
Abstract
In heart failure (HF), increased physical activity is associated with improved quality of life, reduced hospitalisation, and increased longevity and is an important aim of treatment. However, physical activity levels in individuals living with HF are typically extremely low. This qualitative study with one-to-one interviews systematically explores perceived clinical, environmental, and psychosocial barriers and enablers in older adults (>70 years old) living with HF. Semi-structured interviews (N = 16) based on the Theoretical Domains Framework elicited 78 belief statements describing the barriers and enablers to physical activity. Theoretical domains containing these beliefs and corresponding constructs that were both pervasive and common were deemed most relevant. These were: concerns about physical activity (Beliefs about Consequences), self-efficacy (Beliefs about Capabilities), social support (Social Influences), major health event (Environmental Context and Resources), goal behavioural (Goal), action planning (Behavioural Regulation). This work extends the limited research on the modifiable barriers and enablers for physical activity participation by individuals living with HF. The research findings provide insights for cardiologists, HF-specialist nurses, and physiotherapists to help co-design and deliver a physical activity intervention more likely to be effective for individuals living with HF.
Introduction
Heart failure (HF) is a syndrome triggered by underlying cardiac dysfunction that affects the efficiency with which the heart pumps blood around the body. It is characterised by signs of volume overload, which may include peripheral oedema and pulmonary rales, and involves symptoms of breathlessness, effort intolerance and fatigue. It is a global health problem, affecting an estimated 64 million individuals: around 1% to 2% of the general adult population (1). Despite medical advances, HF is a substantial cause of morbidity and mortality (2); 5 and 10-year survival have been identified by recent meta-analysis as 57% and 35%, respectively (3).
Physical activity is recommended for individuals living with HF (4). However, levels of engagement are considerably lower among individuals with HF than in the general population (5). Promoting physical activity is particularly challenging in the context of HF, owing to the complexity underlying the behaviour (6) and the many challenges individuals living with HF may face (7).
While the beliefs about symptoms and the course of the disease held by individuals living with HF have been previously described (8), less is known about how to promote recommended lifestyle changes, including increased physical activity. There is emerging evidence that physical activity interventions addressing behaviour change (9) and interventions based on a behaviour change theory (10) are potentially promising for promoting physical activity in HF. An explicit understanding of how behaviour is enacted is recommended by the Medical Research Council Guidelines for the development of complex interventions because this can enable understanding of the mechanisms that underpin change and so guide the choice of theory, thus informing the development and delivery of future interventions (6,11,12).
Engagement in physical activity among individuals with HF is complex and is subject to many clinical and psychosocial factors specific to this population. A systematic review of the barriers and enablers of physical activity among this patient group (13) indicated that a complex relationship between physical health status and support and encouragement from professionals and social sources are relevant and merit further investigation.
Currently, existing interventions have a limited and variable impact on increasing physical activity in older adults living with HF (9). Only one intervention – REACH-HF(14) – was developed adhering to the Medical Research Council guidelines (6) and evaluated a theory-based intervention targeting self-care behaviours, including physical activity engagement (14). The REACH-HF intervention achieved clinically meaningful change in the quality of life and is estimated to be cost-effective in increasing the number of quality-adjusted life years, QALY (15). However, the efficacy of the REACH-HF intervention in increasing physical activity in HF was not supported (16). The REACH-HF intervention was developed using the Intervention Mapping Framework (17). This study, which also follows the MRC guidelines, adopts alternative methods used in research informing intervention development Theoretical Domains Framework (18). The use of TDF offers the following advantages over the IMF. The TDF offers means to systematise and structure the research enquiry (18). Additionally, in contrast to REACH-HF, the present study focuses on physical activity alone. A meta-analysis of behaviour change interventions suggests that simultaneously addressing several behaviours is not beneficial in achieving a positive change in the target behaviour (19).
This study expands the understanding of the barriers and enablers to physical activity in older adults (>70 years old) living with HF. The present qualitative study with one-to-one interviews systematically explores perceived clinical, environmental, and psychosocial barriers and enablers in older adults living with HF.
Methods
We followed the Standards for reporting qualitative research in conducting and describing this study (20).
Design
One-to-one interviews guided by a TDF-based interview schedule were carried out.
Setting and recruitment
Participants were recruited from outpatient cardiology clinics at the Royal Brompton & Harefield NHS Foundation Trust, UK. Individuals with HF who meet the inclusion criteria were identified by a member of the clinical team and asked if they were interested in the study. Those who expressed an interest were introduced to the researcher (AA). Each participant was provided with a participant information sheet (PIS) and an informed consent form (ICF). The researcher described the study aims, objectives, and procedure in more detail and answered participants’ questions about the study. Individuals who expressed an interest in participating in the study were given an option to consider their participation over 24 hours. Those who decided to take part were asked to sign the ICF.
Inclusion and exclusion criteria
Older adults (≥70 years old) diagnosed with HF according to the diagnosis criteria outlined by the contemporaneous European Society of Cardiology guidelines (21) were recruited to take part in this study. Only clinically stable HF patients were recruited (i.e., someone who has not experienced a change in their condition’s severity, NYHA class, or medical regimen in the past three months). The clinical assessment of the stable condition was carried out by a health professional at the recruitment site. To take part in the study, participants were required to be able to provide informed consent and to converse in English. Individuals with uncontrolled angina or symptoms even at rest (New York Heart Association class IV) and those who were recommended to avoid exercise or any moderate or strenuous physical activity by a healthcare professional were not invited to take part in the study.
Sampling strategy
The criterion sampling strategy has been designed to reflect the diversity and breadth of this population within pragmatic limits (i.e., ethnicity, sex, and NYHA class).
Ethical issues pertaining to human subjects
The design and the conduct of this research were approved by the Health Research Authority. The ethical approval was received from the East of England – Cambridge Central Research Ethics Committee (REC reference: 17/EE/0183).
Data collection methods
Age, sex, level of education, ethnicity, marital and occupational status were recorded using self-reports. Information on the duration of HF diagnosis, comorbidities, NYHA class, left ventricular ejection fraction (LVEF) (%) at the most recent clinical assessment, medication, and the frequency of hospitalisation in the past year was extracted from clinical records. Comorbidities were additionally assessed using a standard self-report checklist (22). The medical records data extracts were matched to the participant identification number and entered into an Excel file.
Procedure
After providing informed consent, participants took part in a single one-to-one interview. The researcher arranged for the interview to be conducted at a convenient time and place suited to the participant. Participants were offered an option to be interviewed at City, University of London premises, in a suitable room at the clinic (e.g., vacant consultancy room), research rooms available at the clinic, at the participant’s home, or via telephone. All participants opted for the research room or clinic room at the hospital or for a telephone interview.
Data collection instruments and technologies
A flexible interview schedule was developed. The schedule was designed to elicit the description of everyday physical activity. It then explored how physical activity has changed since the time of HF diagnosis to assist the participant in expressing beliefs that are relevant to HF. The schedule was then followed with a TDF-informed interview schedule. The feedback on the content and structure of the interview schedule was received from six health services researchers with expertise in TDF-informed research and/or health research management, a cardiologist, a HF-specialist nurse, and two individuals diagnosed with HF, who are members of the Patient-Participant Committee at the Public Involvement in Research Forum of the Cardiovascular Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust. The interview schedule was amended following this feedback. One individual with HF participated in a pilot interview and provided feedback on the structure and length of the interview.
Data processing
With the participants’ consent, interviews were audio-recorded and transcribed verbatim. The audio recordings and the transcripts were pseudonymised by assigning a participant identification number to each interview. The analysis was facilitated using NVivo 12 software.
Data analysis
We followed the five steps recommended for conducting data analysis of TDF-based interviews (18).
Coding the interview transcripts
A line-by-line analysis of each transcript involved categorising monothematic parses of text referred to as ‘quotes’ (e.g., phrase, sentence, a collection of sentences conveying a single meaning) into TDF domains. For each domain, the quotes with a shared underlying meaning were then summarised into belief statements.
Inter-rater reliability of coding and coding scheme
Three authors independently annotated a proportion of interview transcripts. The inter-rater reliability (Krippendorff alpha) was estimated using methods developed by Hayes & Krippendorf (23). A Krippendorff alpha of α ≥ 0.80 was considered as an indication of high inter-rater agreement among the three authors. A coding scheme was developed based on the initial data analysis, which then guided the analysis of the remaining transcripts.
Generating specific belief statements
Specific belief statements about the barriers and enablers of physical activity were generated from the quotes. Specific belief statements are defined as a collection of responses with a similar underlying theme that suggests a problem and/or influence of the belief on the target behaviour (24). Strong evidence for a belief affecting the behaviour had to be present in each interview transcript for it to be coded as a quote. The frequencies of quotes supporting a belief statement (number of quotes, k) and the number of participants (n) were calculated.
Generating causal belief statements
Each transcript was assessed on the presence of lexico-syntactic patterns used to infer causality in natural language. The TDF domains and constructs that were linked, as evidenced by these patterns, were noted as being related to one another.
The following types of lexico-syntactic patterns inferring causality were extracted from the transcripts: 1) A causal statement about the event/experience/state indicated by the phrases such as ‘because’, ‘since’, ‘as a result of’, ‘this led to’, ‘due to’, (syntactic causal structures; (25); 2) A causal statement indicated by the use of causal verbs (e.g. ‘resulted in’, ‘decreased’, ‘increased’, ‘caused’, ‘made’); 3)A conditioning statement indicated by a semantic structure such as if-then and when-then. For example, ‘since I had a surgery, I became more confident in exercising’; 4) A counterfactual statement (26) which include statements supporting reasoning about consequences of hypothetical but feasible situations or events that are contrary to the actual situation or event (27).
The descriptions of perceived cause-effect relationships between TDF domains and physical activity were extracted from the transcripts and used in building a graph that represents this causal structure.
Identifying relevant theoretical domains
The belief statements were categorised according to TDF. The relevance of the domains was evaluated by three authors.
Quantification
Domains were judged as likely to be relevant for changing physical activity in HF if they were relatively pervasive (i.e., high number of quotes, k) and common (expressed by a large proportion of participants, n). For a belief to be considered relevant, it had to be expressed by more than two participants at least. If a specific belief has a low frequency (number of quotes, k) but was mentioned by all participants, it was identified as relevant to physical activity.
Differences between transcripts
The beliefs that were shared by all physically active individuals but not shared by sedentary individuals were judged as relevant.
Mapping specific beliefs onto theoretical constructs
Belief statements were mapped onto theoretical constructs. The constructs were chosen on the basis of how closely they described each belief statement in a single term. Standardised definitions of the constructs as described by TDF (18), the APA Psychology Dictionary (28) were adopted. Environmental Context and Resources constructs were adopted from HF guidelines (4). This has been done to situate the findings of this study in the vast body of literature on behaviour change and HF.
Techniques to enhance trustworthiness
The first interview was independently annotated using the TDF by three authors. The proportion of the quotes that the coders agreed were as follows: author 1 and author 2 (50.90%); author 1 and author 3 (30.43%); author 2 and author 3 (32.30%). The Krippendorff alpha – a measure of inter-rater reliability – was 0.69, 95% CI: [0.63; 0.75], with a 61% chance of falling below 0.70 if an entire sample of the interviews would be coded. Since a sufficient level of agreement (α ≥ 80) was not reached, another two interview transcripts (comprising 242 coded quotes in total) were annotated using a coding scheme that was developed as the result of independent data analysis of the first transcript and discussion among three authors.
The proportion of quotes that the authors agreed on was as follows: author 1 and author 2 (81.67%); author 1 and author 3 (71.67%); author 2 and author 3 (63.33%). The Krippendorff alpha was 0.797, 95% CI: [0.72; 0.87], with a 0.5% chance of alpha falling below 0.70 if it was estimated from the entire sample. Any new disagreements were discussed. The new coding scheme was developed based on the analysis of all three interview transcripts and disagreement discussion. The remaining 13 interviews (755 quotes in total) were annotated by the first author using this coding scheme.
Results
Recruitment
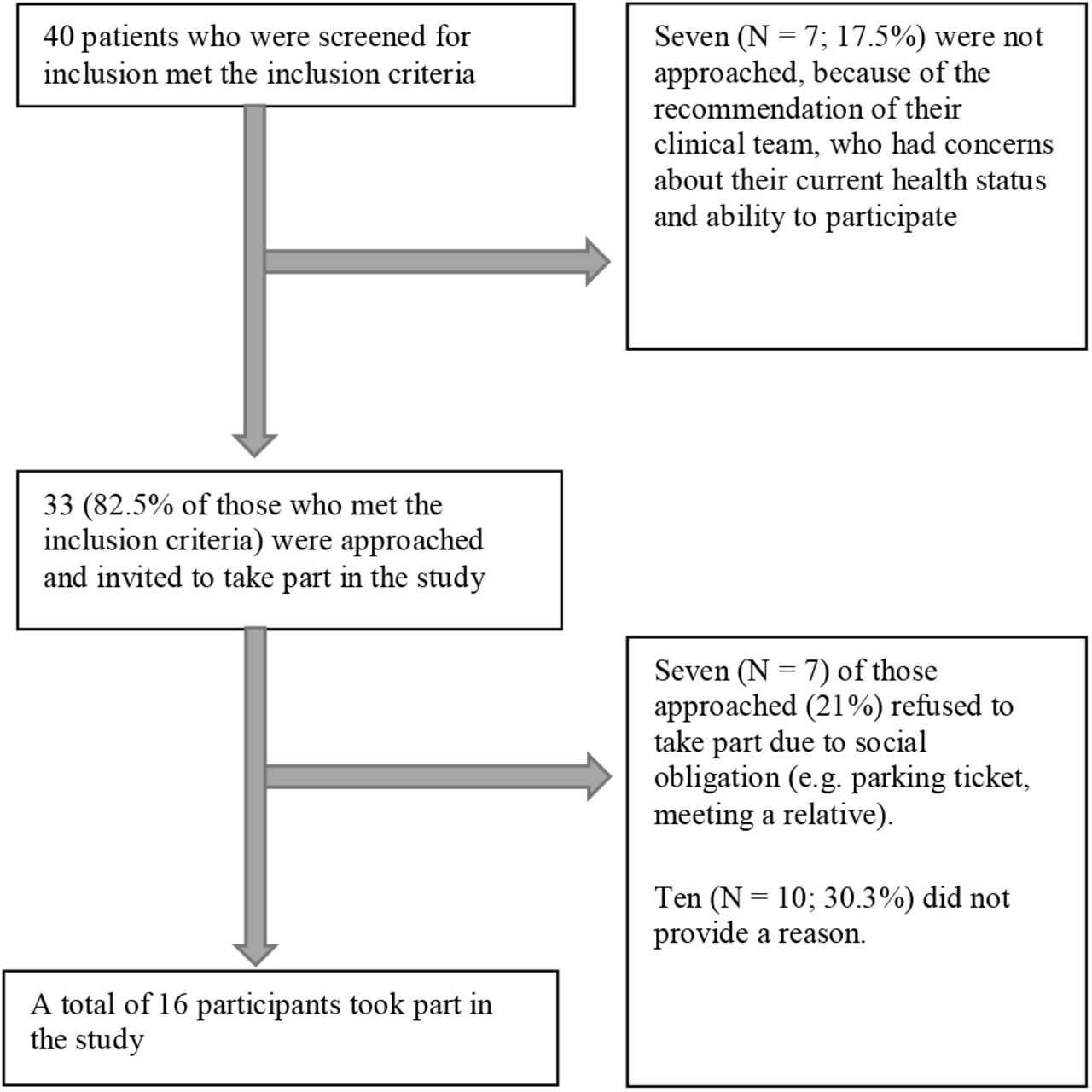
The participant recruitment is described in Fig 1. One-to-one interviews were conducted face-to-face in a research room available at RBHT (n=6), a vacant consultancy room (n=6) and via phone (n=4). All interviews were audio-recorded and transcribed verbatim. Interviews’ duration ranged between 15 to 85 minutes (mean = 41.24, SD = 20.97).

Participant characteristics
Participants’ characteristics are reported in Table 1. The final sample included 16 participants of a mean age of 79.19 (SD=5.15), four of whom were women, and 12 were men.
A total of 78 belief statements were produced from 16 transcripts. The corresponding constructs and the TDF domains, the number of quotes supporting them, and the number of participants expressing these beliefs are described in Table 2. The belief statements were mapped onto constructs and domains specified by TDF (12). The largest proportion of belief statements were coded as Environmental Context and Resources. The following domains were also judged to be relevant to physical activity based on the number of quotes: Beliefs about Consequences, Goal, Social Influences, Beliefs about Capabilities, and Behavioural Regulation.
Breathlessness reduced ability and damaged confidence (Beliefs about Capabilities); it led to persistent anticipation of negative outcomes of physical activity (Beliefs about Consequences). Due to this multifaceted influence of breathlessness on physical activity, it is identified as a major barrier to physical activity in HF.
Causal belief statements
The causal belief statements summarising the perceived links between domains that were shared by at least three participants are presented in Table 3. These were summarised into a causal graph (Fig 2).

{kind=link}
{kind=link}
Discussion
This study identified and described perceived barriers and enablers to physical activity in older adults living with HF. The following TDF domains were identified as relevant: Environmental Context and Resources, Beliefs about Capabilities, Goal, Behavioural Regulation, Beliefs about Consequences, and Social Influences. The specific beliefs summarising the barriers and enablers to physical activity are myriad (n = 78).
The lack of self-efficacy (Beliefs about Capabilities) influenced by the heart condition, comorbidities, and HF symptoms is suggested to be a pervasive barrier to physical activity in HF. Similarly, previous qualitative evidence suggests that ‘Changing Soma’ (29) due to age, comorbidities, and HF causes lack of perceived ability (i.e., ‘negative beliefs about perceived ability’ (30). In this study, the extent to which self-efficacy determined the engagement in physical activity was defined by the degree of breathlessness as well as comorbidity. In contrast to a previous qualitative study (29) suggesting that the change in the perception about oneself because of ageing’ influenced physical activity engagement, in this study, ageing was described to influence perceived capability rather than self-concept. Self-efficacy in its turn promoted resourcefulness in Behavioural Regulation (i.e., pacing oneself in accordance with perceived ability) as indicated by the causal belief statements.
The local environment and exercise equipment and facilities (Environmental Context and Resources) were reported as both barriers and enablers. It was identified as an enabler if it has the following attributes: available at home, flexible (e.g., exertion levels to accommodate different physical capacity levels), safe, and aesthetically pleasing in its appearance. An intervention typology (31,32) describes these features as essential for a successful nudging of the behaviour as functionality, availability and presentation, respectively. In HF, some tailoring to individual needs might be required (i.e., level of exertion being closely matched to their physical capacity and perceived ability).
The implantable device (Environmental Context and Resources) was a source of both – reassurance in, and worry about, physical activity. The NICE (4) and European Society of Cardiology (21) recommend low to moderate levels of activities in this population such as walking and daily activities, as well as soft aquarobics activities. Only sports of bodily collision and highly vigorous competitive sports are not recommended to this population group. Therefore, rightly so, participants regulated the type of activities they engaged in. However, several misconceptions surrounding their implantable device were still present. This included battery usage and wires imposing risk on the heart. As suggested by the review of the perceptions about cardiac implantable devices, education on the safety of the device would be helpful to individuals living with HF who were fitted with an implantable device.
Major health-related events, such as cardiac surgery, cancer surgery, heart attack, the first HF decompensation and subsequent hospitalisation, had a negative impact on physical activity for most of the participants (n = 7). These events were suggested to cause habit-breaking as indicated by the causal lexico-syntactic patterns’ analysis. The habit-breaking follows a short period of clinically recommended rest (approx. three months). To put it in the words of Participant 10: “I remember being told to be careful. Once you get out of the habit [post-surgery], it is hard to start again. It is difficult to start again because you forget.” In addition, such events in HF are associated with a drastic reduction in physical capacity. A significant life event – a crisis – is theorised to cause a shift in an individual’s identity (33,34). The salience of the event may result in a radical shift in beliefs (33,34). This is especially likely given the associated risks of sedentary behaviour in HF, including reliving the crisis all over again.
Behavioural Regulation influenced physical activity in HF. These included implementation intentions – strategies to execute a goal-directed behaviour in the face of barriers such as bad weather, forgetfulness (i.e., routine), fluctuation of perceived ability (i.e., pacing of physical activities when feeling unwell) (35). The following strategies that require focus and effort were also useful: action planning; and self-monitoring. These are consistent with: Self-regulation theory (36), and Dual process model of self-control (37). Behavioural Regulation implies prolonged effortful control of behaviour and restriction, which may result in ego depletion – the loss of motivation, cognitive resources, and the focus on the behaviour (38). Thus, making it an inconsistent enabler of the behaviour. Social and environmental resources such as social support and companionship (Social Influences) and monitoring devices (Environmental Context and Resources) were utilised to support Behavioural Regulation as indicated by the lexico-syntactic patterns’ analysis. Beliefs about Capabilities were causally linked to Behavioural Regulation constructs such as implementation intentions. Clinical advice (enabler) and reassurance, Companionship, Social support (practical), Social support (emotional, barrier), Social support (emotional, enabler), Social comparison, Social support (practical), and Social modelling were all suggested to influence physical activity in HF. These Social Influences were explicitly causally linked to Intention and Behavioural Regulation, as evident by the lexico-syntactic patterns. Three participants who self-identified as active were inspired by the positive example set by individuals they viewed as role models. Participants who did not self-identify as active intended to exercise only when provided with social support (practical and emotional) by others. Negative Beliefs about Consequences, such as negative outcome expectancies (i.e., symptom onset and hospitalisation), were causally linked to a weakened behavioural goal (Goal). Participants were less likely to form a strong behavioural goal to engage in physical activity if they held negative outcome expectancies about the behaviour. Action planning was motivated by the positive outcome goal (Goal): to remain functionally independent. A negative goal targeted at avoiding overdoing physical activity resulted in monitoring physical activity with an aim to reduce it.
Overall, the causal relationships between the identified barriers and enablers and described using lexico-syntactic patterns analysis in this study are consistent with Health Action Process Approach (39,40). The HAPA suggests that self-efficacy enables an individual to be resourceful in action planning and coping. This study supports the relevance of HAPA in explaining the driving forces of physical activity in HF, and thus it might be useful to employ this theory in developing physical activity interventions designed for individuals living with HF.
Breathlessness is suggested a key barrier to physical activity in this study and an overarching theme spanning two TDF domains: Beliefs about Capabilities and Beliefs about Consequences. However, breathlessness is also suggested is a somatic and emotional experience in HF. In cardiac disease, when cardiac output and oxygenation is suboptimal breathing is increased to provide appropriate oxygenation. Due to this, the physical capacity to engage in physical activity is reduced and it places a burden on the cardiopulmonary system. This results in Dyspnoea – a clinical symptom of shortness of breath. Breathlessness in HF is a threatening and aversive experience. Besides imposing physical restrictions in HF, breathlessness also directly punishes physical activity behaviour (Reinforcement: punishment). On the other hand, breathlessness is a fear-inducing somatic experience of HF and can be considered within the fear-avoidance model (41). In this context, perceived threat associated with breathlessness influence coping with HF and engagement in physical activity. Therefore, three interpretations of the impact of breathlessness on physical activity in stable HF exist: (a) Pavlovian conditioning; (b) operant conditioning (42); and (c) cognitive-behavioural response to symptoms. While the former two are concerned with habit breaking (i.e., model-free processes), the latter is concerned with the underlying cognitive and behavioural response to somatic experience (i.e., beliefs about symptoms, catastrophising and dyspnoea-related fear-avoidance beliefs).
Because breathlessness is associated with a heart attack, physical activity becomes punishing as it induces breathlessness. Such conditioning can be extinguished through repeated performance of physical activity. During this performance, the somatic state of being out of breath is not followed by pain or hospitalisation, so the pairing is unlearned. Not only punishment following physical activity needs to be lifted, getting out of breath on physical exertion needs to be paired with a positive reward. This happens in habitual physical activity over time when physical activity becomes intrinsically rewarding (43). However, for habitual physical activity to be established, an individual needs to practice and repeat the behaviour (44). Individuals living with HF find the experience of getting out of breath aversive enough that they do not engage in the behaviour at all in the first place. When they do persist, over time, their exercise capacity improves and permits them to engage in physical activity without limitations.
Strength and limitations
The participants recruited for this study are representative of the general population of individuals living with heart failure attending a specialist clinic in terms of their age and clinical and demographic characteristics. However, they may have a better clinical outcome than on average. This sample was hospitalised three times fewer days a year than the general population (45).
This study, using the TDF, was able to elicit a comprehensive list of relevant domains. Belief statements provide the basis for the content development of a scale designed to assess physical activity barriers and enablers in HF. The identified TDF domains suggest key constructs and domains that need to be investigated in a quantitative study. Causal belief statements were formulated to describe the causal links among the relevant TDF domains as perceived by the participants.
This study systematically described the causal links between relevant factors influencing physical activity in HF. The systematicity was facilitated by clearly defined criteria for inferring causality – lexico-syntactic patterns. This may impose a limitation, as it may have resulted in the omission of the links that are drawn implicitly without apparent lexico-syntactic patterns.
The assessment of the validity of the qualitative findings was carried out (46). Reflexivity and reflection were ensured throughout the study. A coding scheme, as well as the inter-rater reliability analysis, were carried out to improve reliability of the findings. The ecological validity of the findings was ensured through the recruitment of a representative sample and rich and thick verbatim analysis.
Clinical implication
According to the findings of this study, clinical advice and reassurance that reduces negative expectancies surrounding physical activity (e.g., secondary heart attack) are the first necessary means to physical activity change in HF.
The findings of this study also recognise that to improve physical activity engagement in HF, one should address the detrimental effect of breathlessness on the behaviour. It is essential to engage an individual in physical activity, gradually increasing the intensity and duration. Once an individual has built the physical capacity to engage in physical activity and has repeatedly been engaging in physical activity, they will experience exercise-induced breathlessness that is not followed by adverse outcomes, which will lead to a new learnt response to exercise-induced breathlessness.
Furthermore, an education programme differentiating HF-related dyspnoea from the expected exercise-induced breathlessness is needed (i.e., reassurance in the safety of physical activity even when it induces getting out of breath). Overall, according to the findings of this study, a cognitive behavioural intervention that addresses the fear-avoidance response to breathlessness is deemed helpful for engaging individuals living with HF in physical activity. The common approaches include Cognitive Behavioural Therapy (CBT) and Acceptance and Commitment Therapy, ACT (47,48). While CBT can address the maladaptive beliefs about breathlessness and negative emotional response (i.e., anxiety, fear), ACT can promote acceptance, reduce avoidant behaviour triggered by breathlessness and change maladaptive coping.
In addition, based on the findings of this study, it is recommended to engage individuals living with HF in a gradual increase in physical activity intensity, foster their skill mastery and use verbal persuasion, which may help improve physical activity self-efficacy (49). This study suggests that it is essential to set specific, measurable, achievable, relevant, time-bound physical activity goals and detailed action plans, including implementation intentions (i.e., if it rains, I will walk around the house). Similarly to the study informing REACH-HF intervention development (50), this study found that goal setting and behavioural regulation concerned with self-care behaviours in HF can be facilitated by instrumental and emotional social support. Therefore, it is recommended to set goals and make plans with others who have a similar level of physical capacity to engage in physical activity as those affected by HF. Thus, individuals living with HF might benefit from a walking group, where participants support each other in making explicit goals and action plans and social contracts to act on them.
The findings indicate a clear need for a behaviour change intervention that addresses the following perceived barriers: maladaptive beliefs about the major health-related event that preceded HF (e.g., heart attack, acute decompensation) and maladaptive beliefs about implantable devices that lead to fearful avoidance of physical activity. It is recommended to explore these beliefs in a non-judgemental and open manner, ensuring patient-driven change.
Therefore, it is evident that to tackle the barriers and amplify the enablers, a behaviour change intervention is needed. According to the findings of this study, this intervention should closely follow HAPA (39,40). In addition, there is a need for explicit clinical advice and reassurance in the safety of physical activity educational programme, CBT and ACT to take place as soon as possible after the major event. It is proposed to investigate the effectiveness and acceptability of such interventions in a RCT and subsequently consider these interventions for inclusion in clinical guidelines.
A broad range of professional expertise is required to support physical activity engagement in HF. Therefore, a multidisciplinary healthcare team comprising psychotherapists, clinical psychologists, HF nurses and cardiologists is needed to provide comprehensive healthcare and improve clinical outcomes in HF.
Conclusion
The present one-to-one interview study elicited 78 belief statements about barriers and enablers to physical activity in older adults (>70) living with HF. These belief statements and their pervasiveness across transcripts (i.e., the number of quotes) suggest that breathlessness (i.e., Dyspnoea), Beliefs about Capabilities, Environmental Context and Resources, Goal, Behavioural Regulation, Beliefs about Consequences, and Social Influences are most relevant to physical activity in HF. This study provides insights for cardiologists, HF-specialist nurses, and physiotherapists to help design and deliver a physical activity intervention to individuals living with HF.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Funding
This study was supported by a PhD studentship from City University London.
Bibliography



