
Abstract
The role of modelling in predicting the spread of an epidemic is important for health planning and policies. This study aimed to apply a dynamic Susceptible-Exposed-Infected-Recovered-Deaths (SEIRD) model and simulated it under a range of epidemic conditions using python programme language. The predictions were based on different scenarios from without any preventive measures to several different preventive measures under R0 of 4. The model shows that more weight to personal protection can halt the spread of transmission followed by the closure of public places and interprovincial movement restriction. Results after simulating various scenarios indicate that disregarding personal protective measures can have devastating effects on the Sri Lankan population. The importance of strict adherence, maintain and monitoring of self-preventive measures lead to minimizing the death toll from COVID-19.
What we already know
Compartmental models can be used to project scenarios with various disease control measures individually or as a useful combination for evidence-based policy formulation.
Epidemiologists have been using mass action, compartmental models, over a hundred years which are famous for simplicity in both analysis and outcome assessment.
Mathematical modelling plays a vital role in the highest level of policymaking in the fields of health economics, emergency planning, monitoring of surveillance data and, risk assessment and control.
What this article adds
This paper aimed to describe a dynamic Susceptible-Exposed-Infected-Recovered-Deaths (SEIRD) model and simulate it under a range of epidemiological conditions to give an insight into COVID-19 spread in Sri Lanka.
The SEIRD model produces a time frame for preparedness and resource allocation of a country without exceeding the surge capacity which may lead to a disastrous situation which allows authorities to plan potential mortuary capacity and understand the burden on crematoria and burial services.
New policy discussions need to occur whenever the best available options such as different preventive strategies and knowledge about the epidemiology changes.
The proposed model can serve as a tool for health authorities for planning and policymaking to control the pandemic by implementing appropriate policy decisions on time to prevent a disastrous situation.
1. Introduction
The coronavirus disease has become a pandemic that poses a serious public health risk globally. The virus is mutating rapidly and producing many strains which is a significant threat to the control measures. The alpha strain is a more transmissible variant initially detected in the United Kingdom, currently circulating in Sri Lanka as the main variant 1. However, the delta variant which has higher transmissibility is currently being detected in several places from June to August 2021. In this context, an in-depth understanding of the current epidemic and demand dynamics is fundamental in health planning and policymaking, especially when the resources are limited. With the purpose of forecasting, different prediction models are proposed by various academics and groups 2,3. Compartmental models can be used to project scenarios with various disease control measures individually or as a useful combination for evidence-based policy formulation. Furthermore, epidemiologists have been using mass action, compartmental models, over a hundred years which are famous for simplicity in both analysis and outcome assessment4. One scientific way of predicting the future directions and trends of an epidemic is the development of different compartment models 5. The key element in this field of research is being able to link mathematical models and data. Both epidemiological data and findings of mathematical model studies can be compared for optimal results and guidance. Mathematical modelling plays a vital role in the highest level of policymaking in the fields of health economics, emergency planning, monitoring of surveillance data and, risk assessment and control. This paper aims to describe a dynamic Susceptible-Exposed-Infected-Recovered-Deaths (SEIRD) model and simulate it under a range of epidemiological conditions to give an insight into COVID-19 spread in Sri Lanka.
2. Methods
Many compartmental models belong to the basic Susceptible-Infectious-Recovered (SIR) class 4,6,7. The SIR models are further extended by adding an Exposed (E) compartment. We constructed a compartmental epidemiological model in the Figure 1 with vital dynamics describing the number of individuals in a fixed population who are susceptible to infection (S), exposed (E), infected (I), recovered (R), and deaths (D) compartments4,5.


{kind=link}
{kind=link}
X axis: Population= e107
We extracted publicly available data with permission from the official website of the Health Promotion Bureau (HPB) and the Epidemiology Unit, Ministry of Health, Sri Lanka 8,9. We used anonymized data for this analysis and extracted data relevant to cases reported from the 11th of March 2020 to the 5th of July 2021. For the development of the prediction model, three dynamic variables were considered. The first variable was personal measures (the practice of social distancing, wearing masks and handwashing) which was considered by the way they were adopted (100%, 50% and 25%). The second variable was inter-provincial movement restrictions with 100%, 75% and 50% adaptation. The third variable was the closure of places (public place, school, workplace) with 100%, 50% and 33% adaptation. The weighted factors for the three scenarios were 0.70, 0.33, 0.10 for personal measures, 0.15, 0.33, 0.60 for the movement restrictions, and 0.15, 0.33 and 0.30 for the closure of places, respectively. The predictions for SEIRD were made when the R0 value is 4. Python programming language was used for the analysis.
2.1 Model equations
The flow of individuals through the compartments of the model is governed by a set of Ordinary Differential Equations (ODE) as given below.

3. Results
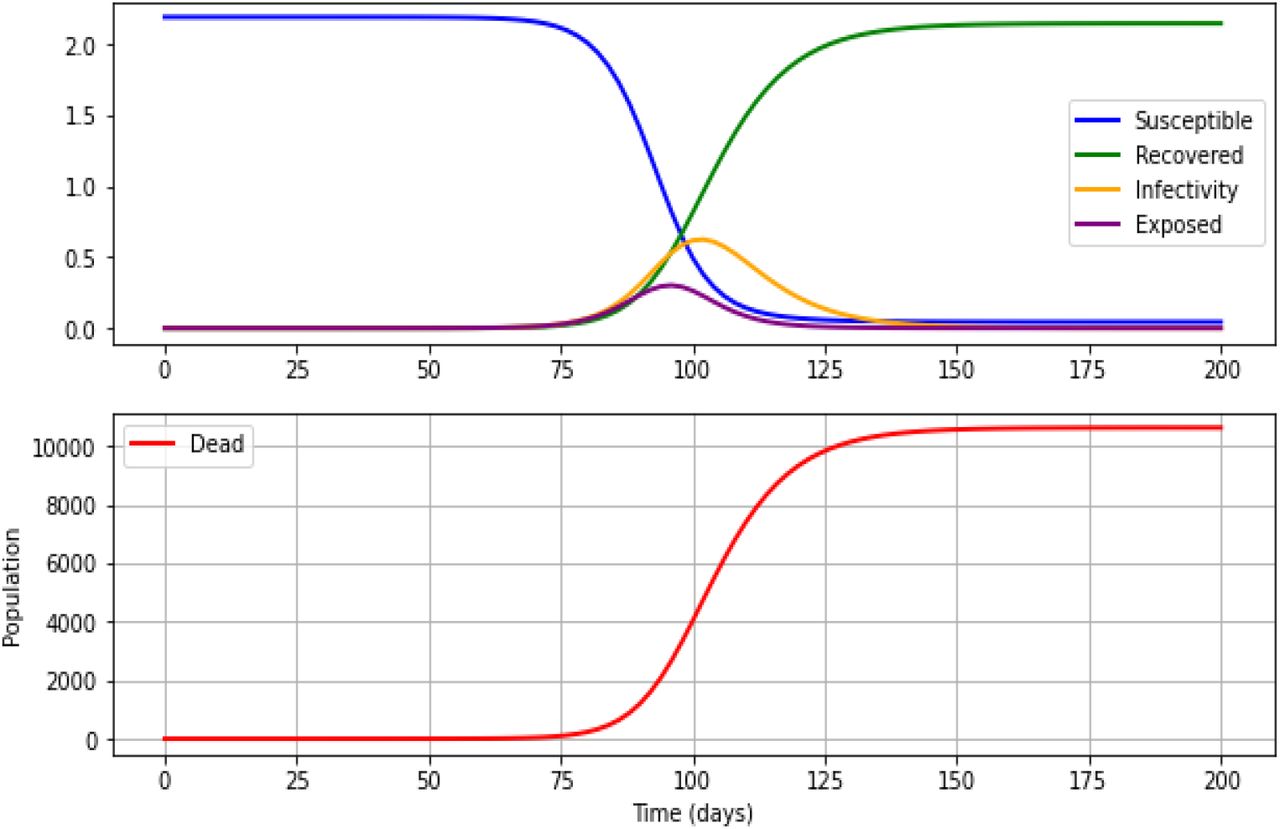
The figures below show the predictions of various preventive strategies which were based on R0 of 4. The X-axis shows the time (in days), and the Y-axis shows the population. The number of susceptible individuals is shown in blue, recovered in green, infective in yellow, exposed in purple and deaths in red.
3.1 Predictions based on the SEIRD model without any preventive strategies
If the R0=4, the peak of the infectious will occurs around day 100 with 6.3 million infected individuals. Out of all exposed and infected individuals, 10,617 will die following 150 days after the beginning of the epidemic curve if there are no proper strategies to prevent the outbreak.
3.2 Scenario One
3.2.1 Predictions of SEIRD with 70% of personal protection (social distancing, wearing masks and handwashing), 15% of movement restrictions and 15% of closure places (public place, school, workplace) with R0 of 4 with different strategies
We observed how the SEIRD dynamics are affected by different preventive strategies for COVID-19 at a specific time in the system’s evolution.
3.2.1.1 With the implementation of 100%, 50% and 25% of personal protection
With 100%, 50% and 25% of personal protection are implemented at R0 of 4, the rate of deaths will be increased from 600 days, 125 days, 85 days, with 3,409 deaths in 1200 days (with 0.24 million infected individuals), 9,803 deaths in 250 days (with 3.9 million infected individuals) and 10,373 deaths in 175 days (with 5.2 million infected individuals) will be observed, respectively. There is no visible peak observed with 100% personal protection. However, the number of days to achieve the peak of the infection curve will be 160 days with 3 million and 125 days with 4 million infected individuals at the peak of the infection curves with 50% and 25% personal protection, respectively.
[Refer Supplementary Figure 1 and Supplementary table 1]
3.2.1.2 With implementation of 100%, 75% and 50% of movement restrictions
With 100%, 75% and 50% of movement restrictions, the rate of deaths will be increased from 85 days, 80 days, and 75 days with 10,417 deaths in 175 days (with 5.4 million infected individuals), 10,481 deaths in 160 days (with 5.6 million infected individuals) and 10,535 deaths in 150 days (with 5.8 million infected individuals) will be observed, respectively. Moreover, the number of days to achieve the peak of the infection curve will be 120 days, 115 days, and 110 days, respectively.
[Refer Supplementary Figure 1 and Supplementary table 1]
3.2.1.3 With the implementation of 100%, 50% and 33% of closure of places
With the 100%, 50% and 33% of closure of places are implemented at R0 of 4, the rate of deaths will be increased from 85 days, 80 days, and 75 days with 10,417 deaths in 175 days with 5.4 million infected individuals, 10,535 deaths in 150 days with 5.8 million infected individuals and 10,566 deaths in 145 days with 5.98 million infected individuals will be observed, respectively. Furthermore, the number of days to achieve the peak of the infection curve will be 120 days, 110 days, and 105 days with the infected individuals of approximately 4 million, 5 million and 6 million at the peak of the infection curves. [Refer to Supplementary Figure 1 and Supplementary table 1]
[Refer to Supplementary Figure 1 and Supplementary table 1]
3.3 Scenario Two
3.3.1 Predictions of SEIRD with personal protection (social distancing, mask, hand washing), movement restrictions and closure (public place, school, workplace) with R0 of 4 with equal weight (33%) for all three dynamic variables
3.3.1.1 With the implementation of 100%, 50% and 25% of personal protection
With 100%, 50% and 25% of personal protection are implemented at R0 of 4, the rate of deaths will be increased from 120 days, 85 days, and 75 days and 9,897 deaths in 200 days (with 4.1 million infected individuals), 10,387 deaths in 175 days (with 5.3 million infected individuals) and 10,525 deaths in 150 days (with 5.8 million infected individuals) will be observed. Furthermore, the number of days to achieve the peak of the infection curve will be 150 days, 120 days, and 110 days with 4 million, 3.5 million and 5.8 million infected individuals at the peak of the infection curves respectively.
[Refer Supplementary Figure 2 and Supplementary table 1]
3.3.1.2 With implementation of 100%, 75% and 50% of movement restrictions
With 100%, 75% and 50% of movement restrictions are implemented at R0 of 4, the rate of deaths will be increased from 115 days, 100 days, and 85 days with 9,663 deaths in 200 days (with 4.1 million infected individuals), 10,165 deaths in 200 days (with 4.7 million infected individuals) and 10,387 deaths in 175 days (with 5.3 million infected individuals) will be observed, respectively. Moreover, the number of days to achieve the peak of the infection curve will be 120 days, 115 days, and 110 days with an infected individuals of approximately 4 million, 4.5 million and 5 million at the peak of the infection curves, respectively.
[Refer Supplementary Figure 2 and Supplementary table 1]
3.3.1.3 With the implementation of 100%, 50% and 33% of Closure of Places
With the 100%, 50% and 33% of closure of places are implemented at R0 of 4, the rate of deaths will be increased from 120 days, 90 days, and 80 days with 9,663 deaths in 200 days (with 4.1 million infected individuals), 10,387 deaths in 175 days (with 5.3 million infected individuals) and 10,487 deaths in 150 days (with 5.7 million infected individuals) will be observed. Furthermore, the number of days to achieve the peak of the infection curve will be 160 days, 120 days, and 115 days with an infected individuals of 2.5 million, 5 million and 5.5 million at the peak of the infection curves, respectively.
[Refer Supplementary Figure 2 and Supplementary table 1]
3.4 Scenario Three
3.4.1 Predictions of SEIRD with 10% of personal protection (social distancing, mask, hand washing), 60% of movement restrictions and 30% of closure of places (public place, school, workplace) with R0 of 4
3.4.1.1 With the implementation of 100%, 50% and 25% of personal protection
With the 100%, 50% and 25% of personal protection are implemented at R0 of 4, the rate of deaths will be increased from 85 days, 80 days, and 75 days, with 10,500 deaths in 150 days (with 6.3 million infected individuals), 10,565 deaths in 150 days (with 5.7 million infected individuals) and 10,592 deaths in 150 days (with 6.1 million infected individuals) will be observed, respectively. Furthermore, the number of days to achieve the peak of the infection curve will be 115 days, 110 days, and 105 days with 5 million, 6 million and 6.5 million infected individuals at the peak of the infection curves, respectively. [Refer Supplementary Figure 3 and Supplementary table 1]
3.4.1.2 With implementation of 100%, 75% and 50% of movement restrictions
With the 100%, 75% and 50% of movement restrictions are implemented at R0 of 4, the rate of deaths will be increased from 250 days, 150 days, and 110 days with 6,950 deaths in 500 days (with 1.3 million infected individuals), 9,142 deaths in 250 days (with 2.96 million infected individuals) and 9,912 deaths in 200 days (with 4.3 million infected individuals) will be observed. Moreover, the number of days to achieve the peak of the infection curve will be 350 days, 200 days, and 150 days with infected individuals of 0.5 million, 2.5 million and 4 million at the peak of the infection curves, respectively. [Refer Supplementary Figure 3 and Supplementary table 1]
3.3.1.3 With the implementation of 100%, 50% and 33% of closure of places
With the 100%, 50% and 33% of closure of places are implemented at R0 of 4, the rate of deaths will be increased from 110 days, 90 days, and 80 days with 9,912 deaths in 200 days (with 4.3 million infected individuals), 10,417 deaths in 150 days (with 5.4 million infected individuals) and 10,502 deaths in 150 days (with 5.7 million infected individuals) will be observed, respectively. Furthermore, the number of days to achieve the peak of the infection curve will be 150 days, 120 days, and 110 days with an infected individuals of 4 million, 5 million and 6 million at the peak of the infection curves, respectively. [Refer Supplementary Figure 3 and Supplementary table 1]
4. Discussion
As the COVID-19 pandemic progresses, countries are increasingly implementing a broad range of response activities 16. The present study revealed that it will be necessary to layer multiple interventions, regardless of whether suppression or mitigation is the overarching policy goal. The choice of interventions ultimately depends on the relative feasibility of the implementation of the different strategies and their effectiveness.
The compartment models were invented during the late 1920s, which are the most used models in epidemiology. Moreover, different approaches using agent-based simulations are still based on compartment models17. The SEIR model is very frequently used to explain the COVID-19 pandemic, which is basic and a reasonably good fit for the disease5. Results of our paper after simulating various scenarios indicate that disregarding social distancing and hygiene measures can have devastating effects on the Sri Lankan population. However, that model also shows that quarantine of contacts and isolation of cases can help halt the spread of novel coronavirus 18. The accuracy of the predictions of the epidemiological models depends critically on the quality of the data feed into the model. If the data quality is good, the model can precisely describe the situations. A fitting example would be when accurately estimating the case fatality rate, which requires all cases of the disease and the number of dead 4. However, during the COVID-19 pandemic, the number of deaths has often been highly inaccurate for many reasons, and the number of infected has also been incorrect. There can be undiagnosed cases during that period because of limited testing, which lead to inaccurate reporting 4,19. Furthermore, one of the significant limitations of the model is that it does not include the natural death and birth rates assuming those are constant 4,20. In addition, during the COVID-19 pandemic, there are broad variations in estimations of Case Fatality Rate (CFR) that may be misleading. Countries may be more or less likely to detect and report all COVID-19 deaths. Furthermore, they may be using different case definitions and testing strategies or counting cases differently. Variations in CFR also may be explained in part by the way time lags are handled. Differing quality of care or interventions being introduced at different stages of the illness also may play a role. Finally, the profile of patients may vary between countries 15.
The proposed model uses the predictors as given in the parameter table under the methodology section. The model was internally validated using the parameters available in the previous studies in the underpinning literature. As with any modelling approach, our findings relate to the assumptions and inputs of the model which lead to a major limitation. The assumptions with the greatest potential effect on our findings are the structural assumptions of a compartmental epidemiological model4. Furthermore, the predictive capability of the tool is highly dependent on several preliminary data for parameter estimation. This dependence may lead to data misinterpretation, especially considering the SIR model. Notably, an essential parameter in epidemic modelling is the ‘basic reproduction ratio (R0)’. The size of the R0 can be varied since it is determined by averaging many cases. Moreover, R0 depends on the contagiousness of the pathogen and the number of contacts of an infected person18. Furthermore, a study has found an R0 of 2.53, implying that the pandemic will persist in the human population in the absence of strong control measures5. The parameters, which are locally informed, form the basis of predicting and forecasting exercises accounting for different scenarios and impacts of COVID-19 transmission.
The internal, and external validation of the model is vital for the robust prediction of the ODEs in the model. Thus, the models were applied in the series of equations to get the equilibrium in the SEIRD model. Thereafter, the simulation of the validated model was performed to obtain the policy scenarios of the proposed model. Initially, the model comprised of one exposed individual, and the rest of the population was considered as a susceptible population21–23. Therefore, the predictors were handled with care in the model to avoid overestimation or underestimation. In addition, the infection fatality ratio (IFR) of COVID-19 acts as a simple factor in the mortality effects of preventive strategies and does not alter the presented relative conclusions. There are limited serological studies to calculate IFR accurately during outbreaks. In such situations, estimates need to be made with routinely available surveillance data, which generally consist of time series of cases and deaths reported in aggregate15. When the available data was considered, the situation was almost like a similar study done in China14. The high mortality rate in the COVID-19 pandemic requires that our model have a designated compartment for deaths. The fatality compartment is the only compartment of the model with no further interaction with the rest of the epidemic system. Beta, the proportion between the rate of infection and the rate of spread (R0) was predicted when R0 equals 4. It is found that the peak of deaths in Sri Lanka may arrive after five months (150 days) following exposure with a maximum number of deaths around 10,617 if there are no preventive measures during the current wave. With high weight to the personal protective measures, the occurrence of deaths will be reduced by 68% and 71% reduction of the infected cases than without having any measures. With high weight to movement restrictions, 35.7% of deaths and 83% of the infected population will be reduced without having any measures. If we give equal consideration for personal protection, movement restriction and closure, only 10.6% of deaths and 36.5% infected population will be prevented without having any measures.
5. Conclusion and Recommendation
In the present work, a computational model for predicting the spread of COVID-19 by the dynamic SIERD model has been proposed. The dynamic model assumes a time-dependent death fraction. Various epidemiological parameters such as time of peak arrival, number of active cases and number of deaths during peak are evaluated for all cases and predictions were made against different preventive measures. The key conclusion that we emphasized from this study is the importance of strict adherence, maintenance, and monitoring of the self-preventive measures properly to minimize the death toll from COVID-19. Policymakers need to streamline the resources that are essential for the smooth functioning of this strategy. Polices can be guided by these results which need to be implemented to lower the total population infected, and deaths which will lead to flattening of the curves.
Data Availability
Publicly available data was taken from the dash board of HPB, Ministry of Health
Ethics Approval
The research design and methodology used only anonymized data sets. This entails that no ethical approval is required.
Author Contributions
Conceptualization and methodology; MSDW, NUR, SPJ, PCW, IG; Software; SPJ; Formal analysis; SPJ and NUR; Original draft preparation; NUR; Writing; NUR, PCW, IG; Review, editing and supervision; MSDW and NUR. All authors have read and agreed to the manuscript.
Declaration of Competing interest
There is no conflict of interest.
Funding
We did not receive any funding from funding agencies for this study.
Acknowledgement
We would like to acknowledge Health Promotion Bureau (HPB), Ministry of Health Sri Lanka.
Footnotes
Postal Address (Permanent): No-157, Jayanthipura, Kurunegala, Sri Lanka (Postal code: 600000)
References



