
ABSTRACT
Legalization of recreational cannabis in Ontario included the legalization of flower and herbs (Phase 1, October 2018), and was followed by the deregulation of cannabis retailers and sales of edibles (Phase 2, February 2020). Research on the impact of cannabis legalization on acute care utilization is nascet; no research has investigated potential age, gender, and geographically vulnerable subgroup effects. Residents living in Northern Ontario not only have higher levels of substance use problems, but also have inadequate access to primary healthcare. Our study investigated the impact of Ontario’s recreational cannabis policy (including Phase 1 and 2) on cannabis-attributable emergency department (ED) visits, and estimated the impact separately for different age and gender groups, with additional analyses focused on Northern Ontarians. We created a cohort of adults (18 and over) eligible for provincial universal health insurance with continuous coverage from 2015-2021 (n=14,900,820). An interrupted time-series was used to examine the immediate impact and month-to-month changes in cannabis-related ED visits associated with Phase 1 & 2 for each subgroup. While Northern Ontario has higher rates of cannabis-related ED visits, both Northern and Southern Ontario show similar patterns of changes. Phase 1 was associated with significant increases in adults 25-64, with the strongest increases seen in women 45-64. Month-to-month trends were flattened in most groups compared to pre-legalisation. Phase 2 was associated with significant immediate increases for adults aged 18-44 in both genders, but the increases were larger in women than men. No significant month-to-month changes were detected in this period. While current preventive efforts are largely focused on reducing cannabis-related harms in youths and younger adults, our results show that adults 25-64, particularly women, have been significantly impacted by cannabis policies. Further research on gender-specific cannabis dosage and targeted interventions for adult women should be investigated. Legalization did not appear to have a differential impact on Northern versus Southern Ontario, but higher rates of ED visits in the North should be addressed.
INTRODUCTION
On October 17th, 2018, the federal Canadian government, through the Cannabis Act 2018, legalized the possession, consumption, and sales of cannabis for recreational use for adults. Subsequently, each province implemented their own regulations governing access and use. In Ontario, Canada’s most populated province with 38.8% of the entire Canadian population, a two-phased approach was taken for the sales and distribution of cannabis products. During Phase 1 (October 18, 2018-March 17, 2020), flowers and herbs were the only available product and could be exclusively purchased from the government-run website and 67 retail storefronts (licensed through a lottery) (1). In Phase 2 (March 18, 2020-June 17, 2021), cannabis edibles became legalized and widely available, and the cap on the number of retailers was lifted, and by June 2021, there were 826 stores (2).
Although prior research has shown that cannabis may be associated with fewer acute harm events compared to tobacco, alcohol, and opiates(3), problematic use can lead to anxiety, paranoia, suicidal ideation, cognitive impairment, induce temporary tachycardia and cannabinoid hyperemesis syndrome(4), or lead to cyclical emesis with chronic use(5). While emerging evidence suggests that legalization has led to modest increases in cannabis-attributable emergency department (ED) visits(6–9), these studies have a number of limitations. First, these studies focus only on the general population or the pediatric population, which ignores the differential impact of legalization across gender and lifecourse(10). This information is necessary for the development of age- and gender-specific interventions. Second, there has been no research that looks at the impacts of legalization on cannabis-related ED visits in Northern Ontario. Northern Canada experiences low physician retention(11), a lack of comprehensive service availability, and a historical vulnerability to substance use problems(12). In Ontario, Northern residents have double the rate of substance-related healthcare encounters compared to the rest of the province (911.6 per 100,000 vs. 457.2 per 100,000)(13), which underscores the importance of research on the impact of cannabis legalization on this underserved population. Our study will address these distinct gaps in the literature using disaggregated analyses of population-level health administrative data in Ontario.
We aim to investigate the impact of recreational cannabis policy (including Phase 1 and 2) on cannabis-attributable ED visits, and estimate the impact separately for different age and gender groups, with additional analyses focused on Northern Ontarians.
Materials and Methods
Data source
The study cohort (n=14,900,820) was created using health-administrative data held at ICES (formerly the Institute for Clinical Evaluative Sciences), based on all Ontarians (contained in the Registered Person Database) eligible for the Ontario Health Insurance Plan (OHIP) as of October 17, 2015, with healthcare records followed through until June 17, 2021. To be included in the cohort, individuals must have continuous OHIP coverage and residency in Ontario for the entire study period. Age groups for our study were based on each person’s age on the day of Canada’s cannabis legalization. Northern Ontario, based on Statistics Canada’s health regions(14), was defined as the area of the province that is north of the French River and Algonquin Park. The Registered Person Database provides gender identity(15); however, gender may be mismatched if not officially changed.
This study complied with privacy regulations of the Institute for Clinical and Evaluative Science (ICES). To protect privacy, all cell sizes fewer than six individuals were suppressed and reported as n < 6. Consent was not obtained for participants for the use of their data in this study. ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data used for the study, without consent, for health system evaluation and improvement. All patient information was anonymized and de-identified prior to analysis. Ethics approval for this study was obtained through Brock University (REB# 20-134-CHUM).
Outcomes
The outcomes of interest were monthly cannabis-attributable ED visits from October 2015 to May 2021 in Ontario (i.e. the frequency of the event within age, gender, and region-specific subgroups for each month of the study period). Using the National Ambulatory Care Reporting System, Discharge Abstract Database, and Ontario Mental Health Reporting System, records were included with at least one of the following ICD-10 codes for either the primary or supplemental diagnosis: F12 (cannabis-related disorders) and T40.7 (cannabis poisoning), following the conventions from prior studies(6,7,16).
Intervention
Our study considers three distinct time periods related to cannabis policy in Ontario, including 1) the pre-legalization period (October 2015-October 2018), 2) Phase 1 of legalization (October 2018-February 2020) which marked the beginning of online flower and herb sales alongside limited physical retail locations, and 3) Phase 2 (March 2020-June 2021) saw the removal of the retail cap and increased edible cannabis availability. These cutoff dates were used in a prior study estimating the impact of legalization and commercialization on cannabis-related ED visits in the Ontario population(9). Following recommendations from the prior study, healthcare visits in March and April 2020 were censored to account for large decreases in health-seeking behaviors (including ED visits) associated with the early stages of COVID-19 pandemic.
Statistical analyses
We used an interrupted time-series with single-group, multiple-interventions design to examine the immediate and month-to-month changes associated with cannabis-related policies on cannabis-related ED visits for each age and gender group in Ontario (both North and South), Southern, and Northern Ontario. We conducted segmented regressions using the negative binomial function to estimate the incidence rate ratio while adjusting for overdispersion (i.e. extra-Poisson variation). We estimated models for each age group (18 to 24, 25 to 44, 45 to 64, and 65+) and gender separately, given prior research finding age and gender differences in the patterns of cannabis use(17). We adjusted for the length of the month and for any seasonal effect(18). We conducted two sensitivity analyses. First, to examine whether the results were robust regardless of the functional form and address possible residual autocorrelation in a time-series dataset, the Prais-Winsten regressions following a first-order autoregressive process were performed(19). Second, we included the months March and April 2020 in an alternative specification of the models, and used an indicator variable for both months as an adjustment to confirm whether the estimates were robust.
RESULTS
Table 1 shows the number of individuals with 1 or more cannabis-related ED visits in the entire study period (October 18, 2015-June 17, 2021) across age, gender, and for Northern, Southern, and the entirety of Ontario. In general, men, those in the 18-24 age group, and those living in Northern Ontario are at a higher risk of cannabis-related ED visits. Table 2 shows the gender- and age-specific average monthly rates (per 100,000 people) of cannabis-related ED visits in the pre-legalization period, Phase 1, and Phase 2. Rates for cannabis-related ED visits appear to increase for age groups under 65 after both Phase 1 and Phase 2.
In Southern Ontario (Table 3), there was an increasing trend in cannabis-related ED visits across all gender and age groups during the pre-legalization period: at the lowest end, an increase of 1.6% ED visits per month among women aged 18-24 (IRR = 1.016, 95% CI 1.013-1.020), and at the highest end, an increase of 7.3% ED visits per month among boys aged 0-17 (IRR = 1.073, 95% CI 1.064-1.082). Legalization (Phase 1) was associated with an immediate (level) increase overall, and they were statistically significant in 3 groups: 1) a 20% increase in ED visits among men aged 45-64 (IRR = 1.207, 95% CI 1.015-1.436), 2) a 13% increase among women aged 25-44 (IRR = 1.134, 95% CI 1.000-1.286), and 3) a 29% increase among women aged 45-64 (IRR = 1.289, 95% CI 1.020-1.628). In Phase 1, there were no significant month-to-month (trend) increases in ED visits across all gender and age groups.
Associations between cannabis policies and ED visits in Southern Ontario using negative binomial regression with censored months in the early stages of COVID-19 pandemic
In Southern Ontario during Phase 2, immediate (level) increases in ED visits were observed among 4 groups: 1) a 36% increase among men aged 18-24 (IRR: 1.363, 95% CI 1.193-1.557), 2) a 26% increase in men aged 25-44 (IRR: 1.222, 95% CI 1.074-1.472), 3) a 50% increase in women aged 18-24 (IRR: 1.499, 95% CI 1.252-1.794), and 4) a 42% increase in women aged 25-44 (IRR: 1.421, 95% CI 1.196-1.688). Finally, in Phase 2, month-to-month (trend) increases had stabilized in all age and gender groups, with a decreasing monthly trend of 1.3% per month among men aged 18-24 (IRR: 0.986, 95% CI 0.973-0.999).
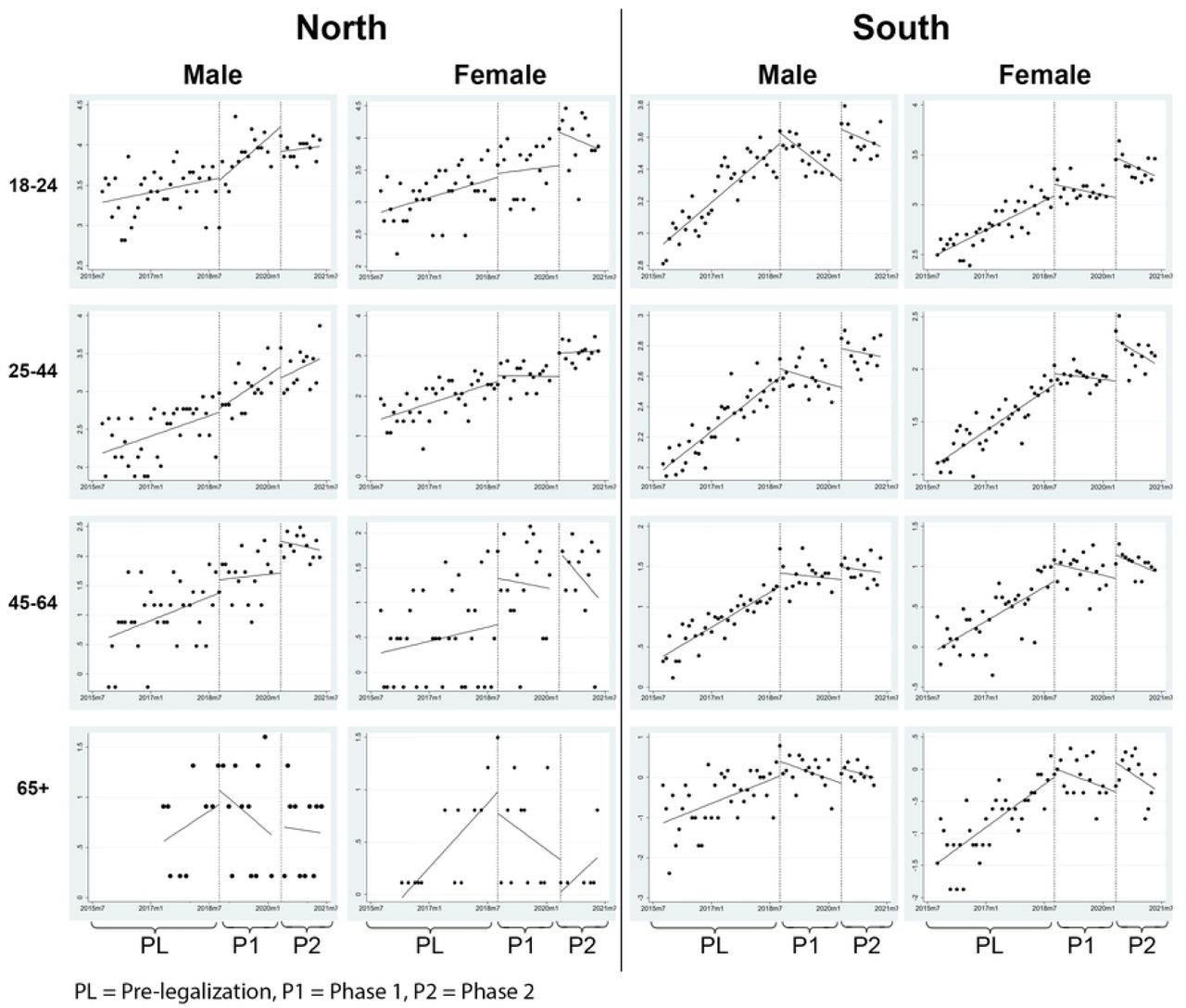
The pre-legalisation trend and immediate effect of Phase 1 observed in Northern Ontario (Table 4) were similar in magnitude compared to Southern Ontario. For instance, almost all age and gender groups had significant month-to-month increases in ED visits in the pre-legalization period, and there were immediate insignificant increases for most demographic groups, but only significant among women aged 45-64 (IRR: 2.004, 95% CI 1.017-3.949). In Phase 2, while many demographic groups had immediate increases in ED visits in Southern Ontario, fewer groups observed immediate increases in Northern Ontario (only women aged 25-44 had a statistically significant increase of 75%, IRR 1.747, 95% CI 1.084-2.814). In Phase 2 (i.e. the edibles period), similar to Southern Ontario, the month-to-month increase in ED visits also stabilized in Northern Ontario. Table 5 provides the estimates for the entirety of Ontario (i.e. pooling Northern and Southern Ontario): these results are substantially similar to Southern Ontario given that its residents account for 94.3% of the entire province’s population. Figure 1 visualizes the change in monthly cannabis-related ED visits by each subgroup.
Associations between cannabis policies and ED visits in Northern Ontario using negative binomial regression with censored months in the early stages of COVID-19 pandemic
Associations between cannabis policies and ED visits in all of Ontario using negative binomial regression with censored months in the early stages of COVID-19 pandemic

{kind=link}
Discussion
Cannabis legalization was associated with immediate increases in ED visits of adults in Ontario. Phase 1 was associated with significant immediate increases in adults 25-64, and Phase 2 was associated with immediate increases in those 18-44, with greater increases observed in women for both phases. Among these groups, the pattern is characterized by rapid immediate increase, but no significant subsequent trend (month-to-month) change is observed. Also, while Northern Ontario has higher rates of cannabis-related ED visits, both Northern and Southern Ontario show relatively similar patterns of changes with regards to Phase 1 and 2 of legalization.
Our results are largely consistent with findings from prior research that found cannabis legalization (Phase 1) (6) and cannabis edibles legalization and commercialization (Phase 2) were associated with increases in cannabis-related ED visits in Canadian provinces (8,9). For example, a study reported that cannabis legalization (Phase 1) led to a small immediate increase in urban-Alberta cannabis-related ED visits; however, this study included a relatively short period (less than 1 year) and did not adjust for temporal autocorrelation and seasonality(6). Our results also support the findings of an Ontario study which suggest that the immediate effects of cannabis legalization (Phase 1) were largely driven by adults over the age of 24(9). Additionally, similar to other studies that examined the Phase 2 effect (i.e. edibles and commercialization), we found evidence of an immediate increase in cannabis-related ED visits; however, no studies including ours have been able to isolate the Phase 2 effect from the COVID-19 effects that coincided with Phase 2. Only one study from Hamilton, Ontario contradicted our results: they found that there was no change in the rate of cannabis-related ED visits following legalization(20), but the authors only examined a single hospital, and did not measure level and trend changes.
Our study is the first to conduct age- and gender-specific analyses on legalization and cannabis-related ED visits in Canada. Since prior studies did not include age and gender stratifications, they were unable to identify whether the effects were consistent across age and gender groups, and whether the apparent effects may be driven by a specific subgroup. Our study also makes unique contributions to the study of Northern Ontario. While our study finds consistently higher rates of cannabis-related ED visits in Northern Ontario compared to the rest of the province (consistent with studies of substance-related healthcare visits in the North prior to cannabis legalization(13)), we note that ED visits in the North and South were similarly affected by Phase 1 and Phase 2.
Limitations of this study include: 1) the use of single-group interrupted time series is vulnerable to concurrent interventions, policies or events that may confound the relationship between cannabis legalization and cannabis-related ED visits. While we have adjusted for the early COVID-19 effects on ED visits, there may be other unforeseen events that impact people’s willingness to visit the ED. 2) Phase 2 of the study overlapped with the COVID-19 pandemic, so we cannot confidently estimate the independent effects associated with commercialization and edibles. 3) Our study relies on administrative health records to indicate whether individuals have continuous OHIP coverage and residency in Ontario, but some individuals may not be in Ontario for the full study period (e.g. traveling while still maintaining OHIP coverage). 4) The reporting of cannabis-related ED visits may have changed over time, especially given that patients may feel less stigmatized reporting cannabis use at the ED after legalization, which may bias our results towards a significant finding for Phase 1 effects; however, prior literature on cannabis-related ED visits uses the same methods for identifying outcomes(21).
Future studies could take a different approach to isolate the edibles/commercialization effects on cannabis-related ED visits. Such a study can include a control region that is contextually similar (e.g., comparison with a US state that was similarly impacted by COVID-19, but did not implement cannabis legalization) so that we can isolate the Phase 2 effects. Further research should be conducted on the impact of cannabis legalization on the cannabis-related ED visits and hospitalizations in specific patient and at-risk groups (e.g., people with depression, anxiety, or schizophrenia).
Conclusion
Our study provides evidence that the rate of increase in cannabis-related ED visits in Ontario has flattened even in the face of cannabis legalization and deregulation of retailers/edibles. Furthermore, the association between cannabis legalization and cannabis-related ED visits varies across age, gender, and geography (i.e., Northern vs Southern Ontario). Of note, cannabis-related ED visits in adults aged 18-44 in both genders in the South and women aged 25-44 in the North were significantly increased during Phase 2; however, it is unknown how much COVID-19 contributed to these changes. While legalization (Phase 1 and 2) did not differentially impact the North (vs the South), cannabis-related ED visits remain high and should be addressed in this region. While current preventive efforts are largely focused on reducing cannabis-related harms in youths and in school settings (22), our results show that adults 25-64, particularly women, have been significantly impacted by cannabis policies. Further research on gender-specific cannabis dosage and targeted interventions for adults should be investigated. Legalization did not appear to have a differential impact on Northern versus Southern Ontario, but higher rates of ED visits in the North should be addressed.
Data Availability
The dataset from this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre- specified criteria for confidential access, available at www.ices.on.ca/DAS. The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Data partner acknowledgements
Parts of this material are based on data and information compiled and provided by CIHI. However, the analyses, conclusions,opinions, and statements expressed herein are those of the author, and not necessarily those of CIHI.
Data availability statement
The dataset from this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS. The full dataset creation plan and underlying analytics code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Contributions
Chungah Kim and Antony Chum co-wrote the first draft of the study. Chungah Kim analyzed the data. Chungah Kim, Antony Chum, and Sara Allin contributed to the interpretation of the data. Antony Chum, Chungah Kim, and Andrew Nielsen co-wrote the dataset creation plan. Antony Chum conceived of the initial project and provided funding and oversight of the study. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Acknowledgement
This study contracted ICES Data & Analytic Services (DAS) and used de-identified data from the ICES Data Repository, which is managed by ICES with support from its funders and partners: Canada’s Strategy for Patient-Oriented Research (SPOR), the Ontario SPOR Support Unit, the Canadian Institutes of Health Research and the Government of Ontario. The opinions, results and conclusions reported are those of the authors. No endorsement by ICES or any of its funders or partners is intended or should be inferred.
Footnotes
Funding Funding for the study was provided by Canadian Institutes of Health Research (Project Grant FRN# 173447, NPI: Antony Chum). The funding agencies had no role in the design and conduct of the study; the collection, management, analysis or interpretation of the data; the preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication.
Competing interests None declared.



