
Abstract
Objective To investigate the diagnostic and prognostic role of gastric fluid DNA (gfDNA) in gasric cancer (GC) patients and controls submitted to upper digestive endoscopy.
Design The concentration of gfDNA was evaluated in 941 samples, including subjects with normal gastric mucosa (n = 10), peptic diseases (n = 596), pre-neoplastic conditions (n = 99), and cancer (n = 236). gfDNA levels were evaluated according to age, gender, BMI, gastric fluid’s pH, use of proton-pump inhibitors, GC tumor subtypes, histological grades, clinical stages, and disease progression/outcome.
Results In the non-cancer group, we observed that gfDNA levels are increased in women as compared to men (p=7.44e-4). Remarkably, gfDNA levels are increased in GC patients as compared to non-GC (normal + peptic diseases, p=5.67e-13) and in GC versus pre-neoplastic disease (p=1.53e-6). Similar differences were also seen when more advanced tumors (T3) were compared to early stages (T2 and below) (p=5.97-4). Moreover, our results suggest the prognostic value of gfDNA as GC-patients with higher gfDNA concentrations (<1.28ng/µl) had increased infiltration of immune cells in the tumor (p=1.06e-3), which parallels with better disease-free survival (p= 0.014).
Conclusion These findings highlight the significance of collecting and studying stomach fluids from gastric cancer patients and reveals the potential impact of this approach as well as its diagnostic and prognostic value for disease management.
What is already known on this topic
- The DNA contained in biofluids that are in direct contact with tumor lesions is a valuable source of information for cancer diagnosis treatment.
- Gastric fluids are in direct contact with gastric cancer (GC) lesions and immune cell infiltrates and may be a reliable source of biomarkers with multiple applications.
- Liquid biopsies are usually based on the detection and analysis of cell-free DNA found in the plasma, urine or saliva.
- Studies of the DNA present in the gastric fluids of patients (gfDNA), collected during routine endoscopy, are scarce and limited to assessing mutation profiles. It’s diagnostic and prognostic potential has not been studied so far.
What this study adds
- An analysis of gfDNA concentrations in 941 samples revealed increased DNA levels in GC patients as compared to non-GC individuals.
- When tumor stages were compared, gfDNA levels are elevated in more advanced disease.
- For GC subjects, increased gfDNA was positively associated with immune cell infiltrates and reduced tumor recurrence, suggesting this to be an informative and very low-cost prognostic marker.
How this study might affect research, practice or policy
- gfDNA collected during routine upper digestive diagnostic endoscopy can be used as an additional and very simple biomarker useful during patient follow-up and to determine cancer prognosis.
- In the future gfDNA assessment has the potential to contribute to a range of applications, such as monitoring treatment response, indicating immune cell infiltration and may potentially indicate cases with progressive disease non-responsive to chemotherapy.
INTRODUCTION
Gastric cancer (GC) is one of the most common cancer types in some areas of the world, presenting high mortality rates and a patchy, heterogeneous worldwide distribution, with high prevalence observed in regions such as Eastern and Central Asia countries and the Andean South America. According to GLOBOCAN (2020), GC is the fifth most common neoplasm and the third deadliest cancer, with an estimated 768.793 deaths in 2020. At early-stage GC has no specific symptoms and, therefore, tumors are usually detected when the disease is already advanced. This has a direct impact in the survival rates for this disease, leading to 5-years relative survival rates of 70% for patients diagnosed with localized disease, compared to only 6% for subjects who are diagnosed with advanced, disseminated disease (American Cancer Society. Cancer Facts & Figures 2021. Atlanta, Ga: American Cancer Society; 2021; Smyth et al., 2020).
Whereas endoscopic screening, followed by histopathology evaluation of biopsies, is an effective diagnostic tool that allows GC mortality reduction in high-incidence areas (Hamashima et al., 2013; Matsumoto & Yoshida, 2014), it is also employed as a disease management tool, as well as as well as a treatment method in early-stage disease (Kim et al., 2021).
We have recently demonstrated that gastric fluids collected from GC subjects during upper endoscopy contain tumor-derived DNA that can be used for determining mutation profiles and as a patient follow-up tool (Pizzi et al., 2019). Also, as the gastric fluid is in direct contact with the gastric mucosa it has the potential to allow a comprehensive view of the mutational landscape of these tumors, including the cancerization field and multiple tumor lesions. In this way, gastric fluids potentially permit a broader evaluation of the mutational profiles, not only restricted to the few areas of biopsy collection, but also allowing a comprehensive detection of tumor-derived DNA alterations that may potentially indicate actionable mutations and the monitoring of treatment response and disease follow-up (Pizzi et al., 2019).
Early liquid biopsy studies found increased amounts of DNA in the plasma, or even in mouth washes of cancer patients, as compared to non-cancer controls (Leon et al., 1977; Shapiro et al., 1983; Stroun et al., 1987; Nawroz et al., 1996; Anker et al., 1999; Nunes et al., 2000). These consistent findings quickly propelled this field, allowing the identification of tumor-derived mutations in the plasma of patients with colorectal or pancreatic cancer (Vasioukhin et al., 1994; Sorenson et al., 1994). Research in this field was boosted after the cost reduction seen for deep sequencing technologies (Forshew et al., 2012), and the demonstration that many sample types (such as blood, urine, feces, saliva, cerebrospinal fluid, peritoneal washes, and gastric fluids) can be used as DNA sources to support the diagnosis and monitoring of cancer patients.
In this sense, tumor lesions that are in closer or even in direct contact with body fluids may release tumor-derived DNA that can indicate the presence of neoplastic disease allowing precise molecular diagnosis. In the case of GC patients, as gastric fluids are in direct contact with neoplastic areas, the tumor derived DNA is less diluted, as compared to plasma, and it may be a reliable source of biomarkers with multiple applications (Wu et al., 2013; Pizzi et al., 2019). In this study we evaluated 1056 patient-derived gastric fluid samples in order to investigate if DNA amounts found in gastric fluids (gfDNA) would vary according to the presence of malignant versus non-malignant and potentially pre-malignant lesions, tumor subtype and stage, tumor location, patient gender, survival and disease recurrence. Our results have shown a continuous increment of gfDNA amounts in GC patients as compared to non-GC subjects. Within the GC group, higher gfDNA levels appear to correlate with immune cell infiltrates, potentially impacting disease management and disease prognosis.
MATERIALS AND METHODS
Patients
All subjects enrolled in this study were examined by upper digestive endoscopy in a single institution, the A.C.Camargo Cancer Center, São Paulo, Brazil. Samples were collected during endoscopic evaluation, which was only performed after medical indication to assess abdominal complaints made by patients. Samples were obtained after the study was presented to the patients, who have signed an informed consent form previously approved by the Institutional Review Board. Diagnostic and epidemiological data were collected from all subjects (Bartelli et al., 2019).
Determination of the analysis groups
gfDNA was extracted from gastric fluid samples from a total of 1056 individuals. After excluding cases with partial, total gastrectomy, esophagectomy, portal hypertension, and other tumors (e.g., elevated lesion in second duodenal portion, Hodgkin lymphoma, well-differentiated neuroendocrine neoplasm, squamous cell carcinoma of the esophagus, and breast cancer metastasis), a total of 941 subjects (89.1%) remained. These were grouped according to the endoscopy findings as: normal (n = 10, 1.1%), peptic diseases (n = 596, 63.3% - including enanthematic or erosive gastritis, erosive and non-erosive esophagitis associated or not to hiatal hernia, erosive or enanthematous and gastrobulboduodenitis, and peptic ulcer), pre- neoplastic conditions (atrophic gastritis, gastric intestinal metaplasia, dysplasia, Barret esophagus - n = 99, 10.5%), or gastric cancer (n = 236, 25.1%). Diagnostic group, age, gender and BMI of the enrolled participants are shown in Table 1.
General characteristics of participating subjects
Sample collection, DNA extraction, and quantification
All subjects enrolled in the study had medical indication of upper endoscopic examination and were sedated for the procedure. As required for endoscopic examination, all subjects were fasting for more than 8 hours. At the beginning of the procedure, gastric fluids were collected in sterile plastic containers attached to the endoscope suction channel and kept on ice until pH measurement and neutralization. Samples were then kept frozen until DNA extraction, which was performed by standard proteinase-K digestion, followed by phenol-chloroform extraction, ethanol precipitation and washing in 70% ethanol in water. DNA was resuspended in pure deionized water and quantified by QUBIT (Thermo Fisher Scientific).
Quantification of human and bacteria-derived DNA in gastric fluids
For a fraction of our samples (N=180, 19.1%), we also evaluated the proportion of human- and bacteria-derived DNA in gastric fluids using quantitative PCR (Albuquerque et al., 2022).
Analysis of inflammatory cell infiltrates in tissue biopsies
Fragments of tumor tissue biopsies were still available from a small subset of cases evaluated for the gfDNA content. In this case, after the microscopic identification of cancer cells and the histological classification of GC, the presence and intensity of inflammatory cell infiltrates in the neoplastic lesions were also evaluated, as well as their patterns in the tumor stroma (diffuse, microscopic lymphoid aggregate, lymphoid aggregate with the formation of hyperplastic germinal centers). We have also described the predominant cellular composition of the inflammatory infiltrate, and quantified the approximate infiltrate/tumor stroma ratio as: i) minimal/rare – rare inflammatory cells in the tumor stroma; ii) moderate – moderate cellularity, no distortion of the epithelial component and no formation of luminal micro-abscesses and iii) intense/elevated - large amounts of inflammatory cells, making it difficult to visualize the stroma, with the formation of luminal micro-abscesses and/or epithelial thinning. We have also evaluated the presence of lymphoid aggregates, necrosis/ulcer and neutrophilic infiltrate. Areas directly related to ulcer and granulation tissue were not considered in the polymorphonuclear component assessment.
Statistical analyses
Baseline gfDNA levels for patient groups are given as a median. Analyses were performed in the R statistical environment (version 4.2.0, R Core Team, 2022). Statistical analysis was carried out using Mann-Whitney and Kruskal-Wallis tests for comparisons among two and three groups, respectively. Survival data was collected for all subjects and the cutoff on DNA concentrations to separate survival groups was determined according to the log-rank test (function maxstat.test from R package maxstat; Hothorn, 2017). Distributions of DNA concentrations for the four groups of patients (normal, peptic diseases, pre-neoplastic conditions, or gastric cancer) were compared using the two samples Wilcoxon test, and p-values were adjusted by the Benjamini-Hochberg procedure (aka, False Discovery Ratio). Logistic Regression Analysis was used to determine Receiver Operating Characteristics (ROC) and Area Under the Curve (AUC). Results were considered statistically significant when p ≤ 0.05.
RESULTS
gfDNA levels according to age, pH of gastric fluids and BMI
No significant variations in gfDNA levels were found when subjects were grouped according to age, pH of gastric fluids and Body Mass Index (BMI). Subjects were clustered in three age groups (<45, 45-60, and >60 years old) and no significant differences were found between cancer (p = 0.26) or non-cancer subjects (p = 0.14). For the analysis of gastric fluids’ pH, samples were grouped as pH<7, pH=7 or pH>7; we found p-values of 0.60 and 0.91 respectively for GC and non-cancer controls. For BMI analysis, subjects were grouped as: i – underweight (BMI< 18.5); ii – normal (BMI between 18.5 - 24.9); iii – overweight (BMI between 25 - 29.9), or iv - obese, BMI ≥ 30. Again, no significant differences in gfDNA levels were found: i) pH group values in gastric cancer individuals (p = 0.604), or for subjects with no cancer (p = 0.907) and ii) BMI groups in cancer individuals (p = 0.60) or non-cancer subjects (p = 0.26) (Suppl. Fig. 1).
gfDNA levels and gender
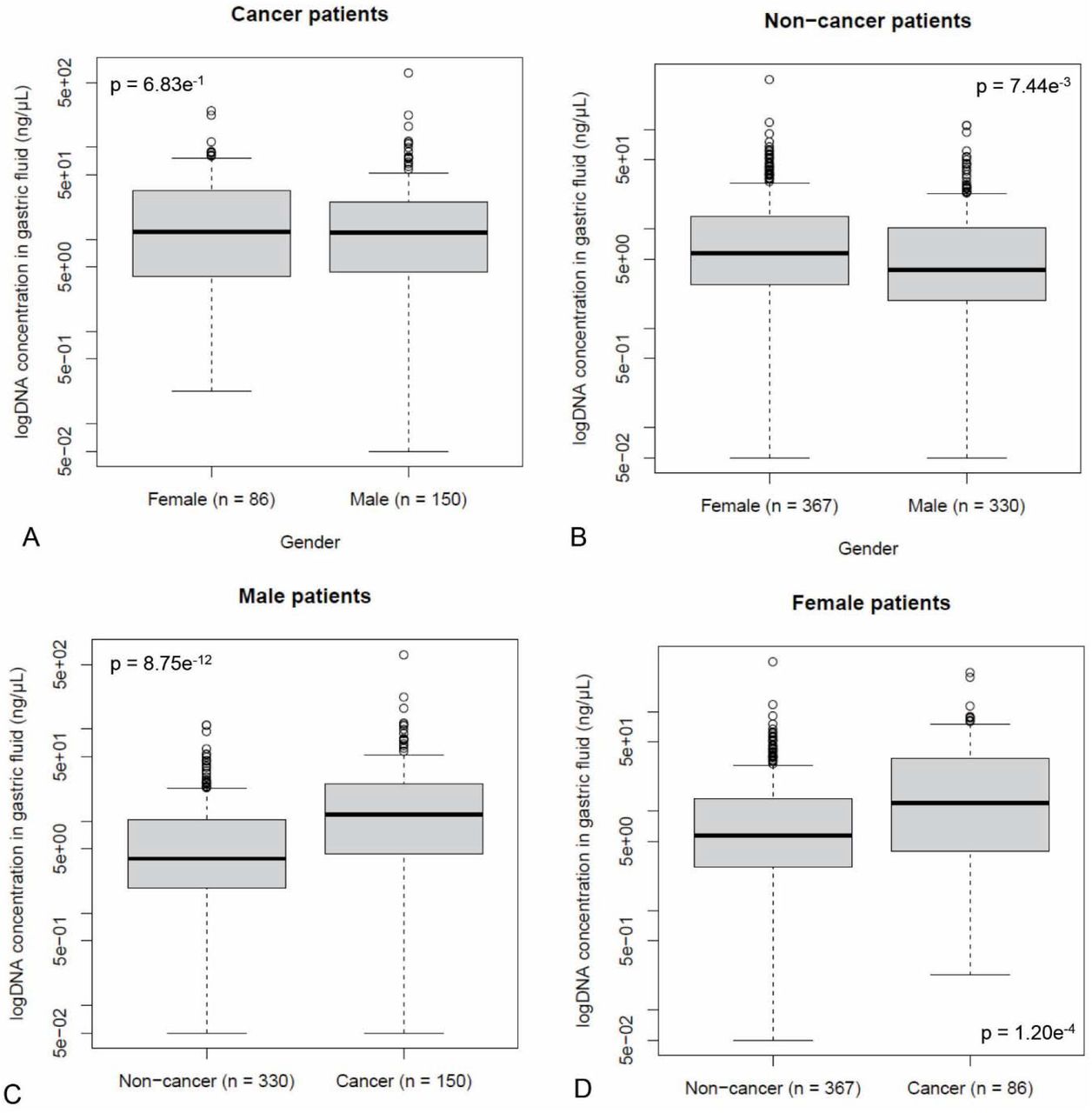
Next, we evaluated whether gfDNA concentrations would vary according to gender in non-cancer and GC-patients. For the non-cancer cohort, we observed elevated gfDNA concentrations in females versus males (p = 7.44e-3) (Figure 1B). Therefore, when we compared gfDNA levels between cancer x non-cancer subjects, considering gender, we found striking differences for men and for women, respectively, p = 8.75e-12 and p = 1.20e-4 (Figures 1C and 1D). This difference in gfDNA levels was no longer present when we compared males versus females from the cancer group (p = 0.68), probably due to an increment in gfDNA for when GC is present (Figure 1A).

gfDNA levels observed in GC-patients as compared to non-cancer, according to gender (A, B), or in males versus females according to presence of GC (C, D).
As some studies suggest that the use of proton pump inhibitors (PPIs) is more frequent in women (Hoffmann et al., 2015; Rückert-Eheberg et al., 2021), we evaluated possible links between gfDNA levels and the reporting of current, previous or no PPIs use (Suppl. Fig. 2). In general, we see no impact of PPI over gfDNA concentrations (Suppl. Fig. 2G-H). However, for the group of non-cancer subjects that made use of proton pump inhibitors (N=410), increased gfDNA levels are seen for women (N=206) as compared to men (N=204) (p= 1.51e-4) (Suppl. Fig. 2F). Moreover, gfDNA levels was not different for subjects that reported current and previous administration, as well as no-administration of PPIs, for females with or without cancer (N=55, N=6 and N=25; N=111, N=45 and N=206, respectively), as well as for males with or without cancer diagnosis (N=60, N=19 and N=66; N=75, N=51 and N=209, respectively, with corresponding p-values of p= 0.93; p= 0.07; p= 0.24 and p= 0.72) (Suppl. Fig. 3A to 3D).
Analysis of bacteria:human ratios in gfDNA
As the origin of the gfDNA is likely to be a sum of host DNA (tumor and non-tumor human cells), combined with the DNA from the microbiota (originating from transient microorganisms from the saliva, as well as the resident gastric microbiota), we performed a quantitative analysis of bacteria and human DNA for a subset of 180 samples, using an approach recently described by our group (Albuquerque et al., 2022). The samples selected for the analysis of this subset included all 10 subjects from the N group (no pathologies detected), as well similar numbers of samples from the peptic diseases group (N = 51), preneoplastic conditions (N = 55) and the cancer group (N = 64). For this limited sampling we found no significant differences in the amounts of human- or bacteria-derived DNA present in the gfDNA (Suppl. Table 1).
gfDNA levels are increased in gastric cancer patients as compared non-neoplastic cases
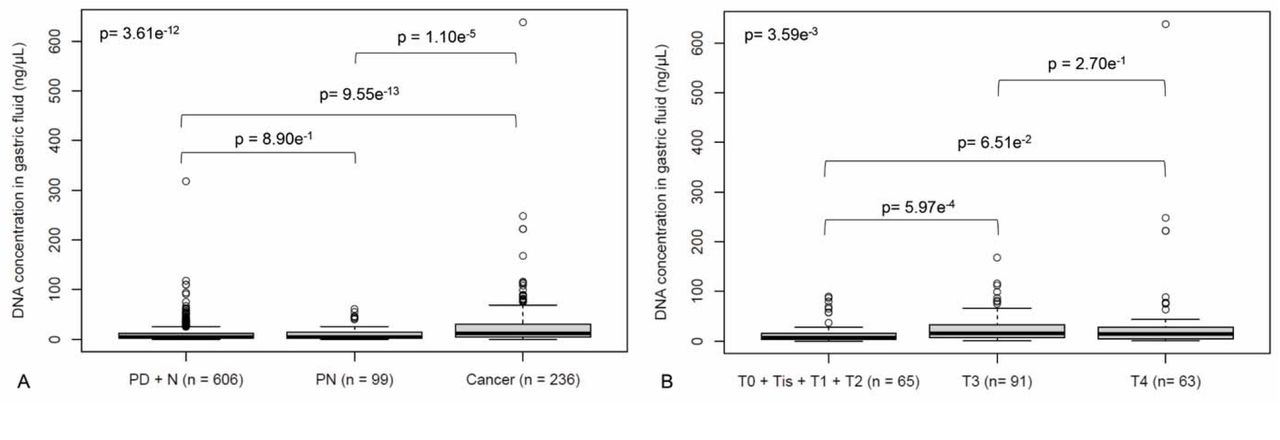
We evaluated the concentration of gfDNA from subjects with different diagnoses after upper endoscopic examination. Our findings demonstrated the following median concentrations of gfDNA in these groups: normal (N) (6.38 ± 12.00 ng/µL; N=10), peptic diseases (PD) (5.00 ± 19.50 ng/µL; N=596), preneoplastic conditions (PN) (4.18 ± 12.72 ng/µL; N=99), which were not different from each other, but are all distinct from gastric cancer (11.90 ± 53.37 ng/µL; N=236; p= 3.6e-12) (Figure 2A). Gastric fluids from GC samples presented higher levels of gfDNA as compared to a combination of groups N+PD groups (merged due to the very small size of group N) (p= 5.67e-13), as well as to the PN group (p= 1.53e-6) (Figure 2A). Groups of non-neoplastic disease showed no differences in gfDNA levels among them (Suppl. Figure 4).

A) gfDNA concentration (ng/µL) in patients with no endoscopic findings (Normal, N) or presenting peptic diseases (PD), preneoplastic conditions (PN), or gastric cancer. B) gfDNA concentrations (ng/µL) for early-stage disease patients (T0 + Tis + T1 + T2), as compared to more advanced disease stages T3 and T4.
Next, for the GC group patients, we evaluated possible correlations between gfDNA levels and clinical variables such as T-stage and histological grades. In general, our results point to increments in gfDNA in subjects with more advanced disease (Figure 2B). The gfDNA median concentration found for the combined early-stage disease groups (tumor stages - T0 + Tis + T1 + T2; N=65) was of 7.3 ± 21.71 ng/µL as compared to about a double, seen for T3 (15.4 ± 29.76 ng/µL; N=91; p = 5.97e-4) or T4 stages (14.3 ± 91.71 ng/µL; N=63; p = 0.07). Other comparisons showed p-values >0.05, including gfDNA concentrations for 165 cases with localized disease versus 71 with metastatic disease (N+ and M1; p = 0.1 – data not shown). Besides, gfDNA levels could not differentiate tumor histological grade groups (Suppl. Fig. 5). When gfDNA levels were compared between gastric cancer subjects stratified according to the Lauren subtypes: diffuse (N=97), intestinal (N=93) or mixed (N=25) subtypes (p= 0.28).
gfDNA is a potential new gastric cancer biomarker that correlates with gastric cancer survival and the presence of inflammatory cells infiltrates
Our results indicate gfDNA levels are increased in gastric cancer patients as compared to non-cancer individuals. In Figure 3A we show the Receiver Operating Characteristic (ROC) curve of gfDNA between the cancer versus non-cancer subjects. The results showed a statistically significant curve (Area Under the Curve AUC = 0.66; p = 5.23e-10), with a fair capability of detecting true positive GC-cases simply considering gfDNA levels. Besides, the ROC curve of gfDNA between cancer/preneoplastic conditions and peptic diseases/normal, again indicates the potential of this analysis to support diagnosis, with statistically significant findings (AUC = 0.61 and p = 6.86e-07 – Figure 3B).

Analysis of Receiver Operating Characteristics (ROC) and Area Under the Curve (AUC) for gfDNA levels between cancer patients and non-cancer individuals. A) ROC curve of gfDNA between the cancer patients and non-cancer individuals. B) ROC curve of gfDNA between cancer versus non-cancer and cancer + preneoplastic conditions versus peptic diseases + normal.
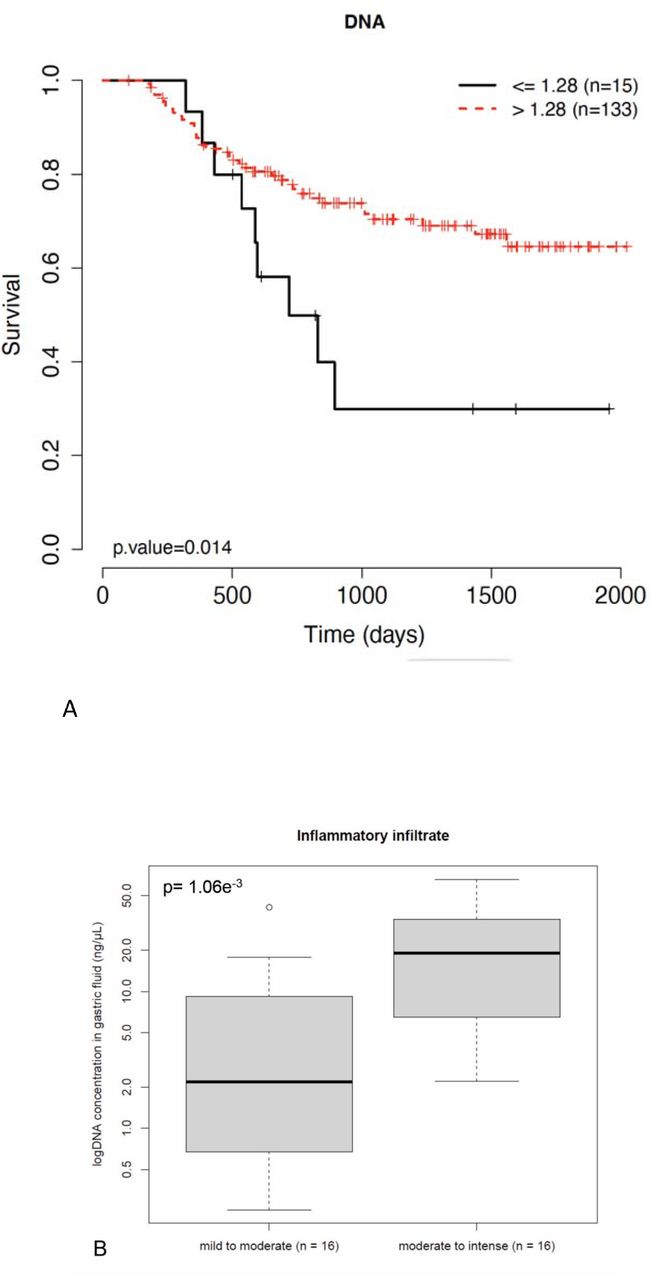
We evaluated if DNA concentrations would impact disease prognosis. Clinical records were collected for all GC-subjects of the cohort, and the cutoff on DNA concentrations that would split the patients in groups showing more contrasting overall survival were determined (Hothorn, 2017). Our results indicate that GC-patients presenting higher gfDNA concentrations (>1.28ng/µL) have better survival (N = 163; p = 0.019); the same was true after excluding metastatic subjects (N = 148; p = 0.014) (Figure 4A).

(A) For a total of 148 non-metastatic GC patients, cutoff gfDNA concentrations determined by a log-rank test (1.28 ng/µL) correlated to overall progression (p = 0.0014). (B) For a subset of 32 cases, for which representative biopsy H&E slides were available, inflammatory cell infiltrates in the gastric tumors were inspected by experienced pathologists and have shown that more intense inflammatory infiltrates in tumors are present in subjects with more intense gfDNA concentration (p = 1.06e-3).
As the increased gfDNA concentration was apparently seen in GC patients presenting more favorable outcomes, for a set of 32 subjects (8 with lower gfDNA and 24 with higher gfDNA), we investigated if gfDNA concentrations could possibly be correlated with the intensity of inflammatory cells infiltrates. The result was positive, (p=1.06-3) (Figure 4B and Suppl. Table 2), supporting the contrasting survival data and gfDNA from Figure 4A.
Discussion
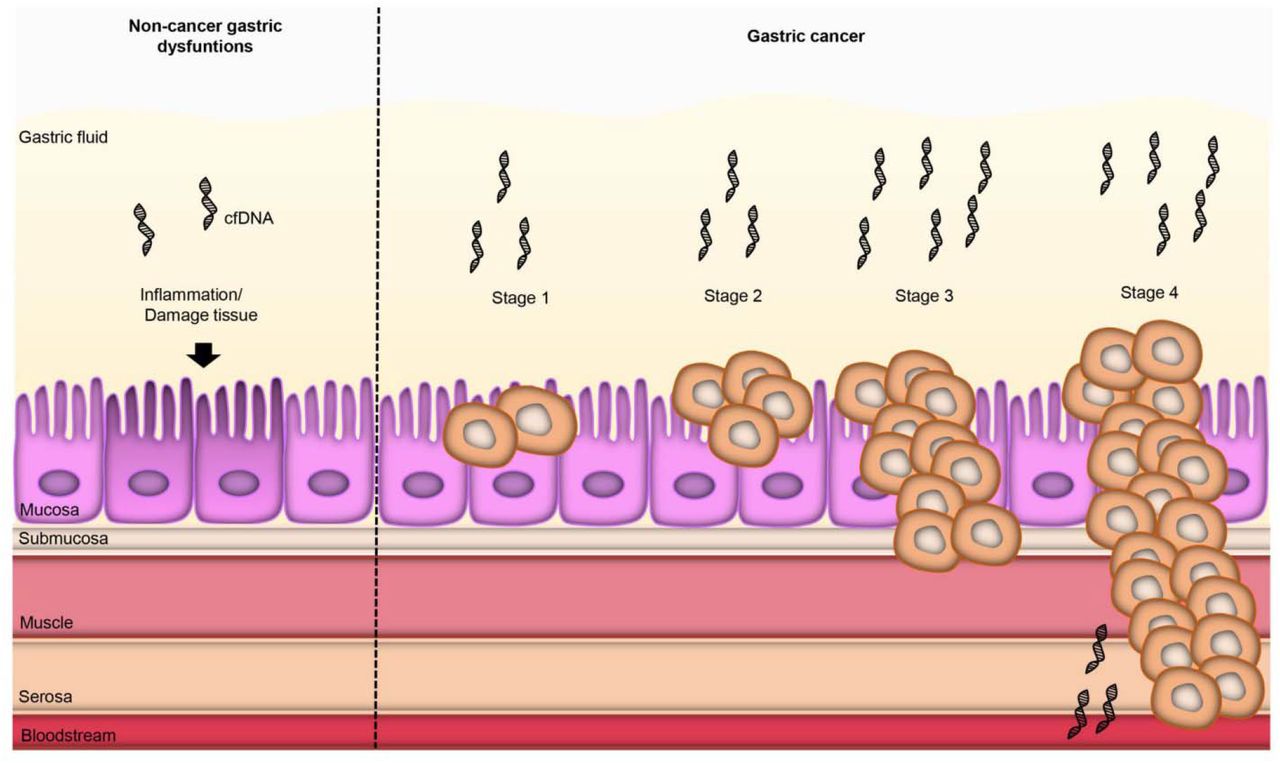
The study of gastric fluids has been limited to the evaluation of certain molecules, such as proteins, microRNAs or for the analysis of mutations in specific genes (Wu et al., 2013; Shao et al., 2014; Pizzi et al., 2019). The results we present here suggest that the DNA content of gastric fluids collected from gastric cancer patients during upper endoscopy is elevated, as compared to peptic diseases and preneoplastic conditions, reinforcing the utility of gfDNA for the study of gastric cancer. This elevation of gfDNA levels was consistent for all Lauren subtypes. However, whereas we found no significant variations among tumor histological grades, we found a consistent trend for increased gfDNA levels when early x advanced disease stages were compared (Figure 2B). While in average T4 tumors still have elevated gfDNA concentrations, similar to T3 tumors (T3: 15.4 ng/ml, ±29.76 and T4: 14.3 ng/ml, ±91.71), the difference between T4 and earlier stages (T2 and below) was marginal (p = 0.06), probably due to the higher variability of gfDNA concentration seen for T4 (Figure 2B). We postulate that this heterogeneity may be intrinsic to the T4 stage, as some tumors are more invasive than others and, the tumor mass would grow through the gastric wall and the serosa (Fukuda et al., 2011), thus shedding DNA into adjacent structures as opposed to the gastric cavity, leading to a reduction of gfDNA levels, as opposed to T0-T3 tumors that appear to continuously release DNA inside the stomach (Figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic view of a model based in our findings. The presence of a gastric cancer lesion would lead to increased concentrations of gfDNA, as compared to non-cancer status, including peptic diseases and pre-neoplastic conditions. As the disease advances, gfDNA concentrations would gradually increase until the tumor starts invading adjacent tissues and releasing DNA in contiguous structures other than the gastric cavity. The influence of inflammatory cell infiltrates in the tumor mass, which appear to contribute to higher gfDNA concentrations in GC-cases, is not illustrated here.
In agreement with this, we found that more advanced tumors have increased gfDNA concentration as compared to earlier stages, a finding that may suggest that the origin of the gfDNA could derive from the tumor, but also from the environment - including inflammatory cells and the microbiota. However, our quantitative analysis of bacterial and human DNA in the gfDNA for a set of 180 samples, including 64 cancer samples, showed no clear trends towards an increased bacterial or human DNA. Besides, we found a correlation between gfDNA concentration and survival. GC-patients presenting lower gfDNA concentrations (≤ 1.28 ng/µL) appear to have worse prognosis. We envisaged that this finding could be correlated to poorer immune responses (cold tumors) a hypothesis that appears to be true as we observed that patients with higher gfDNA concentrations (>1.28 ng/µL) more often presented moderate to intense inflammatory infiltrates, whereas individuals with lower gfDNA (≤1.28 ng/µL) usually presented mild to moderate inflammatory infiltrates (p=1.06-3).
Plasma-derived DNA is the most popular source of cell free DNA (cfDNA) for tumor follow-up and even for cancer diagnosis (Allouchery et al., 2021). One of its advantages is its simple collection. A study with a large cohort of 640 subjects (Bettegowda et al., 2014) indicated that individuals with stage IV of cancer presented nearly 100 times more cfDNA levels in the plasma as compared to stage I disease, suggesting a potential prognostic value for cfDNA levels. On the other hand, a reduction in cfDNA after treatment seems to indicate a positive therapy response (Zhuang et al., 2017; Scherer et al., 2016; Santiago-Walker et al., 2016; Gray et al., 2015; Wang et al., 2010; Gautschi et al., 2007; Lecomte et al., 2002). Qian et al. (2017) analyzed cfDNA in serum samples of gastric dysfunctions, such as benign gastric disease and gastric cancer, and healthy controls. Their findings indicate that gastric cancer patients presented elevated levels of cfDNA when compared to benign gastric disease or normal controls. Also, the results showed that advanced disease (stages III – IV) and tumor size (>5 cm) presented more cfDNA levels than earlier stages and smaller tumor size.
Our results suggest that the increased DNA concentrations are also found in gastric fluids of GC patients as compared to non-cancer individuals. This increment appears to be independent on age, BMI, gender, PPI-usage or Lauren’s subtypes, but was associated to the presence of the disease, varying from mean concentration ranges between 4.18-6.38 ng/µL in non-neoplastic conditions to 11.9 ± 53.37 ng/µL in GC cases (p= 3.61e-12). In parallel with cfDNA, it is significant to observe a continuous growing trend in the amounts of gfDNA according to tumor stage, with increasing mean values of 15.12 ± 21.71 ng/µL (T0 + Tis + T1 + T2; N=65), 25.66 ±29.76 ng/µL (T3; N=91) and 38.12 ± 91.71 ng/µL (T4; N=63).
The most obvious barrier of using gfDNA in the routine is the need to perform an endoscopy in order to access it. Whereas the monitoring of tumor DNA in the plasma has clear advantages directly related to the easy collection in multiple time-points for patient follow-up, the use of gfDNA as a source of tumor-derived DNA may present some relevant benefits. The most relevant aspect is related to the proximity to the tumor site, which leads to a much-reduced dilution of tumor-derived DNA and a better representation of tumor-related DNA alterations, as tumors will shed cells and cell debris into the surrounding fluids. In this sense, the study of gfDNA would resemble that of peritoneal lavage of patients with endometrial carcinoma, who showed that this fluid contains significantly higher mutant allelic fractions as compared to plasma (Mayo-de-las-Casas et al., 2020) and as previously demonstrated by our early work (Pizzi et al., 2019).
Given the importance of this cancer type, studies have been looking for new tools for detecting diagnostic, prognostic, and predictive markers (Wu et al., 2014; Yu et al., 2016). Our AUROC analysis with gfDNA showed a discrimination capability of 0.66, which is far from ideal, but still comparable to biomarkers such as CEA (0.68), CA72-4 (0.67) and CA19-9 (0.64) (Qian et al., 2017). On the other hand, gastric fluids seem to contain significant amounts of tumor-derived DNA, as we have previously demonstrated (Pizzi et al., 2019) and may be valuable in the context of liquid biopsies, when tumor-derived mutations or aberrant methylation of selected genes such as P16, CDH1 or MGMT, may provide additional biomarker tools for diagnosis and follow-up studies (Tahara & Arisawa, 2015; Lin et al., 2020). In this sense, the monitoring of gfDNA concentration may be valuable for a closer follow up of patients with potentially pre-malignant diseases and, for the already diagnosed GC cases, the monitoring of gfDNA may be used in the future as surrogate marker of immune cell infiltration and a potentially more aggressive disease.
The collection of gastric fluids during endoscopy is a straightforward procedure that is already part of the endoscopic procedure, when the gastric walls must be free of fluids for a better visualization. The easy incorporation of gastric fluid collection into the examination procedure and its low cost favors the adoption of gastric fluid collection for future screening approaches. Whereas we don’t advocate the use of upper endoscopic access to simply collect gfDNA, we suggest that the gastric fluid can be used as an additional valuable source for patient monitoring and prognosis, as it can be easily collected during routine endoscopy or at the pre- and post-surgical evaluation of patients with gastric cancer. Further applications may include the closer follow-up of subjects in high-risk for gastric cancer development, and the intriguing possibility of evaluating gfDNA levels in different moments of the peri-operatory chemotherapy regimen as a potential biomarker to indicate treatment response, potentially directing non-responders more rapidly to surgery. We hope that our study will encourage the collection and study of gastric fluids, a source of potentially rich and informative biomarkers of the gastric environment that may facilitate the comprehension of gastric diseases, not only limited to gfDNA, but also including the microbiota, proteomic, transcriptomic and metabolomic studies.
Data Availability
All data produced in the present study are contained in the manuscript and in its supplementary information files
Competing Interests
None.
Contributions
Collection of samples and clinical data: FCC, AGP, CZS, LBCS, GPB, FAP, LLSA,
Conceived and performed analysis: FC, TFB, RD, ITS, DNN, EDN
Pathology: APB, GOS, WAN,
Discussion of findings, manuscript writing and reviewing: LGVC, ML, FJFV
Data analysis and statistics: FCC, AD, RDD, ITS, TFB, DNN, ED-N
Project supervision: ED-N
Funding
The collection of samples and metadata, DNA extraction and further analyses performed here were supported by grants by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, 14/2687-0, 18/14267-2, 18/02972-3) and Departamento de Ciência e Tecnologia (DECIT), Ministry of Health, Brazil (PRONON, SIPAR 2500.035-167/2015-23).
Patient consent for publication
Not applicable.
Ethics approval
The study was approved by the ethics committee of the A.C.Camargo Cancer Center (protocol 2134/15). Written and informed consents were obtained from all subjects or their guardians.
Authors ORCID, Affiliation and email
Francine Carla Cadoná, PhD
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
Mestrado em Ciências da Saúde e da Vida, Universidade Franciscana, Santa Maria, RS, Brazil.
francinecadona{at}gmail.com
Adriane Graicer Pelosof, MD
Endoscopy sector, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
adriane.pelosof{at}accamargo.org.br
Claudia Zitron Sztokfisz, MD
Endoscopy sector, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
claudia.zitron{at}accamargo.org.br
Adriana Passos Bueno, MDa
Department of Pathology, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
adriana.passos{at}accamargo.org.br
Luana Batista do Carmo dos Santos, BSc
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
luana.santos{at}accamargo.org.br
Gabriela Pereira Branco, BSc
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
gbranco{at}accamargo.org.br
Gabriel Oliveira dos Santos MD, MSc
Department of Pathology, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
patologista{at}live.com
Warley Abreu Nunes, MD
Department of Pathology, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
warley.nunes{at}accamargo.org.br
Fernanda Araújo Pintor, RN
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo and Department of Abdominal Surgery, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
fernanda.pintor{at}accamargo.org.br
Laís Lie Senda de Abrantes, RN
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo and Department of Abdominal Surgery, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
lais.senda{at}accamargo.org.br
Alexandre Defelicibus, PhD
Laboratory of Computational Biology and Bioinformatics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
alexandre.defelicibus{at}accamargo.org.br
Luiz Gonzaga Vaz Coelho, MD, PhD
Programa de Pós-Graduação em Ciências Aplicadas à Saúde do Adulto & Instituto Alfa de Gastroenterologia, Hospital das Clínicas, Faculdade de Medicina, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil.
lcoelho22{at}gmail.com
Marcis Leja, MD, PhD
University of Latvia, Institute of Clinical and Preventive Medicine and Center for Gastric Diseases GASTRO, Riga, Latvia.
marcis.leja{at}lu.lv
Felipe José Fernandez Coimbra, MD, PhD
Department of Abdominal Surgery, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
felipe.coimbra{at}accamargo.org.br
Rodrigo Drummond, PhD
Laboratory of Computational Biology and Bioinformatics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
rdrummond{at}accamargo.org.br
Israel Tojal da Silva, PhD
Laboratory of Computational Biology and Bioinformatics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
Itojal{at}accamargo.org.br
Thais Fernanda Bartelli, PhD
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
tfbartelli{at}mdanderson.org
Diana Noronha Nunes, PhD
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
dnoronha{at}accamargo.org.br
Emmanuel Dias-Neto, PhD
Lab. of Medical Genomics, A.C.Camargo Cancer Center, São Paulo, SP, Brazil.
emmanuel{at}accamargo.org.br
Acknowledgements
Authors acknowledge the support given by the institutional Tumor Bank from A.C.Camargo Cancer Center. We thank Dr. Christian Abnet (NCI, NIH, USA) for his critical review of this manuscript. ED-N is a researcher from Conselho Nacional de Pesquisas (CNPq).
References



