
Abstract
Importance The case fatality rate of SARS-CoV-2 has been high among residents of long-term care (LTC) facilities. It is important to know if the excess mortality persists beyond the acute infection.
Objective To evaluate whether SARS-CoV-2 is associated with higher mortality after the first month from documented infection.
Design We extended the follow-up period of a previous, retrospective cohort study based on the Swedish Senior Alert register. LTC residents infected with SARS-CoV-2 were matched to uninfected controls using time-dependent propensity scores on age, sex, body mass index, health status, comorbidities, and prescription medication use. In a sensitivity analysis, residents were also matched on geographical region and time of Senior Alert registration.
Setting LTC facilities in Sweden.
Participants 3731 LTC residents with SARS-CoV-2 and 3731 controls (n=3604 in each group in the sensitivity analysis).
Exposure SARS-CoV-2 infection, documented in the SmiNet register (until September 15, 2020).
Main Outcome All-cause mortality over 8 months (until October 24, 2020).
Results The median age was 87 years, and 65% were women. Excess mortality was highest 5 days after documented infection (hazard ratio 19.1; 95% confidence interval [CI], 14.6-24.8), after which excess mortality decreased rapidly. After the second month, the mortality rate became lower in infected residents than in controls. Median survival of uninfected controls was 577 days (1.6 years), which is much lower than national life expectancy in Sweden at age 87 (5.05 years in men, 6.07 years in women). During days 61-210 of follow-up, the hazard ratio for death was 0.41 (95% CI, 0.34-0.50) in the main analysis and 0.76 (95% CI, 0.62-0.93) in the sensitivity analysis.
Conclusions and Relevance No excess mortality was observed in LTC residents who survived the acute SARS-CoV-2 infection (the first month). The life expectancy of uninfected residents was much lower than that of the general population of the same age and sex. This difference should be taken into account in calculations of years of life lost among LTC residents.
Question Does SARS-CoV-2 increase mortality in residents of long-term care (LTC) facilities beyond the first month (that is, beyond the acute infection)?
Findings In a matched cohort study, we found that excess mortality was high during the first month but then decreased sharply. After the second month, the mortality rate became lower in infected residents than in uninfected controls.
Meaning No excess mortality was observed in LTC residents who survived the acute SARS-CoV-2 infection.
Introduction
During the COVID-19 pandemic, many of the COVID-19 deaths that occurred in high-income countries were seen in long-term care (LTC) facilities,1 where case fatality rates were 10-40% or even higher.2,3 We have previously reported that 30-day mortality in Swedish LTC was 40% in residents infected with SARS-CoV-2 versus 6% in matched, non-infected controls.4 A natural follow-up question to ask is whether SARS-CoV-2 also increases the risk of death beyond the acute period of 30 days, i.e. whether it has long-term effects on mortality in LTC residents who recover from infection. A major concern is that LTC residents who recover from SARS-CoV-2 infection may have residual debilitation caused by the infection. If so, this may affect also their life expectancy beyond the acute phase of the infection. Moreover, it would be interesting to estimate the loss of life expectancy in LTC residents infected with SARS-CoV-2. We set out to answer these questions by extending the follow-up period in our previous analysis from 30 days to 8 months.
Methods
The study offers extended follow-up on a retrospective cohort study. The basic study design of the retrospective cohort and of selection of exposed (infected) and unexposed (uninfected control) residents was described in detail previously in the publication presenting 30-days of follow-up.4 In brief, data on Swedish LTC residents were obtained from Senior Alert, a database of health assessments performed in older adults aged ≥65 years.5 All residents of LTC facilities in Sweden registered in Senior Alert were eligible to be considered. Senior Alert collects health data on various conditions in adults aged ≥65 years. Senior Alert captures an estimated 73% of all Swedish LTC facility residents. We selected LTC residents who had a record in Senior Alert from 2019 or 2020; the latest record during these years was used, whenever there were multiple records. Linkage used pseudo-anonymized Personal Identification Numbers. Among these, we identified 3731 LTC residents with confirmed SARS-CoV-2 until September 15, 2020. Each infected resident was matched to a control resident on age, sex, body mass index, health status, comorbidity, and prescription medication use. Data on SARS-CoV-2 infections were obtained from the SmiNet national registry where SARS-CoV-2 infections must be reported by law. The study outcome was all-cause mortality (until October 24, 2020). These data were obtained from the national Swedish Cause of Death Registry. Information on comorbidities was obtained from the Swedish National Patient Register and for cancer outcomes from the Swedish Cancer Registry. Information on recent use of medications (prescriptions in 2019-2020) came from Senior Alert and the Swedish Prescribed Drug Register.
We excluded SARS-CoV-2 infected residents that did not have a record in Senior Alert within a year prior to date of testing or confirmed infection (whichever came first or was available) and those where dates of testing and confirmed infection were both unavailable.
Infected residents and uninfected controls were 1:1 matched with time-dependent propensity scores, so as to allow for the fact that exposure (date of documented SARS-CoV-2 infection) did not coincide with the time of cohort entry (date of Senior Alert record). With time starting at the date of the Senior Alert record, a Cox model calculated a propensity score for the propensity to contract SARS-CoV-2. Each infected resident was matched to the control with the closest propensity score among those who were still alive when the SARS-CoV-2 case occurred (counting time since the Senior Alert date). Matching was done sequentially, starting with the first case (smaller number of days since cohort entry) and proceeding with cases with increasingly larger number of days since cohort entry. Diagnoses and medications were used as time-varying covariates in the Cox regression model.
We conducted a sensitivity analysis to examine whether the results were confounded by secular trends and geographic variations in mortality. To do this, matching included also the region (21 categories) and the date (year and month) of Senior Alert registration. Using this matching procedure, 3604 infected residents could be matched to an equal number of uninfected controls.
In both the main and sensitivity analyses for death risk, all-cause mortality was considered as the outcome of interest and the starting date for follow-up was the SARS-CoV-2 documentation date in infected residents and the corresponding date (in days since cohort entry) in controls. Follow-up time in days was calculated as censor date (24 October 2020 or death whichever came first) minus baseline date + 1 day. This was done so that the baseline date could also be included in the follow-up time and analysis (thus, a person would be able to die on the same date as they were documented to be infected).
The absolute risk of death was examined using Kaplan-Meier plots. The hazard ratio (HR) for death was plotted over time using flexible parametric models with restricted cubic splines (4 knots in default positions). HRs and 95% confidence intervals (CIs) were also estimated using Cox regression for 30-day intervals of follow-up until 210 days. To adjust for matching, we calculated 95% CIs in the Cox models and the flexible parametric models using robust standard errors.
Analyses were performed using Stata MP version 16.1 for Mac (StataCorp, College Station, TX).
The study was approved by the Swedish Ethical Review Authority, which waived the informed consent requirement (no. 2020-02552). No patients were consulted in the study.
Results
In the main analysis, median baseline date for infected residents was 27 Apr 2020 (IQR 10 Apr to 22 May), median (maximum) follow-up was 129 (246) days and there were 1713 deaths. For controls, median baseline date was 12 Apr 2020 (IQR 16 Dec 2019 to 30 Jun 2020), median (maximum) follow-up was 146 (641) days and there were 899 deaths. In the sensitivity analysis, for infected residents, median baseline date was 26 Apr 2020 (IQR 10 Apr to 21 May), median (maximum) follow-up was 130 (246) days and there were 1640 deaths. For controls, median baseline date was 28 Apr 2021 (IQR 9 Apr to 23 May), median (maximum) follow-up was 173 (249) days and there were 536 deaths. The median age was 87 years, 65% were women, and comorbidities were common (Table 1).
Baseline characteristics
As previously reported, SARS-CoV-2 was associated with a sharp, early increased risk of death: 40% versus 6% within 30 days (1487/3731 versus 211/3731). However, extending the follow-up period showed that the risk soon plateaued (Figure 1A). Similar results were seen in the sensitivity analysis (Figure 1B).

Risk of death in residents with SARS-CoV-2 and controls in the main analysis (panel A) and in the sensitivity analysis (panel B). The colored areas show the 95% CI.
Survival of controls at 210 days was 74.3% (72.6%-75.9%) in the main analysis and 82.9% (81.3%-84.4%) in the sensitivity analysis. Median survival of controls was 577 days. Median survival was also 577 days among the controls who were matched to the 1487 infected residents who died in the first month. Survival of these 1487 controls was similar to the survival of the remaining 2242 controls, for example their survival at 210 days was 72.5% versus 75.4%.
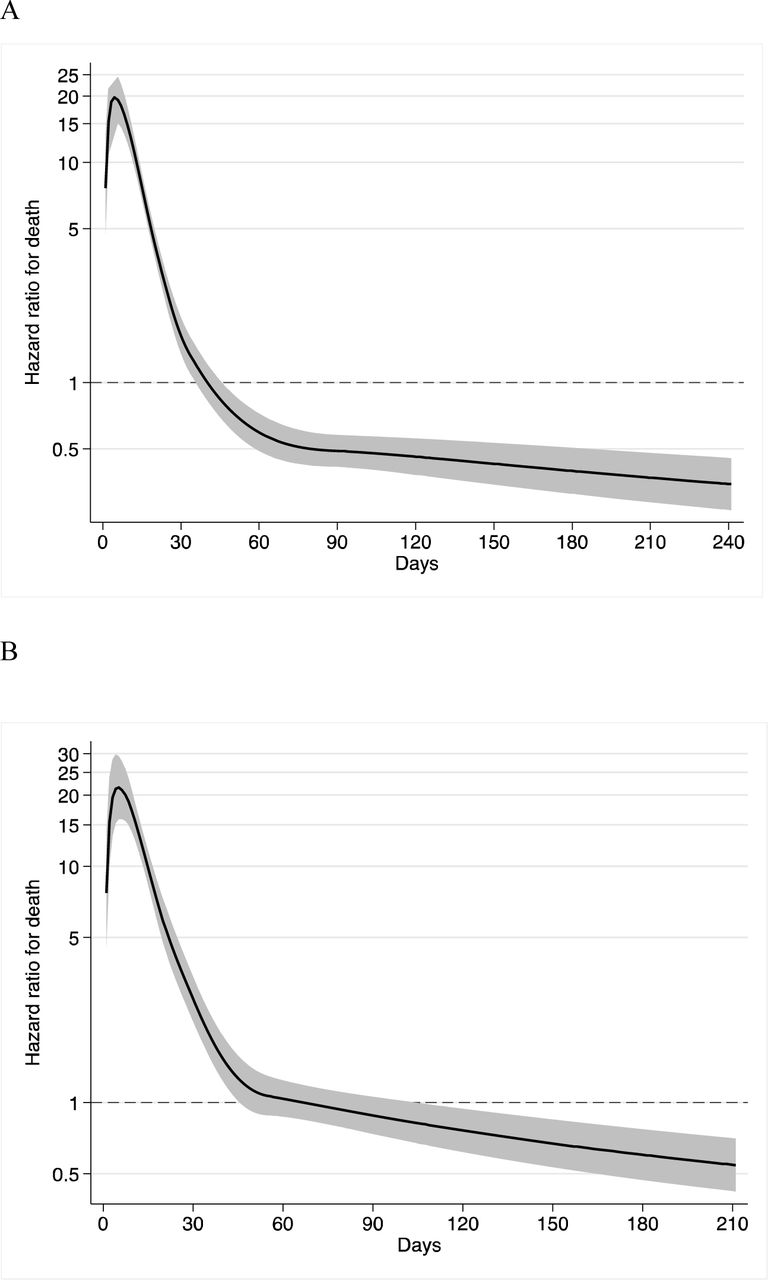
Peak HR (19.1 (95% CI, 14.6-24.8)) occurred at 5 days after documented infection. HR was high in the first month, decreased below 1.0 early in the second month, and remained below 1.0 for the remaining duration of follow-up (Figure 2). In the sensitivity analysis, peak HR was 21.5 (95% CI, 15.9-29.2). Again, HR decreased sharply but took a bit longer to drop below 1.0 (after the second month) and remained below 1.0 afterwards.

{kind=link}
{kind=link}
Hazard ratio for death in residents with SARS-CoV-2, as compared with controls in (A) the main analysis and (B) the sensitivity analysis.
In the main analysis, for 0-30 days, there were 1487 deaths among infected residents (17.57 deaths per 1000 person-days) versus 211 in uninfected controls (1.88 deaths per 1000 person-days), resulting in a HR of 8.81 (7.64-10.15). For 31-60 days, there were 93 deaths (1.42 per 1000 person-days) versus 144 (1.42 per 1000 person-days) (HR 1.00 (0.77-1.30)). For 61-90 days the respective numbers were 33 (0.55) versus 121 (1.38) (HR 0.38 (0.26-0.55)). For 91-120 days, the respective numbers were 38 (0.63) versus 126 (1.72) (HR 0.36 (0.25-0.52)). A similar pattern was seen for 121-150 days (HR, 0.52 (0.36-0.76)), 151-180 days (HR 0.47 (0.28-0.79)), and 181-210 days (HR 0.29 (0.10-0.83)).
During the 61-210 days follow-up, there were 133 deaths among infected residents (0.58 per 1000 person-days) versus 420 deaths among the uninfected controls (1.37 per 1000 person-days), with the HR being 0.41 (0.34-0.50). In the sensitivity analysis, during 61-210 days of follow-up, there were 131 deaths (0.59 per 1000 person-days) in infected versus 278 deaths (0.78 per 1000 person-days) in controls, with the HR being 0.76, 95% CI, 0.62-0.93).
Discussion
In this extended follow-up analysis of mortality in SARS-CoV-2-infected versus uninfected control LTC residents, we found that mortality risk peaked during the first week of documented infection, after which it rapidly decreased. Mortality remained elevated for the first month after infection, but then reverted back to baseline levels (i.e., control levels) before it dropped below baseline levels, where it remained at low levels for the remaining duration of follow-up (up to 8 months). These results suggest that SARS-CoV-2 does not reduce the life expectancy of LTC residents who survive the acute period of the disease. Despite concerns that infected residents who survive may have persistent residual debilitation that might enhance their subsequent death risk, we saw the opposite: death risk decreased in longer-term follow-up. This suggests that deaths due to COVID-19 in LTC facilities in Sweden during the first wave probably resulted in average loss of life expectancy of less than 1.6 years on average. This figure is much lower than the life expectancy in the general Swedish population, which in 2019 was 5.05 years for men and 6.07 years for women at the age of 87 (the median age in our study).7
Calculations of burden of disease due to COVID-19 often use age- and gender-adjusted life expectancies to calculate years-of-life-lost; however, without properly accounting for LTC residence and general health. Our findings suggest that such an approach can yield massively inflated estimates.8 Adjustment for comorbidities has been shown to decrease the number of years-of-life-lost in some studies.9-11 However, the change is typically modest (e.g., in the range of 1 years) and much smaller than what we observed in the LTC resident population that we evaluated. It is possible that in most studies, information on comorbidities is not available in sufficient granularity and accuracy regarding severity. E.g., “kidney disease” would carry very different risk connotations depending on the stage and severity. LTC resident status is a surrogate for increased frequency and severity of many comorbidities and of overall frailty. Therefore, it should be taken into account as a first correction for any years-of-life-lost estimates for COVID-19 burden of disease calculations.
Calculations accounting for LTC status and also properly adjusting for comorbidities and their severity may also lead to much lower estimates than some other increasingly used approaches such as the Global Burden of Disease Reference Life Table12 - also known as Theoretical Minimum Risk Life Table. This life table is an “aspirational” construct: it assumes an idealized situation with very low risk of death. According to this table, life expectancy is 88.9 years at birth, 9.99 years at age 85, 5.92 years at age 90, and 5.92 years at age 95.13 Using this popular aspirational life table would probably overestimate by 5-10-fold the years-of-life-lost for SARS-CoV-2-deceased residents in LTC facilities. Aspirational life tables have been promoted as a way to standardize burden of disease calculations across different countries. However, in the case of diseases like COVID-19 they could lead to grossly misleading inferences.
Estimates of survival in residents of LTC facilities preceding the COVID-19 pandemic also agree with very limited median survival of nursing home residents (e.g., 541 days in one study).14 However, we should acknowledge that there can be large heterogeneity. Some LTC facilities admit mostly residents with known limited life-expectancy (mostly for palliative care), while others may be institutions that admit mostly older adults who are quite healthy or have limited health problems with substantial life-expectancy.
Some caveats should be discussed. Our data pertain to fatalities during the first wave of COVID-19 and until the fall of 2020. The first wave was the most devastating in most high-income countries, with a few exceptions (e.g. Australia).15,16 The relatively lower proportion of fatalities in LTC residents in subsequent waves may reflect a combination of multiple factors: high levels of prior infection (seroprevalence studies have found 5-10 times higher infection rates in LTC facilities than in the general population in the first wave),17-19 better protection of nursing homes, more extensive testing, widespread use of vaccination in 2021,16 and the possibility that the sickest individuals were the first to succumb.20 Moreover, the significantly lower risk of death after the first month post-infection versus the uninfected controls should not be interpreted as a sign that SARS-CoV-2 infection causally decreases the risk of death during long-term follow-up, as it probably reflects mostly a selection process (residents who died in the first month were probably more sick and debilitated before infection, while those surviving probably had better life expectancy).
Allowing for these caveats, the major strength of our study is that it uses on large databases with nationwide coverage. Even so, similar analyses should also be performed in other countries because the health status of LTC residents may be different. This will allow to obtain more solid evidence on both the years-of-life-lost from the major COVID-19 pandemic, as well as insights about the long-term outcomes of SARS-CoV-2-infected residents of various types of LTC facilities who survived and recovered from the acute infection.
Data Availability
The data files used for the present study is publicly unavailable according to regulations under Swedish law, but can be applied for at each of the respective registry holders.
Footnotes
Funding: The authors received funding used for salaries from Foundation Stockholms Sjukhem (MK), Academy of Finland (MK), Läkarsällskapet (MK), and the Swedish Research Council (MK, AN, PN). The funders had no role in any part of this manuscript or the decision to publish.
Conflicts of interest: The authors declare no conflicts of interest.



