and this change did not differ between groups (P = .33). Although groups did not differ at the end of the intervention, both had average SEdiary > 85%, indicative of good sleep efficiency.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in subjective and objective sleep from start to end of intervention period by group. SEdiary (Panel A) was the primary outcome. All others (B – H) were secondary outcomes. Sleep diary and actigraphy assessments began the first night after the initial face-to-face intervention session. Graphs are estimated means over time with 95% confidence intervals shown in the shaded regions. Diary = sleep measures assessed by sleep diary. Acti = sleep measures assessed by wrist-worn actigraphy. SE = sleep efficiency, in percentages. WASO = wake after sleep onset, in minutes. SOL = sleep onset latency, in minutes. TST = total sleep time, in hours. CBT+ = cognitive behavioral therapy + bright light therapy. TAU+ = treatment as usual + relaxation audios.
Secondary Outcomes
Sleep and Psychosocial PRO
Changes over time and group differences for secondary PROs are in Table 2, with adjusted means, effect sizes and group differences in Figure 2 Panels B–F. When compared with TAU+, those assigned CBT+ improved 4.17 points more in fatigue, which was clinically meaningful and significant at 6-week post intervention time point (ES = .59, P = .013). Improvements in CBT+ over TAU+ also emerged for daytime sleep-related impairment (P = .009) with a trend for greater improvement in sleep disturbance (P = .085). Depression and anxiety symptoms did not differ between groups (both P > .30).
Sleep diary outcomes
SOLdiary and WASOdiary did not differ after the first intervention session and did not differ in how they changed over time (Online Table 3; Figure 4 Panels C & E). The trend was for both to decrease across the intervention. Compared to TAU+, the CBT+ group reported a trend towards 30min longer sleep duration (P = .051) after the start of the intervention and no differences in change over time (Online Table 3; Figure 4 Panel G).
Actigraphy outcomes
SEacti did not differ between groups after the first intervention session, but there was a trend for different change trajectories over time (P = .080) with SEacti increasing across the intervention for the CBT+ (P = .030) but not the TAU+ group (P = .817; see Online Table 3; Figure 4 Panel B). A similar pattern was observed for WASOacti, (Online Table 3 and Figure 4 Panel F). There were no differences after the first intervention session nor in the change over time for SOLacti nor TSTacti (Online Table 3; Figure 4 Panels D & H).
Exploratory Analyses
Exploratory analyses were conducted to examine whether treatment was more effective in subgroup of women with higher initial symptoms (n = 67 reported at least subthreshold insomnia with ISI ≥8 at screening). See detailed results in the Supplement (Online Tables 4 & 5; Online Figures 5 & 6). Improvements in insomnia symptoms remained significant and effect sizes were within ±.05 of results on overall sample, indicating minimal differences in benefits. Results for SEdiary also were comparable although in this subgroup, differences after the first intervention session were not significant. Improvements in fatigue in CBT+ vs TAU+ at post-intervention were larger (ES = .76, P = .005). Results for secondary outcomes were comparable.
Additional exploratory analyses on the sleep diary and actigraphy outcomes included two other sleep impacting factors as covariates: (1) weekend versus weekday sleep patterns, and (2) use of dexamethasone as part of chemotherapy regimen. Results were comparable to the overall sample with larger differences between CBT+ and TAU+ on SEdiary (P = .009) and TSTdiary (P = .010) after the first intervention session in favor of CBT+. Rates of mental health and sleep treatment, including medication, receipt during the intervention did not differ between groups, nor were associated with change in insomnia symptoms. Detailed results are in the Supplement (Online Tables 6 & 7; Online Figure 7).
Discussion
In women receiving chemotherapy for BC, this randomized trial examined the effects of CBT+ versus TAU+ on insomnia symptoms and sleep efficiency, as well as secondary outcomes of fatigue, other sleep parameters, and psychological symptoms. Women receiving CBT+ showed significantly greater improvements in the primary outcomes of insomnia symptoms and sleep efficiency, and secondary outcomes of sleep-related impairment and fatigue, supporting its efficacy as a sleep treatment in this population. Intervention effects on insomnia, fatigue and sleep-related impairment were clinically significant by 6 weeks (post-intervention), with women in the CBT+ group having mild insomnia symptoms that no longer differed from the population average, and fatigue symptoms improving beyond the 3-4 points considered a meaningful change, while the TAU+ group had no meaningful change in fatigue. At an individual level, all but three women in CBT+ experienced a decline in insomnia symptoms suggesting that CBT+ works, or at least does no harm, for nearly all women.
Exploratory analyses revealed that CBT+ is effective for women receiving chemotherapy for BC regardless of initial symptoms. Smaller improvements were observed in the TAU+ group for insomnia symptoms, sleep disturbance, and sleep efficiency, suggesting that TAU+ may provide some benefit, although we cannot distinguish effects of TAU+ versus natural declines in sleep problems over time.
Three months after ceasing intervention (including BL), CBT+ treatment benefits were maintained. Although outcomes were not significantly different between groups at follow-up, improvements in insomnia, sleep-related impairment, and fatigue via CBT+ over the 6-week intervention period may result in better functioning and quality of life during chemotherapy, a period when many other symptoms are distressing and difficult to alter.
Despite need and calls for greater recognition of sleep in cancer53, few trials target insomnia symptoms during chemotherapy. To our knowledge, no trial to date has combined brief CBT-I with BL to target the multiple causes of poor sleep during chemotherapy. A recent trial examined the effects of 21 days of bright light therapy only in this population and showed some benefit for sleep, depression and quality of life, however improvements in subjective sleep quality and fatigue were not statistically significant54. Comparatively, outcomes of the present trial may be indicative of the benefit in combining CBT-I and light therapy, or a longer intervention duration. In addition, approximately one quarter of participants in the CBT+ trial had metastatic BC, a group traditionally underrepresented in cancer sleep trials. Our outcomes and adherence data suggest that insomnia symptoms and fatigue can be treated during chemotherapy with a non-pharmacologic approach, despite the substantial physical and psychological impacts of active cancer treatment. CBT+ delivered using a combination of face-to-face (readily adaptable to telehealth delivery), telephone, and self-help materials is less burdensome on clinicians (about 1.5 hours) and patients than standard CBT-I (typically 6–10 hours). BL can be used at home with brief instruction and equipment mailed if needed, making CBT+ deliverable in cancer treatment clinics or at home in a scalable manner.
Strengths of this study include an intervention empirically grounded in the multiple determinants of insomnia symptoms and poor sleep during chemotherapy, random assignment, a manualized intervention, defined eligibility criterion, 6-weeks of subjective and objective sleep assessment, and equal representation of all stages of BC. This study also had limitations. To minimize burden, accelerometry and sleep diaries collection started after the first intervention session, so a true baseline was not available for these measures. Although accelerometry corresponds well with polysomnography for sleep duration, it tends to miss wake after sleep and likely underestimated sleep onset latency. Most participants were white, well-educated and had relatively high household income. Interventions were conducted by one interventionist at a single center. Future trials are needed with greater representation of race and ethnic groups and level of socioeconomic status and across multiple centers and interventionists to evaluate generalizability. About half of eligible women declined, primarily due to not being interested, no sleep concerns, or being overwhelmed. There was dropout after baseline, primarily from women reporting being too unwell, which may bias results. Targeting women with baseline symptoms or emphasizing the potential benefits of the trial may increase uptake. Although the trial was powered for its primary outcomes, larger trials would allow evaluating treatment efficacy in subgroups (e.g., chemotherapy cycle, cancer stage). Future trials are needed to evaluate whether CBT+ works in other cancer types and males. This first trial of CBT+ aimed to evaluate its efficacy, but future trials could investigate brief CBT-I and BL separately and together to identify any independent and synergistic effects.
In conclusion, this trial provides evidence that brief CBT+ can treat insomnia symptoms, sleep-related impairment, and fatigue for women with BC during chemotherapy. Chemotherapy can cause acute sleep disruption and fatigue adding to burden during a challenging time, so early intervention is crucial4,19.Our results support the feasibility and efficacy of intervening during chemotherapy and is one of the first to combine CBT-I and light therapy. Further research needs to consolidate findings, yet these results are an important step toward incorporating accessible, effective treatment for sleep into routine cancer care. Routine delivery of CBT+ may reduce the number of people with BC suffering from insomnia symptoms, fatigue, and associated impairment during and after chemotherapy.
Data Availability
Data will be shared upon reasonable request to the corresponding author.
FUNDING
This study is supported by seed funding from Monash University with light glasses provided by Lucimed SA, Belgium. Wiley (1178487) and Bei (1140299) were supported by NHMRC fellowships.
NOTES
All authors declare no conflict of interest. The funders had no role in the study design, data collection, analysis, interpretation, or presentation of results.
Data will be shared upon reasonable request to the corresponding author.
Footnotes
Email: helena.bean{at}monash.edu
Email: justine.diggens{at}petermac.org
Email: maria.ftanou{at}petermac.org
Email: marliese.alexander{at}petermac.org
Email: lesley.stafford{at}thewomens.org.au
Email: bei.bei{at}monash.edu
Email: prue.francis{at}petermac.org
Email: joshua.wiley{at}monash.edu
References



