
ABSTRACT
Objective This study aimed to investigate the effectiveness of the lower limb rehabilitation protocol (LLRP) using mobile health (mHealth) on quality of life (QoL), functional strength, and functional capacity among knee OA patients who were overweight and obese.
Materials and Methods In the current trial, 114 patients were recruited and randomized into either the rehabilitation group with mobile health (RGw-mHealth) receiving reminders by using mHealth to carry on the strengthening exercises of LLRP and instructions of daily care (IDC), the rehabilitation group without mobile health (RGwo-mHealth) following the strengthening exercises of LLRP and instructions of daily care (IDC) and control group (CG) only following the IDC for duration of 12-weeks. The reminders for using mHealth were provided two times a day for three days a week. Primary outcome measures were QoL assessed by the Western Ontario and McMaster Universities Osteoarthritis Index summary score, and functional strength by Five-Repetition Sit-To-Stand Test. Secondary outcome measure was functional capacity assessed by the Gait Speed Test. The assessments of QoL, functional strength, and functional capacity were taken at baseline and posttest after 12-weeks of intervention.
Results After 12 weeks of intervention, patients in all three groups had statistically significant improvement in QoL within groups (p < 0.05). Furthermore, patients in the RGw-mHealth and RGwo-mHealth had statistically significant improvement in functional strength and walking gait speed within groups (p < 0.05). The pairwise between-group comparisons (Bonferroni post hoc test) of the mean changes in QoL, functional strength, and functional capacity at posttest assessments revealed that patients in the RGw-mHealth had statistically significant greater mean change in QoL, functional strength and functional capacity relative to both the RGwo-mHealth and CG (p < 0.001).
Conclusion Improvement in QoL, functional strength, and functional capacity was larger among patients in the RGw-mHealth compared with the RGwo-mHealth or CG.
TRIAL REGISTRATION Chinese Clinical Trial Registry: ChiCTR1900028600
Date of registration: 28-12-2019
Registration Status: Prospective
- Osteoarthritis
- knee
- overweight
- rehabilitation
- mobile health
In the United States, doctor-diagnosed arthritis is a common chronic condition (1). Osteoarthritis (OA) is a degenerative disease in character and can lead to functional limitations and muscle weakness (2). A published article pointed out that OA is linked to joint wear and tear as well as inflammation of the synovial membrane (3). OA is a chronic disease that occurs in the knees, hips, hands, and spinal joints and causes pain, stiffness, and decreased range of motion (ROM) (4). Generally, populations do not prefer to participate in physical activity. Lack of time and different types of exercise were cited as major barriers (5, 6). OA causes a considerable burden on the quality of life (QoL) and medical treatment of patients (7). In 2015, Knee OA was the highest contributor among OA of the thirteenth leading cause of global disability (8) and it diminished QoL (9). The five-repetition sit-to-stand test (FRSST) test was used for the measurement of functional strength of the lower body. The FRSST measures the time taken to complete the repeated action of a stand five times from a sitting position as rapidly as possible (10). A person’s ability to cope with daily life activities is known as functional capacity (11).
Smart phone’s mobile health applications (mHealth apps) have the potential to play an important role in supporting personal health management (12). A current systematic review found that mHealth app users were more satisfied to manage their health than those of conventional care. The mHealth app users have resulted in a positive impact on health outcomes and health-related behaviors (13).
Exercise therapy is a safe and low-cost method for treating Knee OA that has been shown to delay disease progression and improve knee function (14). The Ottawa Panel found evidence to support the use of therapeutic exercises, especially strengthening exercise and general physical activity, for the improvement of functional characteristics in OA patients (15). A current systematic review on non-pharmacological interventions for treating symptoms of knee OA in overweight or obese patients resulted that the most effective intervention that showed improvement of knee function was strengthening exercise (16). Non-pharmacological interventions, primarily strengthening exercise and more recently strengthening exercises of the lower limbs in non-weight-bearing positions, are recommended as the first line of treatment among overweight or obese knee OA patients (17). The novelty of the current study could have been mediated by two factors, firstly it was provided as text messages and secondly the researchers designed a new lower limb rehabilitation protocol (LLRP) to treat overweight and obese knee OA patients. The training sessions of the LLRP are the strengthening exercises of the major muscle groups of the lower limbs in non-weight-bearing sitting and lying positions to reduce the mechanical load on the knee. However, there is insufficient evidence on the effectiveness of the LLRP by using mHealth on QoL, functional strength, and functional capacity among overweight or obese knee OA patients. Therefore, the objective of the current study was to investigate the effectiveness of the LLRP using mHealth on QoL, functional strength, and functional capacity among knee OA patients who were overweight and obese.
MATERIALS AND METHODS
Design and setting
The assessments of outcome measures of the current randomized controlled trial (RCT) were conducted in the Teaching Bay. The study was approved by the regional Ethical Committee with approval No: RAIC PESSI /Estt/2019/487 on date 28-08-2019 and the trial was registered in the Chinese Clinical Trial Registry with registration number:ChiCTR1900028600 on date 28-12-2019. The first patient in the trial was enrolled on the date 02-01-2020. Pre-defined questionnaire of inclusion and exclusion criteria was used for screening of the patients.
Study patients
Patients diagnosed with knee OA who were overweight or obese from the urban community were screened. According to World Health Organization, the individuals who have BMI ≥ 25kg/m2 are known as overweight and individuals who have BMI ≥ 30kg/m2 are known as obese (18). The sample included males and females diagnosed with 2-mild or 3-moderate OA according to Kellgren and Lawrence radiographic scale (19). The anteroposterior and lateral view of plain radiography of the affected knee/s were performed in the standing position.
The inclusion criteria were as follows: both males and females, overweight and obese knee OA patients; age 45-60 years; residing in an urban community. The exclusion criteria were as follows: system lupus erythematosus, rheumatoid arthritis, spondyloarthropathies, sjogren’s syndrome, gout, scleroderma, infectious arthritis; history of metabolic, hormonal, orthopaedic, cardiovascular disease; spinal deformities; flat feet; previous surgery of knee/s of any cause or injection of knee/s for the last 6-months. The experimental procedures, risks, and benefits associated with the study were explained to all patients prior to providing written informed consent.
Sample size
Sample size estimation was performed using the G* Power 3.1.3 software. By assuming the medium effect size f = 0.70, setting α = 0.05, power (1-B) = 0.80, the total sample size estimated was 30 patients for each group. After considering 20% drop-out rates, the sample size of 114 patients for the three groups was decided.
Patient’s recruitment and selection
Patients were recruited from the urban area using convenience sampling by active recruitment strategies through the political and welfare organizations. A study coordinator explained the criteria of knee OA patients as well as benefits of study participation to the political and welfare organizations. These organizations explained the benefits to the expected knee OA patients in the recruitment area via word of mouth and presented a list of expected knee OA patients to a study coordinator. The study coordinator prepared a list of potential patients based on the inclusion and exclusion criteria of the study and approved a final list of patients to contact. Then, the study coordinator called patients to attend a meeting in the Teaching Bay to further assess eligibility. Patients who were eligible and interested in participating completed a written informed consent for their participation in the study. Prior to the intervention, patients’ baseline measurements were completed
Blinding and Allocation
The coordinators collecting data were independent individuals from the trials and were unaware of the group allocation. There were different coordinators at the baseline and post-test evaluation. Individuals performing the statistical analysis were kept blinded by labelling the groups with non-identifying terms (such as X and Y).
Study Randomization
After completing the screening for eligibility, the selected patients were randomized into one of three groups: rehabilitation group with mobile health (RGw-mHealth), rehabilitation group without mobile health (RGwo-mHealth) or control group (CG) by a computer-generated number. Each group consisted of thirty-eight patients. All patients were also given a diary and asked to record the attendance of completion their interventions based on leaflets.
Research procedures
Rehabilitation group without mobile health (RGwo-mHealth)
Patients in the RGwo-mHealth were taught on how to perform the strengthening exercises of LLRP by following the IDC. The contents of IDC were explained elsewhere (17). Patients were advised to continue performing the training sessions of LLRP 3-times a week for 12-weeks at home. These trainings included strengthening exercises for the lower limbs in non-weight-bearing sitting, or lying positions (Table 1) without putting a mechanical load on the knee.
Lower Limb Rehabilitation Protocol (LLRP)
Each training session started with ten minutes of warm-up, forty-five to sixty minutes of lower limb strengthening exercises, and ten minutes of cool down at the end of the training protocol (Table 1). The study demonstrated that dynamic stretching is recommended for warm-up to avoid a decrease in strength and performance (20). When the static stretching was used as part of a warm-up immediately prior to exercise, then it causes harm to muscle strength (21). The study explained that after two to four repetitions of static stretching, there is no increase in muscle elongation (22). A cool-down period is essential after a training session and should last approximately 5 to ten minutes (23, 24). Additionally, regular messages were also sent to the RGwo-mHealth for intention control.
Rehabilitation group with mobile health (RGw-mHealth)
Patients in the RGw-mHealth were prescribed with the LLRP as described in the RGwo-mHealth. Additionally, they receive regular reminders to carry out of LLRP using mHealth in the form of periodic manual WhatsApp messages. Two text messages per day for three days a week for a period of 12-weeks were sent to patients in the RGw-mHealth. Patients in this group received a total 72 text messages. The researcher sent text messages between 7:00 to 9:00 a.m. and 5:00 to 7:00 p.m. during the days of Wednesday, Friday, and Sunday. A study reported that sending text messages in the morning was to make sure that the patients have enough time to plan and do exercise during the day (25). The screen view for sending the text messages is shown in additional file 1.
Control group (CG)
Patients in the CG only followed the IDC for the duration of 12-weeks. The IDC contents include advice on general guidelines of mobility and healthy eating (Table 2). The contents of IDC were translated into Urdu language by two language experts to ensure better patients’ understanding based on a recent pilot study (17). Regular messages were also sent to the CG for intention control.
Instructions of daily care (IDC)
Measurements
Patient’s demographics, QoL, functional strength, and functional capacity were assessed at baseline before randomization. Similarly, the assessments of demographics, QoL, functional strength, and functional capacity were repeated at posttest after 12 weeks of intervention. The demographic questionnaire covered age, gender, socioeconomic status, and employment. Outcome measures were categorized into primary and secondary outcome measures.
Primary Outcome Measures
Primary outcome measures were QoL and functional strength. To evaluate QoL, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) summary score that was already adapted and validated was used (26). Three dimensional (pain, stiffness, and physical function) QoL questionnaire was designed for the evaluation of the hip and knee OA. The WOMAC score ranges from 0 to 4 on a Likert-type scale, with higher scores indicating an increase in pain, joint stiffness, and reduced functionality (27).
The FRSST was used for the assessment of lower body functional strength. The FRSST has a high test-retest reliability for adults and subjects with knee OA (28, 29). A straight armless chair with 43 cm of back support height was stabilized on the wall. Patients were asked to come forward on the chair seat in a position of standing, until the feet are flat on the floor. Patients were instructed to stand up and sit down once without using the upper limbs as a test purpose. For those who needed assistance, assistance was provided to complete the test. Patients were then asked to stand up and sit down as quickly as possible five times. Timing with a stopwatch was started on the command go and ceased when the patient completed the 5th set of sit to stand. The time taken was recorded as the patients’ score.
Secondary outcome measures
Secondary outcome measure was the functional capacity. The Gait Speed Test (GST) was used for the assessment of the functional capacity. In the GST, the time was recorded when the patient completed a distance of 20 feet and then divided the distance to time for the calculation of gait speed. Gait speed measures obtained during a single test session are reliable. The coefficients (0.90) of comfortable gait speed were highly reliable (30). The GST is used as an outcome measure in rehabilitation (31) and in trials of interventions to delay the onset of disability or frailty (32).
Statistical procedures
The Statistical Package for Social Sciences, version 22, Chicago, IL, was used to analyze the data. Continuous variables were presented as mean (standard deviation [SD]) based on data distribution. The Shapiro-Wilk test was used to assess the normality of all variables. Categorical variables were presented as frequencies (n) and percentages (%). For categorical demographic variables, the One-Way Analysis of Variance (ANOVA) was used to compare for differences between variables. Since all data was normally distributed; the Paired Samples t-test was used to analyze differences between the baseline and post-test assessments within the groups.
The overall treatment effects on change in clinical outcome measures were estimated using the One Way ANOVA (unadjusted results) and Analyses of Covariance (ANCOVA, adjusted results) for mean changes (95% confidence interval [CI]) from baseline to posttest assessments in the continuous outcome data. The ANCOVA model included the changes as the dependent variable, with group as a main effect and the baseline scores as an additional covariate. The purpose of using the pretest (baseline) scores as a covariate in ANCOVA with a pretest-posttest design is to reduce the error variance and eliminate systematic bias [33]. The pairwise comparisons between groups were estimated using Bonferroni post hoc test. The value of p ≤ 0.05 was considered statistically significant.
RESULTS
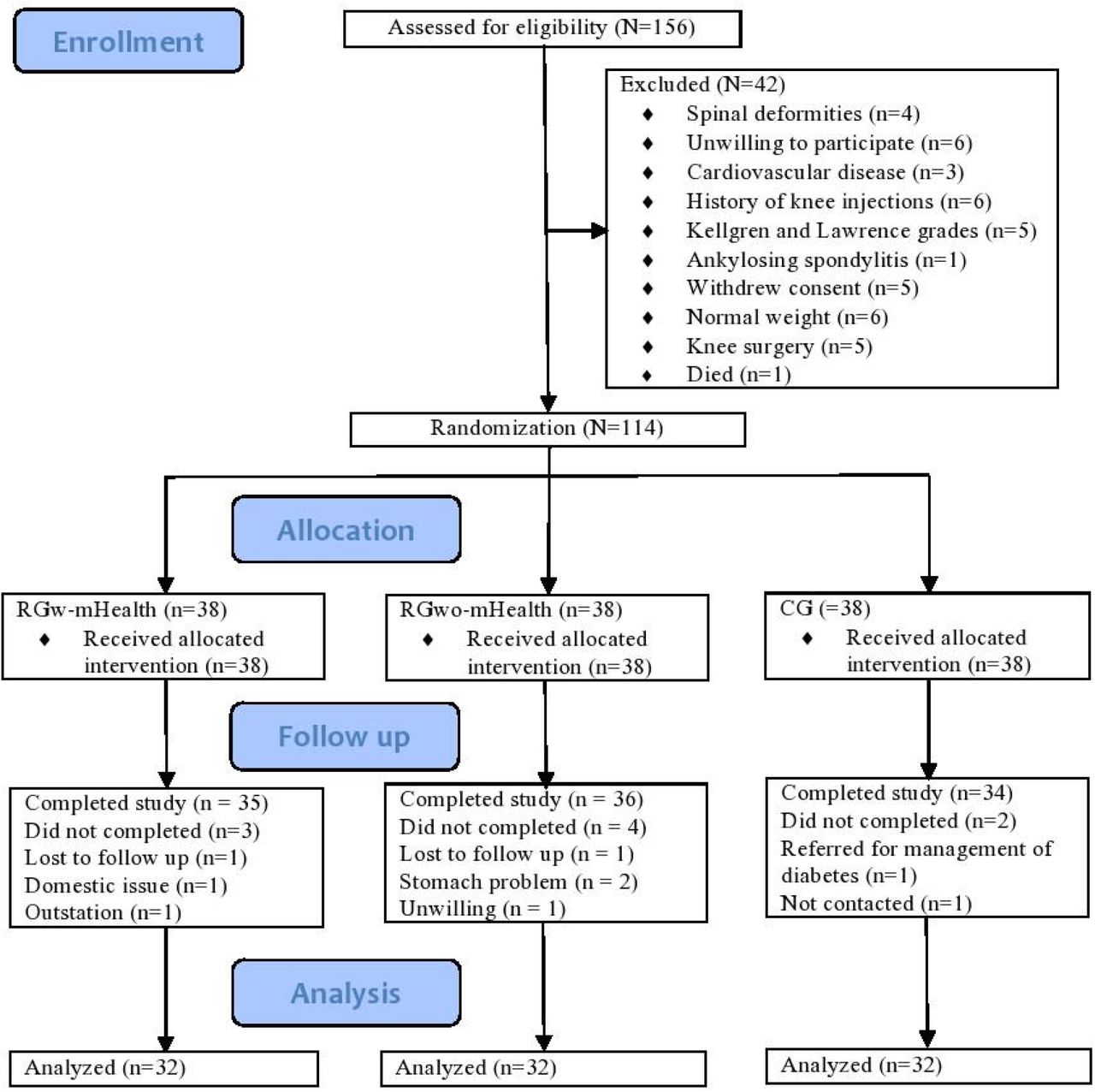
Figure 1 shows a patient flow chart in the current study. A total of 156 overweight and obese knee OA patients were initially enrolled and assessed for eligibility. Among them, 42 patients were excluded for reasons as shown in Figure 1. The remaining 114 were randomized equally into three groups. The post-intervention outcomes were not obtained for the 18 withdrawn patients. Figure 1 demonstrates the study flow chart including reasons given by patients who did not complete the study. A final total of 96 patients (32 in the RGw-mHealth, 32 in the RGwo-mHealth, and 32 in the CG) were included in the analysis of QoL, functional strength and functional capacity.

{kind=link}
Non-completers did not differ significantly from completers in terms of age, gender, socioeconomic status, employment, QoL, functional strength, and functional capacity. Similarly, retention did not differ among the groups (RGw-mHealth, 84%; RGwo-mHealth, 84%; CG, 84%). Two serious adverse events (one appendix surgery in the RGw-mHealth and one gallbladder surgery in the RGwo-mHealth) were unrelated to the study. One nonserious adverse event of muscle spasm in the CG was noted during the study and it was related to the study.
Summary of the overall and baseline demographic characteristics and assessment scores of the QoL, functional strength, and functional capacity are described in Table 3. After participation in the 12-weeks of intervention, a statistically significant improvement compared to baseline was observed for QoL, functional strength, and functional capacity scores in the RGw-mHealth and RGwo-mHealth. In the CG, improvement in QoL score was also statistically significant (Table 4).
Summary of the overall and baseline demographic characteristics and assessment scores of the QoL, functional strength and functional capacity of patients
Change in clinical outcome measures from baseline to post-test after 12-weeks of interventions within groups
The mean changes in QoL scores were 9.11 (95% CI 8.28, 9.93), 4.38 (95% CI 3.57, 5.18), and 0.89 (95% CI 0.08, 1.71) for patients in the RGw-mHealth, RGwo-mHealth and CG respectively (Table 5). The pairwise between-group comparisons of the QoL score at post-test revealed that patients in the RGw-mHealth had significantly better QoL scores relative to both the RGwo-mHealth (difference, 4.72 [3.31, 6.14]; p < 0.001) and CG (difference, 8.21 [6.76, 9.66]; p < 0.001). There was also a statistically significant difference in the mean QoL scores between the RGwo-mHealth and CG (difference, 3.48 [2.08, 4.88]; p < 0.001) (Table 6).
Unadjusted and adjusted treatment effects on change in clinical outcome measures from baseline at post-test after 12 weeks of interventions and significance between groups
The pairwise comparisons between groups by Bonferroni test (post hoc test)
Table 5 presents the mean change in the FRSST (seconds), as an indication of the participant’s functional strength change after 12-weeks. The mean change in FRSST scores in the RGw-mHealth, RGwo-mHealth, and CG were 4.66 seconds [95% CI 3.90, 5.43 seconds], 2.87 seconds [95% CI 2.14, 3.60 seconds] and 1.44 seconds [95% CI 0.67, 2.22 seconds] respectively. As indicated by the overall ANCOVA, there was a statistically significant change in functional strength between groups (p < 0.001) after 12 weeks of intervention. The pairwise between-group comparisons of the mean change in functional strength at post-test revealed that patients in the RGw-mHealth had statistically significant greater mean changes in functional strength relative to both the RGwo-mHealth (difference, -1.79 [-3.07, -0.51]; p = 0.003) and CG (difference, 3.22 [1.81, 4.62]; p < 0.001). There was also a statistically significant difference in functional strength between the RGwo-mHealth and CG (difference 1.42 [0.10, 2.74]; p = 0.030) as shown in Table 6.
Patients in the RGw-mHealth had a mean change in gait speed of -23.75 (95% CI - 26.50, -21.01) at post-test, whereas patients in the RGwo-mHealth and CG demonstrated a gait speed mean change of -8.98 (95% CI -11.72, -6.24) and -1.15 (95% CI -3.88, 1.57) respectively as shown in Table 5. The pairwise between-group comparisons of functional capacity at posttest revealed that patients in the RGw-mHealth had a significantly larger mean changes in functional capacity score compared to both the RGwo-mHealth (difference, 14.77 [9.98, 19.56]; p < 0.001) and CG (difference, -22.60 [-27.36, -17.835]; p < 0.001). There was also a statistically significant difference in the mean change in functional capacity between RGwo-mHealth and CG (difference, -7.82 [-12.56, -3.08]; p < 0.001) as shown in Table 6.
DISCUSSION
The core recommended treatments for OA in OA clinical guidelines are lower limb muscle strengthening (34). Exercise is often indicated as one of the main components in the rehabilitation process (35). Effectiveness of rehabilitation combined with mHealth may provide more objective data than the standard rehabilitation approaches we are using today to treat overweight and obese knee OA patients. Therefore, the current study investigated the effectiveness of the LLRP using mHealth on QoL, functional strength, and functional capacity among knee OA patients who were overweight and obese. We reached the conclusion that in RGw-mHealth patients, the scores of QoL, functional strength, and functional capacity were significantly higher than RGwo-mHealth or CG. The results indicated that patients in the RGw-mHealth who received additional reminders of the intervention combined with WhatsApp messages showed greater improvements in QoL, functional strength, and functional capacity than did the patients in the RGwo-mHealth or CG. In the current study, knee OA was more common in females, while there was no difference in terms of age. The mean age of the overall sample was 53.00 years (SD = 4.60 years). The majority of the study patients were employed (60.5%), and had lower socioeconomic status (69.3%).
In a randomized clinical trial of 316 overweight or obese elderly men and women with knee OA, it was noted that the combination of diet and exercise was more successful in improving health-related QoL, if compared with exercise or diet as single interventions (36). Because there is no cure for this condition, current medical practice focuses on such interventions that reduce the progression of the disease and the negative impact on health-related QoL (37). A recent study concluded that the progressive resistance strength training of LLRP is effective in improving QoL among overweight and obese knee OA patients (38). In the current study, the patients in the RGw-mHealth resulted significantly better QoL compared to both the RGwo-mHealth and CG.
Recently, a study demonstrated that a combination of dietary weight loss and exercise intervention was consistently better in improving a combination of performance and functional outcomes among participants with knee OA compared with exercise alone, diet alone, or a control group (39). In a recent study, a combination of IDC with the strengthening exercises of the major muscle groups of the lower limbs in non-weight-bearing positions resulted in improving functional capacity in overweight and obese knee OA patients (38). Similarly, in the current study the intervention in the patients of RGw-mHealth and RGwo-mHealth was also a combination of IDC and progressive LLRP that reported significant results in improving functional capacity. According to the Osteoarthritis Research Society International Committee for Clinical Trials Response Criteria Initiative and the Outcome Measures in Rheumatology Committee, response to treatment in clinical trials should be based on symptomatic response to therapy in the domain of function, and the patient’s global assessment (40). Data from a study involving knee OA patients who were obese highlight an opportunity to improve the QoL scores by following nutritional education and dietary guidelines (41). In the current study, the IDC also focused on the caloric restriction diet.
Many trials of different physical activity and exercise-based interventions reported the improvement of function among knee OA patients (42). Patients in the RGw-mHealth had statistically significant greater functional strength compared to both the RGwo-mHealth and CG. This may be due to the strengthening exercises of LLRP that were performed in non-weight-bearing positions by patients in the RGw-mHealth in the current study. These strengthening exercises resulted in increased strength of the lower limb muscles. Therefore, the patients in the RGw-mHealth had better improvement in the score of functional strength than the patients in the RGwo-mHealth and CG.
In a meta-analysis, it was indicated that the number of directly supervised exercise sessions can influence the extent of the treatment effect (43). In the current study, the strengthening exercise sessions in the RGw-mHealth were performed 3 times a week for 12 weeks (36 sessions) by sending periodic manual WhatsApp messages as a reminder to perform their intervention. Therefore, the treatment effects of patients in the RGw-mHealth were better than the patients in the RGwo-mHealth and CG.
Based on these findings, the strengthening exercises of LLRP using mHealth are expected to be more effective in terms of improving functional strength, functional capacity, and QoL than any other rehabilitation intervention among overweight and obese knee OA patients. The strengthening exercises of LLRP by using mHealth may have the potential to improve QoL, functional strength, and functional capacity among overweight and obese knee OA patients. These exercises may have the great contribution to the body of knowledge internationally because these are performed in non-weight bearing sitting or lying positions with minimal load at the knee joint. In addition, this rehabilitation protocol is easy to use in the home care setting and may be helpful in treating many bedridden conditions such as multiple sclerosis, hemiplegia, paraplegia and neurological diseases with lower limb weakness.
The present study had some limitations. It was conducted in a single centre to recruit patients. No long-term follow-up records were taken. Thus, further blinded studies across multiple centres and long-term follow-up are required to confirm the results of the strengthening exercises of the LLRP combined with mHealth in overweight and obese knee OA patients. Additionally, physical activity, psychosocial, and comorbidity factors may influence the outcomes. Therefore, further research considering these additional factors is required to confirm the findings of the study.
In conclusion, patients in the RGw-mHealth had better improvement in functional strength, functional capacity, and QoL than those in the RGwo-mHealth and CG. The results of the current study suggest that improvements in functional strength, functional capacity, and QoL among knee OA patients who are overweight or obese, are augmented better by the implementation of the LLRP using mHealth to rehabilitation or general treatment without mHealth.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.
Data Availability
The data used to support the findings of the study are available from the corresponding author upon request.
Footnotes
Emails: Muhammad Tariq Rafiq: drtariqrafiq149{at}yahoo.com; Mohamad Shariff Abdul Hamid: ayip{at}um.edu.my; Eliza Hafiz: eliza{at}um.edu.my
REFERENCES



