
Abstract
Objectives To assess the effectiveness of respiratory interventions and case isolation measures in reducing or preventing the transmission of mpox in humans and to inform future focused reviews on mpox transmission.
Methods The WHO Clinical Management and Infection Prevention and Control guideline 2022 development group developed three structured research questions concerning respiratory and isolation infection prevention control measures for mpox. We conducted a systematic review that included a broad search of five electronic databases. In a two-stage process, we initially sought only randomized controlled trials and observational comparative studies; when the search failed to yield eligible studies, the subsequent search included all study designs including clinical and environmental sampling studies.
Results To inform the questions the review team synthesized route of transmission data in mpox. There were 2420/3924 (61.7%) cases in which investigators identified transmission occurring through direct physical sexual contact. There proved to be no reported mpox cases in which investigators identified inhalation as a single route of transmission. There were 2/3924 (0.05%) cases in which investigators identified fomite as a single route of transmission. Clinical and environmental sampling studies generally failed to isolate mpox virus in saliva, oropharangeal swabs, mpox skin lesions, and hospital room air.
Conclusions Current findings provide compelling evidence that transmission of mpox occurs through direct physical contact. Because investigators have not reported any cases of transmission via inhalation alone the impact of respiratory infection prevention control measures in reducing transmission will be minimal. Avoiding physical contact with others, covering mpox lesions and wearing a medical mask is likely to reduce onward mpox transmission; there may be minimal reduction in transmission from additionally physically isolating patients.
Introduction
Mpox is a zoonotic disease caused by mpox virus, an enveloped double-stranded DNA virus in the Orthopoxvirus genus of the Poxviridae family. The World Health Organization (WHO) declared mpox (then termed monkeypox) a Public Health Emergency of International Concern (PHEIC) on July 23rd, 2022. The 2022 mpox outbreak was associated with sustained human-to-human transmission that had not been previously described; historically mpox occurred primarily in west and central Africa, with infection commonly reported in persons who had contact with probable animal reservoirs with cases of secondary transmission reported in household contacts. Incidence in endemic areas of central and West Africa had been increasing rapidly over the past decades, coinciding with cessation of smallpox vaccination and eradication programmes.
Mpox incubates between five to 21 days and typically presents symptoms in two stages: the invasion period lasting from zero to five days characterized by fever, headache, lymphadenopathy, back pain, myalgia, and asthenia; following this, skin symptoms may appear between one to three days from onset of fever, with a rash evolving from macules to papules, vesicles, pustules and then crusts, often affecting the face, extremities, oral mucous membranes and genitalia.
The effectiveness of any infection prevention and control measures for mpox will depend on route(s) of transmission. Suspected or confirmed transmission routes include direct physical contact with an infected patient (non-sexual physical contact or sexual physical contact), indirect contact (fomite transmission) inhalation of fomites or infectious droplets and transplacental transmission. Human infection is also possible from contact with infected animals (scratches, bites, preparing, eating or using infected meat and animal products). Areas of uncertainty exist concerning the potential for asymptomatic transmission or the transmission potential of other possible routes, such as breastmilk, semen, vaginal fluids, urine, faeces or insect vectors.
There is a need for effective interventions to prevent the transmission of mpox. The WHO Clinical Management and Infection Prevention and Control 2022 guideline development group developed two research questions concerning airborne and respiratory infection prevention and control interventions and one question concerning case physical isolation interventions in mpox. It was expected that scarce evidence, if any, from randomized controlled trials or comparative interventional trials to inform the research questions would exist. As such, it was anticipated that the review questions would be informed indirectly using data on the number of incident cases of mpox by route of transmission and clinical and environmental sampling studies demonstrating viral culture positivity. This is based on the inference that, if there are a significant number of cases transmitted by inhalation or fomites and/or strong viral culture positivity from samples representative of these routes of transmission, interventions directed at preventing transmission via these route(s) would be of importance. Therefore, we conducted a systematic review to provide evidence for guideline recommendations regarding use of respiratory barriers to mpox transmission and physical isolation of mpox patients.
Objective
To assess the effectiveness of respiratory and case isolation infection precaution measures in reducing or preventing the transmission of mpox in humans.
Methods
1. Interventions for preventing transmission of mpox virus
The review research questions developed by WHO Clinical Management and Infection Prevention and Control 2022 guideline development group for this review were:
To provide direct evidence on these review questions, in collaboration with members of the WHO Clinical Management and Infection Prevention and Control 2022 guideline development, the author team developed a protocol and then undertook this systematic review process using the following methods:
Inclusion Criteria
Population
Humans with laboratory confirmed mpox infection; or
humans with laboratory confirmed mpox-like infection; or
humans with exposure to a laboratory confirmed mpox infection or mpox-like infection.
Mpox-like infection is defined for the purposes of the review as infection due to orthopox viruses other than mpox that are capable of human-to-human transmission, namely buffalopox, cowpox, vaccinia and variola.
Types of interventions
Respiratory precautions including medical masks or use of respirators.
Personal contact precautions including use of gloves, gowns, eye protection.
Isolation of cases
Ventilation including natural, mechanical, negative pressure gradient, positive pressure ventilated lobby.
The administration of any type of vaccine to health care workers or contacts of mpox or mpox-like virus confirmed patients was not to be considered as an intervention type.
Control
No intervention or;
Any different intervention measure used as a comparator to the intervention group in the study.
Outcomes
Confirmed secondary mpox or mpox-like virus infection expressed as an absolute number or rate of secondary transmission.
All reported adverse effects related to the interventions.
Settings
All countries and the following contexts were eligible for this review: households, congregate-living, community and healthcare settings.
Types of studies
RCTs, controlled before-and-after studies, observational comparative studies in participants with confirmed mpox or exposed to mpox virus.
RCTs or observational comparative studies in participants with exposure to or confirmed mpox-like virus infection.
Exclusion Criteria
Studies published in a language other than English.
Studies of designs other than RCTs, controlled before-and-after studies, or observational comparative studies for participants with confirmed mpox infection or exposure to mpox.
Studies of designs other than RCTs or observational comparative studies in participants with viruses other than viruses defined as mpox-like viruses.
Studies that do not include a review question-specific intervention to reduce or prevent the transmission of mpox or mpox-like viruses.
Studies conducted in animals.
Literature Search Strategy
Using broad search terms including terms for mpox-like viruses and without date or language limits, the search in September 2022 included the following databases: Medline (OVID), Embase (OVID), Biosis previews (Web of Science), CAB Abstracts (Web of science), and Global Index Medicus (Appendix 1). The author team instituted a call to topic experts for papers concerning the review questions for relevant studies up to 15th December 2022.
Selection of Studies
The team uploaded the results of the literature searches into Distiller SR (DistillerSR 2021) and multiple authors independently undertook screening of title and abstract literature search results according to the Cochrane Collaboration’s Rapid Review Methods (Garritty 2020). One author assessed a study as eligible for full text screening; two authors assessed a study as requiring exclusion. Multiple authors independently undertook full text screening according to review inclusion criteria. One author assessed a study as eligible for inclusion for data extraction; two reviewers assessed a study for exclusion. Authors resolved disagreement at any stage by discussion.
2. Transmission of mpox virus
A second review protocol had been prospectively written and confirmed with members of the WHO Clinical Management and Infection Prevention and Control guideline development group in the event of no randomized controlled trials or comparative observational studies being identified in the first review (see methods section 1 ‘Interventions for preventing transmission of mpox virus’ above).
This second review aimed to identify and synthesize evidence on transmission that could indirectly inform the research questions by answering the following:
What is the proportion of new incident cases of mpox disaggregated by route of transmission?
What is the infectious period of mpox, disaggregated by route of transmission? The infectious period is defined as the number of days since the onset of symptoms.
Inclusion criteria
Population
Human participant of any age with laboratory confirmed mpox infection or exposure of a human to a laboratory-confirmed mpox patient or exposure to a suspected human mpox case.
The WHO definition of a suspected case of mpox infection was used (WHO 2022).
Laboratory confirmed infection was defined as reverse-transcriptase polymerase chain reaction (RT-PCR) positive or viral culture positive.
Outcomes
1. Mpox infection
Type of study
any scientific article of any design including clinical and environmental sampling studies.
Setting
All countries and all contexts.
Exclusion criteria
Studies not including a human case of laboratory confirmed mpox infection or exposure to a laboratory-confirmed mpox patient or exposure to a suspected mpox case.
Studies concerning animal-to-animal mpox transmission or animal-to-human transmission.
Studies not published in English.
Experimental laboratory transmission studies.
Studies meeting the inclusion criteria but not otherwise containing information relevant to the review questions.
Literature Search strategy
The review team used the same search strategy as for methods section 1 ‘Interventions for reducing the risk of transmission of mpox virus’ (above).
Selection of studies
The results of the literature searches were uploaded into Distiller SR (DistillerSR 2021). Screening of results was undertaken according to the Cochrane Collaboration’s Rapid Review Methods (Garritty 2020). Title and abstract screening of all studies identified in the literature searches was undertaken independently by multiple authors; one author was required to assess a study as eligible for full text screening; two authors were required to assess a study as requiring exclusion. Full text screening against the review inclusion criteria was undertaken independently by multiple authors. One author was required to assess a study as eligible for inclusion to data extraction; two reviewers were required to assess a study for exclusion. Authors resolved disagreement at any stage by discussion.
Data extraction and management
Two authors extracted data from all included studies using a pre-piloted data extraction form within Distiller SR. One author extracted all relevant data and the second author cross-checked all extracted data. Data was extracted concerning characteristics of the study participants including number of primary and/or secondary cases, country, year of study, setting of transmission (such as household, healthcare), clade of mpox, reported nature of contact of participants to a potential or confirmed course of mpox, study author reported modes or potential modes of transmission, and data concerning clinical or environmental sampling including sample type, and day of sample PCR or viral culture positivity from symptom onset.
Risk of bias assessment
No risk of bias assessment was undertaken; no randomized controlled trials or observational comparative studies had been identified.
Data synthesis
What is the proportion of new incident cases of mpox disaggregated by route of transmission?
Two authors independently categorized reported human mpox cases from identified studies by route(s) of transmission. Authors resolved disagreement at any stage by discussion. Authors assigned the following route(s) of transmission to each case as applicable: direct sexual physical contact, direct non-sexual physical contact, fomite, inhalation, transplacental, needlestick, ingestion or unknown.
The routes of transmission are defined as:
Direct sexual physical contact: transmission occurring in the context of any type of sexual activity, including oral sex, penetrative anal or vaginal sex (insertive and receptive), or hand-to-genital contact.
Direct non-sexual physical contact: direct physical touch with the exclusion of any sexual physical as defined above.
Fomite: indirect contact transmission involving contact of a susceptible host with a contaminated object or surface.
Inhalation: occurs when infectious particles, of any size, travel through the air, enter and are deposited at any point within the respiratory tract of a (susceptible) person. This form of transmission can occur when the infectious particles have travelled either a short-or long-range from the infected person.
Transplacental: transmission via the placenta from mother to foetus.
Percutaneous injury: transmission via percutaneous injury with a contaminated object, such as a needle.
The review team then categorised all cases into one of three categories: (i) single route of transmission reasonably identified, (ii) multiple routes of transmission possible, and (iii) unknown. The category of a single route of transmission applied when sufficient data concerning the case history, epidemiology and/or clinical details was reported to reasonably judge that a single route of transmission had occurred. The category of multiple possible routes of transmission applied when more than one route of transmission was judged as reasonably possible based on reported information. Authors applied the category of unknown when there was insufficient information reported in the study to assign or hypothesize any route of transmission.
The number of cases for each route and category of transmission is reported as a whole number and percentage of the total. Data are presented for each route of transmission category, by mpox clade, and by route of transmission in the healthcare and household settings. Data that could inform the subgroups within the research questions is summarized.
2. What is the infectious period of mpox, disaggregated by route of transmission?
Authors separated data from included studies into either human mpox clinical samples or environmental samples from an environment occupied by an mpox case. The review team assigned data concerning environmental air sampling, mask sampling, and upper respiratory tract clinical sampling to the review questions concerning prevention of airborne transmission. Data concerning environmental surface sampling and clinical sampling of active skin lesions were assigned to the review question concerning case isolation measures.
Within these categories the review team identified and summarized longitudinal studies and summarized cross-sectional studies that attempted viral isolation. The number of samples for each category is presented. Data that could inform the subgroups within the review questions is summarized.
Results
Search Results
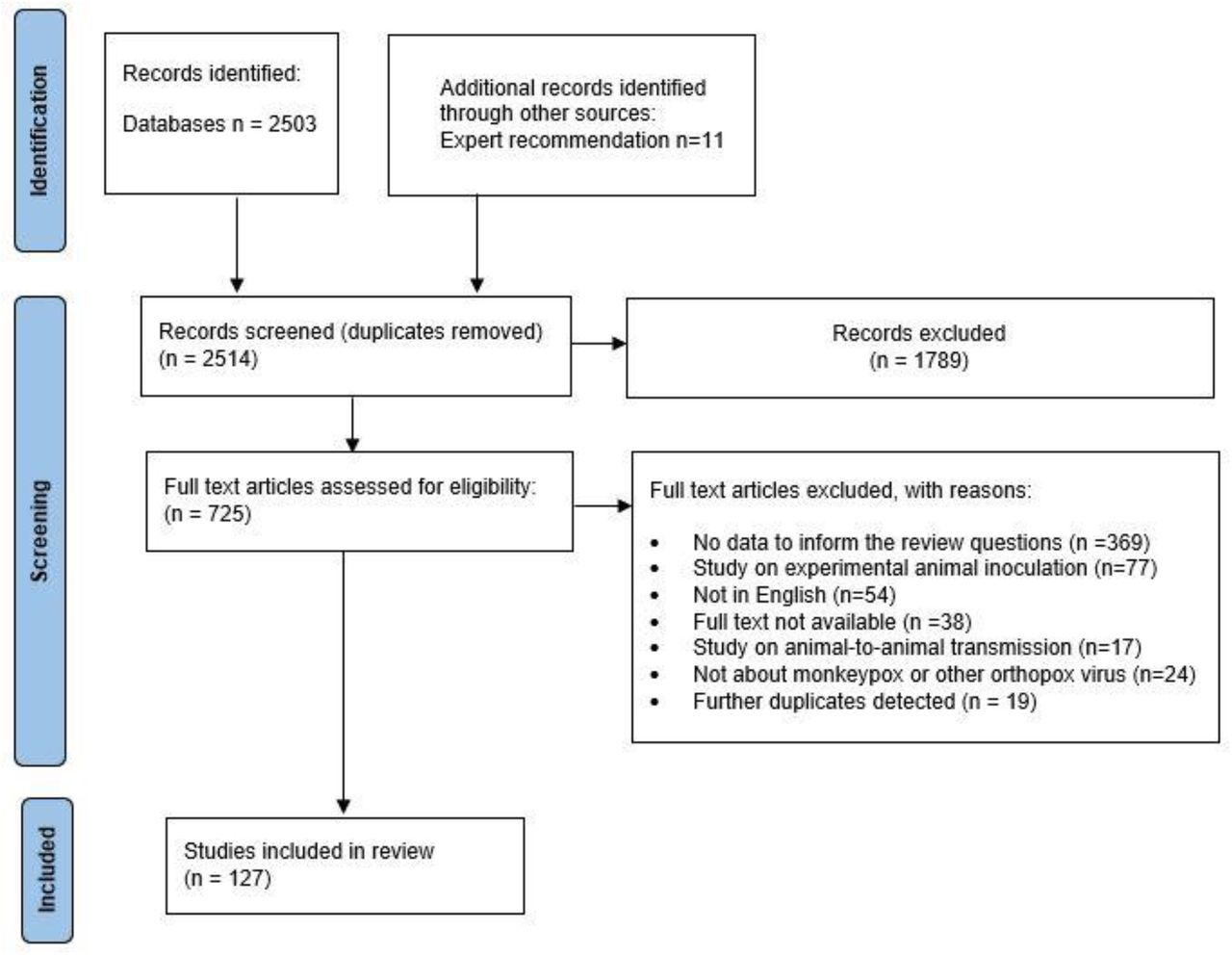
The searches identified 2514 unique records. Authors assessed the full text of 725 studies; 127 studies were included and 598 studies were excluded. The study selection process is seen in Appendix 2.
Included studies
No randomized controlled trials or observational comparative studies were identified that directly informed any of the IPC review questions. No studies concerning mpox-like viruses met the inclusion criteria.
119 studies reported cases of human-to-human mpox transmission. 35 studies were published prior to the 2022 outbreak, and 84 studies were published during 2022. Of the included studies, 46 studies concerned cases acquired from Africa, 42 studies from Europe, 16 studies from the USA, 5 studies from the United Kingdom, 3 studies from Brazil, 1 study from Canada and 6 studies did not report the country of acquisition of infection.
Included cases
There were 3924 cases of human-to-human transmission. Typical cases were males over the age of 18 years; it was not possible to disaggregate age and gender for 35% of cases (Table 1).
Characteristics of reported cases
Results: Review Question 1 and 2
Review questions 1 and 2 are considered together as they both concern respiratory infection prevention control interventions.
Number of incident cases by route of transmission
Where they could identify a single route of human-to-human transmission, investigators reported no cases in which inhalation could have been the exclusive mode of mpox virus transmission (Table 2).
Incident cases of mpox by route of transmission
What is the proportion of new incident cases of mpox, by route of transmission
Population: Adults and children with confirmed mpox
Setting: All settings
Transmission: A single route of transmission was identified
Table 3 displays the clade of mpox by route of transmission in cases where a single route of transmission could be identified. Studies not reporting on clade have been split into those published in 2022 (likely to be clade IIb) and those published prior to 2022 (less likely to be clade IIb).
What is the proportion of new incident cases of mpox, by route of transmission for each clade of mpox?
Population: Adults and children with confirmed mpox
Setting: All settings
Transmission: A single route of transmission was identified
For transmission reported within a healthcare setting, investigators considered 117/120 (97.5%) cases to either be transmitted through physical touch (non-sexual), fomite or inhalation, and 3/120 (2.5%) to be either transmitted through fomite or inhalation (Table 4). Due to limited information reported by study authors, the review team was unable to disaggregate further.
Proportion of new incident cases of mpox by route of transmission in the healthcare setting?
Population: Adults and children with confirmed mpox
Setting: Healthcare
Transmission: More than one route of transmission was identified as possible by authors. Possible routes: direct physical non- sexual contact, fomite, inhalation.
There were 808 cases that authors reported to have occurred within a household setting; however, due to limited reported information, no further disaggregation by route of transmission proved possible (Table 5). Authors reported possible routes of human-to-human transmission as inhalation, fomite, direct sexual physical contact and direct physical non-sexual contact.
Proportion of new incident cases of mpox by route of transmission in the household setting
Population: Adults and children with confirmed mpox
Setting: Household
Transmission: More than one route of transmission was identified as possible by authors.
Clinical and environmental sampling
Two studies (Hernaez 2022, Mileto 2022) attempted viral isolation from respiratory tract samples; mpox virus was isolated from saliva in 22/33 (66.7%) of samples between days 3 and 9 from symptom onset and in 1/4 (25%) oropharyngeal samples taken on day 9 from symptom onset (Table 6).
Clinical samples of viral isolation attempts from adults or children with confirmed mpox infection
Authors identified two studies in which viral isolation was attempted from air samples collected in rooms occupied by an individual with mpox (Hernaez 2022, Gould 2022); replication competent virus was identified in one air sample collected in a hospital room (Table 7).
Air sampling in environments occupied by adults with confirmed mpox infection
Subgroups
Health care worker transmission
Health care workers were the population of interest in review questions 1 and 2.
A health care worker in the United Kingdom in 2018 was diagnosed with mpox after changing the bed linen of a confirmed mpox patient using an apron and gloves; there was no direct contact with the mpox patient (Vaughan 2018). Investigators judged that transmission was possible either by fomite or inhalational route.
Three studies reported mpox infection in a healthcare worker through percutaneous injury with a contaminated sharp object that had been in contact with an mpox lesion (Caldas 2022, Carvalho 2022, Mendoza 2022).
Patient-to-patient transmission
An outcome in review question 2 concerned the risk of transmission to patients. Two studies were identified that provided relevant data (Jezek 1986, Learned 2003). Jezek 1986 reported mpox in a child in the Democratic Republic of the Congo who had visited a hospital several times where another child with confirmed mpox had been admitted; there was no known physical contact between the two. Authors hypothesized fomite or inhalation transmission. Learned 2003 reported a case of mpox in a patient during a hospital stay for malaria and in the same hospital as patients with mpox; authors reported no further information.
Results: Review Question 3
Review question 3 concerned IPC interventions related to the physical isolation of patients with active lesions.
Incident cases by route of transmission
In situations in which investigators could identify a single route of human-to-human transmission, 2420/3924 (61.7%) cases were transmitted via direct physical sexual contact, 36/3924 (0.09%) cases were transmitted via direct physical non-sexual contact, and 2/3924 (0.05%) cases via fomites (Table 2). The majority of data is from Clade IIb cases (Table 3).
The two cases transmitted via fomites occurred in health care workers who visited a patient’s home for one hour, wore PPE during the visit (N95 masks, eye protection, gowns), used gloves only when taking clinical samples from patients, and did not directly physically touch the patient (Salvato 2022).
Clinical and environmental samples
Eight studies reported attempts to isolate virus from lesion samples. In four studies reporting the date of clinical sampling from symptom onset, 8/10 (80%) of lesion samples contained replication competent virus (Table 8) (Lapa 2022, Learned 2005, Mileto 2022, Noe 2022). In four studies in which the day of sampling was not documented, virus isolation was reported in 46.7% of lesion samples (Table 8) (Breman 1980, Erez 2019, Hughes 2021, Rimoin 2007).
Mpox lesion clinical samples in which viral isolation was attempted
Five studies attempted viral isolation from environmental surface samples (Atkinson 2022, Morgan 2022, Norz 2022, Gould 2022, Pfeiffer 2022). The frequency of detection of replication competent virus was between 0 and 60% in surface samples (Table 9).
Surface Sampling in environments occupied by adults with confirmed mpox infection
Discussion
There is no evidence from randomized controlled trials or observational comparative studies concerning respiratory interventions or case physical isolation measures in mpox or mpox-like viruses capable of human-to-human transmission. Investigators reported zero cases of instances of respiratory (inhalation) transmission of mpox as a single route of transmission. Investigators reported 2 out of 3924 (0.05%) cases in which mpox virus could have reasonably been exclusively transmitted through fomites (Salvato 2022). In comparison, in 2420/3924 (61.7%) cases investigators identified transmission occurring through direct physical sexual contact.
Study investigators identified infectious mpox virus in saliva (Hernaez 2022) and oropharyngeal swabs (Mileto 2022), and identified competent virus in 1/28 (3.6%) air samples (Hernaez 2022, Gould 2022). Viral isolation was successful in 101/209 (48%) of lesion samples from 8 studies; surface sampling in domestic and healthcare environments in 5 studies detected viable mpox virus in 16.2% of samples (range 0-60%). The presence of infectious virus in clinical samples and environmental samples provides only very low certainty evidence regarding risk of transmission.
There is scarce data concerning transmission of mpox to health care workers. Transmission of mpox to healthcare workers was identified through percutaneous injury in three cases (Caldas 2022, Carvalho 2022, Mendoza 2022) and through possible fomite or inhalation in one case (Vaughan 2018).
Strengths and limitations
This review is strengthened by a comprehensive search strategy and authors independently assessed all studies for eligibility in duplicate to identify all possible relevant literature. Further, a clear conceptual data framework to address the research questions was undertaken; key data from all available literature that could inform the research questions was identified and synthesized.
This review is limited by the existing available evidence base on mpox. The review team utilized only broad search terms inclusive of terms for mpox-like viruses however no comparative interventional studies were identified. There is limited epidemiological evidence on the risk of fomite and inhalational transmission, and limited evidence on the infectious period for different routes of transmission.
To our knowledge there is no known prior systematic review investigating respiratory or case isolation infection prevention control for mpox or mpox-like viruses.
Implications for practice and research
The findings of this review provide compelling evidence that transmission of mpox occurs primarily through direct physical contact. Epidemiological evidence and data from clinical and environmental sampling does not support the hypothesis that respiratory or fomite modes of transmission are significant. The impact of respiratory infection prevention control measures in reducing transmission may be small. There is potential for shedding of infectious virus onto surfaces from lesions of detached scabs; covering mpox lesions is likely to reduce onward transmission however there is probably minimal reduction in transmission from added physical isolation of patients. Multiple factors such as route of exposure, infecting dose, susceptibility of the exposed individual would affect the relative risk of transmission. Currently, recommendations for respiratory and case isolation infection prevention control measures in mpox rely on expert opinion and inferences from data concerning transmission frequency by route of transmission.
Conclusion
No available evidence from comparative interventional studies addressing respiratory and case isolation infection prevention control measures to prevent the transmission of mpox exists. Current findings suggest that transmission occurs primarily through direct physical contact. No cases of transmission via inhalation were identified; the impact of respiratory infection prevention control measures in reducing transmission may be minimal. Covering mpox lesions, wearing a medical mask and avoiding physical contact with others is likely to reduce onward transmission; there is probably minimal additional reduction in transmission from also physically isolating patients. Further research is needed into effective infection prevention control measures to reduce the transmission of mpox.
Data Availability
All data produced in the present work are contained in the manuscript
Studies included in the systematic review
Acknowledgments
Gemma Villaneuva, Anders Bach-Mortensen, Ferrucio Pelone.
Appendix 1. Search Strategy
Search: Monkeypox virus only
Ovid MEDLINE(R) and In-Process, In-Data-Review & Other Non-Indexed Citations and Embase (OVID)
Date of search: 8th September 2022
Monkeypox virus/ or Monkeypox/
monkeypox.ti,ab.
monkey pox.mp.
1 or 2 or 3
Biosis previews (Web of Science) and CAB Abstracts (Web of science)
Date of search: 8th September 2022
Topic = monkeypox*
Global Index Medicus
Date of search: 26th September 2022
Search term: “monkeypox”
Search: Mpox-like viruses
Ovid MEDLINE(R) and In-Process, In-Data-Review & Other Non-Indexed Citations <1946 to September 27, 2022>
Date of search: 28th September 2022
1 orthopoxvirus/ or cowpox virus/ or ectromelia virus/ or vaccinia virus/ or variola virus/
(orthopox* or cowpox or vaccinia or variola or buffalopox).tw.
1 or 2
Masks/ or mask*.mp.
Ventilation/ or ventilation.mp.
air quality.mp.
patient isolation.mp. or Patient Isolation/
8 or 9 or 10 or 11
3 and 12
nosocomial transmission.mp. or Infection Control/
hospital transmission.mp.
15 or 16
3 and 17
18 or 14
Embase 1947-Present
Date of search: 28th September 2022
orthopoxvirus/ or cowpox virus/ or ectromelia virus/ or vaccinia virus/ or variola virus/
(orthopox* or cowpox or vaccinia or variola or buffalopox).tw.
1 or 2
Masks/ or mask*.mp.
Ventilation/ or ventilation.mp.
air quality.mp.
patient isolation.mp. or Patient Isolation/
4 or 5 or 6 or 7
3 and 8
nosocomial transmission.mp. or Infection Control/
hospital transmission.mp.
10 or 11
3 and 12
9 or 13
monkeypox.m_titl.
15 not 16
Web of Science (BIOSIS Previews, CABI: CAB Abstracts®)
Date of search: 28th September 2022 #6 #4 OR #5
#5 #1 AND #3
#4 #1 AND #2
#3 “nosocomial transmission” or “Infection Control” or “hospital transmission” (Topic)
#2 mask* or Ventilation or “air quality” or “patient isolation” (Topic)
#1 orthopoxvirus* or cowpox or vaccinia or variola or buffalopox (Topic)
Global Index medicus
Date of search: 28th September 2022
tw:((tw:(orthopoxvirus* OR cowpox OR vaccinia OR variola OR buffalopox)) AND (tw:(mask* OR ventilation OR “air quality” OR “patient isolation” OR “nosocomial transmission” OR “Infection Control” OR “hospital transmission”)))
Appendix 2.

{kind=link}
Units and Abbreviations
- ACH
- Air changes per hour
- IPC
- Infection Prevention Control
- RT-PCR
- Reverse transcriptase polymerase chain reaction
- WHO
- World Health Organization
References
- 1.
- 2.
- 3.
- 4.
- 5.↵
- 6.
- 7.
- 8.
- 9.
- 10.↵
- 11.
- 12.
- 13.
- 14.↵
- 15.
- 16.↵
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.↵
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.↵
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.↵
- 69.
- 70.↵
- 71.↵
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.↵
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.↵
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.↵
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.



