
Abstract
Background Cardiovascular events remain one of the frequently reported causes of death globally.
Aims Assess the early laboratory and instrumental changes in systemic manner.
Objectives Patients with fresh myocardial infarction that has been occurred in less than 30 days before hospitalization in the rehabilitation hospital.
Materials and methods A single large scale retrospective cohort sectional study for patient with fresh myocardial infarction for the period of 2014-2019, data collected from Mordovia Rehabilitation Hospital. The study involved 154 patients and analyzed 76 parameters for each patient. The t-test, Pearson correlation coefficient, and ROC test has been used. For statistical analysis used Statistica program.
Results The sample included 154 patients with history of fresh myocardial infarction. Of 154. 51(33.11%) female and 103 (66.88 %) males. chronic heart failure (CHF), which is seen in 42 (27.27273 %) patients, 101 (65.58442 %) did not have a CHF, and 11 (7.14286 %) missing data. Diabetes mellitus (DM) has been observed in 28 (18.18182 %), 118 (76.62338 %) without DM, Hypertension has been seen in 118 (76.62338 %), 28 (18.18182%) did not have hypertension, chronic kidney disease (CKD) has been seen in 11 (7.14%) patients, 131 (85.06494 %) did not have CKD, Chronic obstructive pulmonary disease (COPD) existed in 14 (9.09091%), 132 (85.71429 %) did not have COPD. Post myocardial infarction (MI) CHF has been seen in 108 (70.12987%), 42 (27.27273 %) did not have CHF. Post MI arrythmia seen in 50 (32.47%) patients, 99 (64.28571%) did not have arrythmia. Early post MI complication such as aneurysm has been seen in 12 (7.79221%), 138 (89.61039 %) did not have aneurysm, Dressler syndrome; pericarditis has been seen in 4 (2.59740%) patients, pneumonitis seen in 1 (0.64935%) patient, and pleuritis have not been seen.
Conclusions Systemic manifestations include kidney function impairment or development of new kidney disease. Of these changes include increase in the aorta basement diameter, increase in the right ventricle wall thickness, decrease in the level of serum red blood cell, serum potassium level, and serum calcium level, with increase in the serum myoglobulin.
Others Females are more frequently affected with post MI urinary tract infection.
Introduction
Myocardial infarction (MI) and it is associated sequalae remains the most frequently reported cause of mortality and morbidity worldwide [1]. The development of cardiovascular events is associated with several modified and non-modified risk factors [2]. The lifestyle changes have huge impact on the overall health of the cardiovascular system [3, 4]. Unfortunately, sedentary life style is seen in majority of myocardial infarction victims which is associated with development of several predisposition factors for the cardiovascular events such as dyslipidemia, insulin resistance, and central obesity or visceral obesity [5–7]. Cumulatively, these early signs of cardiovascular homeostasis disturbance are ignored to provoke the progression of dyslipidemia and insulin resistance to reach enough level to induce the emergence of cardiovascular event such as MI [8, 9].
Assessment of the early post-MI changes is of huge impact on the further therapy plan and the prognosis of MI victims. One of the early specific markers of myocardial infarction is elevation in the cardiac lactate dehydrogenase 1 and troponins including troponin I and T. However, systemic changes are rarely assessed in early pot-MI patients [10]. The role of these changes remains not clear in the determination of the prognosis of MI patients and the potential risk of development of complications such as renal failure. In the current retrospective analysis, we covered the potential role of these systemic and the regularly checked cardiac markers in the prognosis determination and prognosis of the patients.
Materials and methods
A retrospective cohort analysis for 155 patients for the period 2014-2019. The data has been collected from the republican rehabilitation hospital. The consent of the patients has been taken for gathering, analyzing and publication the material and any associated photos or graphs. The missing data has been treated as absent and removed from the analysis. All the measurement units are according to the local units used in the laboratories. There was no access to the 2020–2022 year data because of the COVID-19 issues. Pleuritis was not seen in patients and been excluded from the complications report. The presented t test results are all statistically significant, and other non-mentioned results are statistically not significant at p<0.05. the leukocytes and the red blood cell level is always mentioned without the *109 or *1012, respectively. We could not assess the risk hazard for the estimated parameters and the survival rate, limitations of the study.
T-test, Pearson correlation coefficient, and ROC analysis have been used using Statistica 12 program (StatSoft, Inc. (2014). STATISTICA (data analysis software system), version 12. www.statsoft.com.).
Results
The sample included 154 patients with history of fresh myocardial infarction. Of 154. 51(33.11%) female and 103 (66.88 %) males. In the sample, 131 (85.06494 %) lives in the city, 17 (11.03896 %) lives in the village, and 5 (3.24675%) lives in the town.
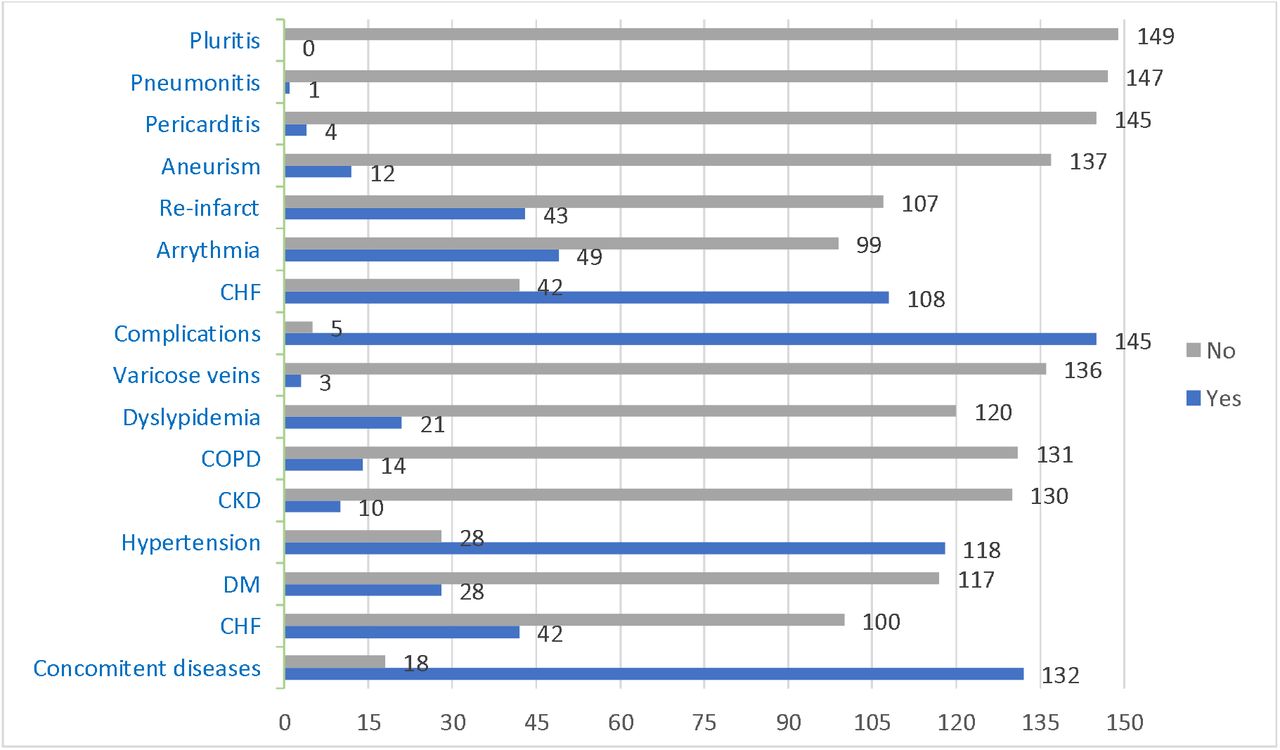
Majority of the patient had a concomitant disease prior to their myocardial infarction. 132 (85.71429%) had a concomitant disease, 18 (11.68831%) did not have a concomitant disease, and 4 (2.59740 %) missing data. Of the concomitant diseases is chronic heart failure (CHF), which is seen in 42 (27.27273 %) patients, 101 (65.58442 %) did not have a CHF, and 11 (7.14286 %) missing data. Diabetes mellitus (DM) has been observed in 28 (18,18182 %), 118 (76.62338 %) without DM, and 8 (5.19481 %) missing data. Hypertension has been seen in 118 (76.62338 %), 28 (18.18182%) did not have hypertension, and 8 (5.19481%) missing data. Chronic kidney disease (CKD) has been seen in 11 (7.14%) patients, 131 (85.06494 %) did not have CKD, and 12 (7.79221 %) missing data. Chronic obstructive pulmonary disease (COPD) existed in 14 (9.09091%), 132 (85.71429 %) did not have COPD, and 8 (5.19481 %) missing data. Disrupted lipid profile was present in 21 (13.63636 %), 121 (78.57143 %) did not have dyslipidemia, and 12 (7.79221 %) missing data. Varicose vein is coexisted in 3 (1.94805%), 137 (88.96104%) did not have varicose vein, and 14 (9.09091%) missing data.
In terms of post myocardial infarction complications, 145 (94.15584 %) patients had complication, 5 (3.24675%) did not have complication, and 4 (2.59740%) missing data. Post myocardial infarction (MI) CHF has been seen in 108 (70.12987%), 42 (27.27273 %) did not have CHF, and 4 (2.59740 %) missing data. Post MI arrythmia seen in 50 (32.47%) patients, 99 (64.28571%) did not have arrythmia, 5 (3.24675%) missing data. Early post MI complication such as aneurysm has been seen in 12 (7.79221%), 138 (89.61039 %) did not have aneurysm, and 4 (2.59740%) missing data. Late post MI complications including Dressler syndrome including the pericarditis has been seen in 4 (2.59740%) patients, 146 (94.80519%) did not have pericarditis, and 4 (2.59740 %) missing data. Additional components of the Dressler syndrome include pneumonitis, which is seen in 1 (0.64935%) patient, 148 (96.10390%) did not have pneumonitis, and 5 (3.24675 %) missing data. Whereas, the third component of the Dressler syndrome, pleuritis, have not been seen, therefore, it has not been reported.
Interestingly, 43 (27.92208%) patients had re-infarct, 107 (69.48052 %) were for the first time, and 4 (2.59740 %) missing data. Assessment of the activity level of tissue-type plasminogen activator (t-PA) through d-dimer level in the serum, it was elevated in 7 (4.54545%) patients, 5 (3.24675%) normal range, other 142 (92.20779%) did not measure their d-dimer level.
The primary descriptive statistics demonstrated in (Table) 1.
The primary descriptive statistics of the sample. Abbreviations: EF; ejection fraction, EDV; end diastolic volume, LV; left ventricle, LA; left atrium, RV; right ventricle, RA; right atrium, Hb; hemoglobin, RBC; red blood cell, ESR; erythrocytes sedimentation rate, CKP-MB; creatinine phosphokinase-MB fraction, LDH; lactate dehydrogenase, ALT; alanine transaminase, AST; aspartate transaminase, LDL; low density lipoprotein, TAG; triacyl glycerides, APTT; activated prothrombin time, PT; prothrombin time.
Males are affected in myocardial infarction earlier in comparing to female, the cut-off point of age is 67 years old. (Figure 1)

Cut-off point for the age of the patients divided in to male and female. Males are less than 67 years old. Whereas, female affected at more 67 years old.
In male group the mean age is 59.76 years old and in female group the mean age is 65.46 years old, which is statistically significant difference, t value 3.30972, p<0.001170. Moreover, mean height of the male is 172.57 cm, and in female 164.88 cm, which is statistically significant difference, t value -3.26225, p< 0.002829. On echocardiogram, in male group, the mean diameter of the aorta is 36.23 mm, in female group, the mean diameter of the aorta is 33.04 mm, which is statistically significant difference, t value -4.24952, p<0.000039. In male group, the mean right atrium wall thickness on echocardiogram equal to 36.26 mm, in female group equal to 34.56 mm, which is statistically significant difference, t value -2.06826, p< 0.040630. Mean hemoglobin level in male was 140.26 and in female was 130.66, which is statistically significant difference, t value -3.71265, p<0.000295. In urine analysis, in male group, mean number of leukocytes in urine was 1.52 under microscope and in female group was 4.91, which is statistically significant difference, t value 3.11688, p< 0.002218. Moreover, in urine analysis, number of the epithelial cells in the male 1.36 under microscope and in female group 2.91, which is statistically significant difference, t value 3.12012, p< 0.002214. In male group, the mean myoglobulin level was 67.00 ng/ml and in female was 199.90 ng/ml, which is statistically significant difference, t value 19.18246, p< 0.033158.
Patients with concomitant diseases have a mean heart rate (HR) equal to 80.82 beat/mint and patients without concomitant disease have mean HR equal to 72.39 beat/mint, which is statistically significant difference, t value 2.05541, p< 0.041633. Additionally, patients with concomitant diseases have a mean right ventricle wall thickness of 27.13 mm and patients without concomitant disease have a mean right ventricle wall thickness of 23.85 mm, which is statistically significant difference, t value 2.79969, p< 0.005833. Moreover, patients with concomitant disease have a mean protein in urine 3.18 mg/l, and the patients without concomitant disease had a mean level of urine protein 21.25 mg/l, which is statistically significant difference, t value -3.10080, p< 0.002353. Interestingly, patients with concomitant disease had lower calcium level a mean equal to 1.31 mmol/l and the patients without concomitant disease had a mean calcium level 3.84 mmol/l, which is statistically significant difference, t value -2.67394, p< 0.008608. (Figure 2)

Diagramed presentation of the concomitant and the post MI compilations. From below up to complications (CHF, DM, hypertension, CKD, COPD, dyslipidemia, varicose veins) belongs to concomitant diseases before the development of MI. Abbreviations: CHF; chronic heart failure, COPD; chronic obstructive pulmonary disease, CKD; chronic kidney disease, DM; diabetes mellites.
Patients with CHF have a mean thrombocytes level equal to 185.26 /l, whereas, patients without CHF have a mean thrombocytes level 216.24 /l, which is statistically significant difference, t value - 2.15343, p< 0.033573.
Mean glucose level in diabetic patients equal to 9.93 mmol/l and in non-diabetic patients equal to 6.13 mmol/l, which is statistically significant difference, t value -7.9724, p< 0.0001. Coexistence of DM in patients increases the mean left ventricle wall thickness to equal 55.60 mm, whereas, in patients without DM, the mean left ventricle wall thickness to equal 51.42 mm, which is statistically significant difference, t value -2.5388, p< 0.012341. Mean erythrocytes sedimentation rate (ESR) in DM patients equal to 23.60 mm/hr, and equal to 17.43 mm/hr in non-diabetic patients, which is statistically significant difference, t value - 2.2236, p< 0.027887. Mean creatinine phosphokinase-MB fraction is dramatically higher in DM patients 233.36 U/L and lower in non-diabetic patients 66.05 U/l, which is statistically significant difference, t value --2.6267, p< 0.009726. Diabetic patients experience high level of triacyl glyceride (TAG) 2.17 mmol/l, whereas, non-diabetic patients had a lower TAG level 1.66 mmol/l, which is statistically significant difference, t value -2.5633, p< 0.011481. Hypertensive patients have a low mean level of red blood cells (RBC) level 4.55 /l in compare to non-hypertensive patients 7.7, which is statistically significant difference, t value -4.63276, p< 0.000010. In hypertensive patients, the mean LDH 1 is 608.21 U/l, INR is 1.05, sodium is 141.70 mmo/l, potassium is 4.04 mmol/l, and calcium is 1.14 mmol/l, whereas, in non-hypertensive patients, the mean level of LDH 1 is 908.8 U/l, INR is 2.1, sodium is 130.6 mmol/l, potassium is 14.8 mmol/l, calcium is 3.9 mmol/l, which is statistically significant difference; t value -2.07903, -3.04226, 2.51546, -3.62102, -3.19601; p< 0.040123, 0.002890, 0.013268, 0.000432, 0.001828, respectively.
CKD patients have high mean troponin I level equal to 22.70 ng/ml in compare to non-CKD patients 3.72 ng/ml, which is statistically significant difference, t value -6.84999, p< 0.0001. Also, CKD patients have higher mean level of CPK-MB fraction equal to 475.61 U/l in compare to non-CKD patients equal to 78.38 U/l, which is statistically significant difference, t value -3.63297, p< 0.000415. Mean creatinine level is higher in CKD patients 109.81 μmol/L comparing to non-CKD patients, which is statistically significant difference, t value - 3.63297, p< 0.000415.
Interestingly, COPD patients have a mean left ventricle wall thickness of 48.46 mm, which is less than non-COPD patients 52.73 mm, which is statistically significant difference, t value 1.99093, p< 0.048653. However, COPD patients have a mean right atrium wall thickness of 39.55 mm in compare to non-COPD patients 35.41 mm, which is statistically significant difference, t value -3.06986, p< 0.002632. Moreover, COPD patients have a mean RBC level equal to 145.29 in compare to non-COPD patients 136.39, which is statistically significant difference, t value -2.11854, p< 0.035948.
Patients with dyslipidemia have mean troponin I 9.4 ng/ml, whereas, patients without dyslipidemia have mean troponin I 3.64 ng/ml, which is statistically significant difference, t value -2.99785, p< 0.003316. Additionally, patients with dyslipidemia have mean total bilirubin 19.3 mmol/l, and 15.72 mmol/l in patients without dyslipidemia, which is statistically significant difference, t value -2.12114, p< 0.036358. Moreover, patients with dyslipidemia have a mean sodium serum level 132.3 mmol/l and a mean serum potassium level 8.4 mmol/l, whereas, in patients without dyslipidemia, the mean sodium serum level 142.24 mmol/l and a mean serum potassium level 4.07 mmol/l, which is statistically significant difference; t value 2.74875, -2.09792; p< 0.006966, 0.038083.
The mean leukocytes level in patients with varicose veins is 12.07 /l, whereas, in patients without varicose veins, the mean leukocytes level is 8.71 /l, which is statistically significant difference; t value -1.99832, p< 0.047801. The mean RBC level in patients with varicose veins is 9.87 /l, whereas, in patients without varicose veins, the mean RBC level is 4.56 /l, which is statistically significant difference; t value -6.88122, p< 0.000000. The mean ESR level in patients with varicose veins is 37.67 mm/hr, whereas, in patients without varicose veins, the mean ESR level is 18.25 mm/hr, which is statistically significant difference; t value -2.64654, p< 0.009161.
In terms of complications, patients with complications have been hospitalized for 14.65 days, whereas, patients without complications hospitalized for 11.40 days, which is statistically significant difference; t value 2.05492, p< 0.041657. In patients with complications, the mean aorta diameter 35.38 mm, whereas, in patients without complications, the mean aorta diameter 29.25 mm, which is statistically significant difference; t value 2.77454, p< 0.006278. In patients with complications, the mean right ventricle wall thickness 26.89 mm, whereas, in patients without complications, the mean right ventricle wall thickness 21.25mm, which is statistically significant difference; t value 2.44283, p< 0.015809. In patients with complications, the mean RBC level 4.87 /l, whereas, in patients without complications, the mean RBC level 12.40 /l, which is statistically significant difference; t value -5.37900, p< 0.0001. In patients with complications, in general urine analysis, microscopically, the mean urea proteins level 4.30, whereas, in patients without complications, the mean urea proteins level 50.00, which is statistically significant difference; t value -3.61867, p< 0.000419. In patients with complications, the mean potassium level 5.37 mmol/l and mean calcium level 1.58 mmol/l, whereas, in patients without complications, the mean potassium level 32.99 mmol/l and mean calcium level is 5.99 mmol/l, which is statistically significant difference; t value -3.75574, -2.05930; p< 0.000265, 0.041784, respectively.
Patients with post-MI CHF have mean myoglobulin level 199.90 ng/ml, whereas, in patients without post-MI CHF, the mean myoglobulin level 67.00ng/ml, which is statistically significant difference; t value 19.18246, p< 0.033158.
Patients with history of previous infarct have creatinine 90.48 μmol/l in compare to patients without reinfarction 78.01 μmol/l, which is statistically significant difference; t value 2.26506, p< 0.025056.
The mean age of patients with arrythmia is 65.58 years old, whereas, the mean age of patients without arrythmia is 59.68 years old, which is statistically significant difference; t value 3.32256, p< 0.001129. The mean height of patients with arrythmia is 173.67 cm, whereas, the mean height of patients without arrythmia is 168.61 cm, which is statistically significant difference; t value 2.23386, p< 0.034675. The mean ejection fraction (EF) of patients with arrythmia is 50.40 %, whereas, the mean EF of patients without arrythmia is 56.43 %, which is statistically significant difference; t value -3.81906, p< 0.000202. The mean left atrium wall thickness of patients with arrythmia is 42.14 mm, whereas, the mean left atrium wall thickness of patients without arrythmia is 39.12 mm, which is statistically significant difference; t value 3.00570, p< 0.003189. The mean right atrium wall thickness of patients with arrythmia is 37.36 mm, whereas, the mean right atrium wall thickness of patients without arrythmia is 34.95 mm, which is statistically significant difference; t value 2.96567, p< 0.003614. The mean CKP-MB of patients with arrythmia is 181.82 U/l, whereas, the mean CKP-MB of patients without arrythmia is 56.68 U/l, which is statistically significant difference; t value 2.34423, p< 0.020643. The mean lactate dehydrogenase (LDH) serum level of patients with arrythmia is 888.37 U/l, whereas, the mean lactate dehydrogenase serum level of patients without arrythmia is 533.49 U/l, which is statistically significant difference; t value 3.16430, p< 0.002039. The mean aspartate transaminase serum level of patients with arrythmia is 71.53 mmol/l, whereas, the mean lactate dehydrogenase serum level of patients without arrythmia is 47.38 mmol/l, which is statistically significant difference; t value 2.23750, p< 0.026893.
The mean EF of patients with aneurysm is 43.00 %, whereas, the mean EF of patients without aneurysm is 55.59 %, which is statistically significant difference; t value 4.57958, p< 0.000010. The mean leukocytes level in patients with aneurysm is 9.70 /l, whereas, the mean leukocytes of patients without aneurysm is 2.11 /l, which is statistically significant difference; t value -3.83162, p< 0.000192. The mean epithelial cell level in general urine analysis in patients with aneurysm is 5.40, whereas, the mean epithelial cell level in patients without aneurysm is 1.58, which is statistically significant difference; t value -4.41313, p< 0.000021. The mean thickness of the left atrium of patients with pericarditis is 45.5mm, whereas, the mean thickness of the left atrium of patients without pericarditis is 39.90 mm, which is statistically significant difference; t value -2.01849, p< 0.045598. The mean creatinine level of patients with pericarditis is 52.5 μmol/L, whereas, the mean creatinine level of patients without pericarditis is 82.39 μmol/L, which is statistically significant difference; t value 1.98986, p< 0.048568.
Patients with pneumonitis have mean aorta diameter of 20.00 mm, whereas, the mean aorta diameter of patients without pneumonitis is 35.32 mm, which is statistically significant difference; t value 3.55083, p< 0.000524. Patients with pneumonitis have mean serum leukocytes level of 14.80 /l, whereas, the mean serum leukocytes level of patients without pneumonitis is 8.70 /l, which is statistically significant difference; t value -2.11170, p< 0.036527. Patients with pneumonitis have mean ESR level of 48.00 mm/hr, whereas, the mean ESR level of patients without pneumonitis is 18.47 mm/he, which is statistically significant difference; t value -2.36894, p< 0.019267. Moreover, patients with pneumonitis have mean urine leukocyte level of 22.00, whereas, the mean urine leukocyte level of patients without pneumonitis is 2.53, which is statistically significant difference; t value -3.15623, p< 0.001963. The mean CKP-MB in patients with pneumonitis 1164.00 U/l, whereas, the mean CKP-MB of patients without pneumonitis is 89.60 U/l, which is statistically significant difference; t value -3.92161, p< 0.000144.
The mean aorta diameter, EF, EDV, troponin I, CKP-MB, APTT in patients with elevated troponin T is 28.00 mm, 36.00 %, 62.00 ml, 33.00 ng/ml, 2881.00 U/l, and 49.10 sec, respectively. Whereas, the mean aorta diameter, EF, EDV, troponin I, CKP-MB, APTT in patients without elevation in troponin T is 35.31 mm, 54.68%, 134.95 ml, 4.51 ng/ml, 75.26 U/l, 27.01 sec, respectively, which is statistically significant difference; t value 2.3478, 2.0136, 2.0775, -3.6144, -19.3413, -2.5572, p< 0.020266, 0.045967, 0.040063, 0.000436, 0.000000, 0.012661, respectively.
The mean age of patients with elevated D-dimer level is 68.14 years old, and mean age of patients with normal D-dimer is 56.60 years old, which is statistically significant difference; t value 2.25820, p< 0.047513. The mean wall thickness of the right ventricle of patients with elevated D-dimer level is 25.93 mm, and mean wall thickness of the right ventricle of patients with normal D-dimer is 29.40 mm, which is statistically significant difference; t value - 2.35428, p< 0.040345.
Comparing the dependent variable shows no statistical differences. (Figure 3)

graphical presentation for the dynamical changes in the levels of LDH (lactate dehydrogenase) and CPK-MB (creatinine phosphokinase-MB fraction. Both LDH and CPK-MB fraction measured by U/L. this analysis conducted between two days for all patients as a follow up after MI.
In terms of correlations, a full table shows the correlation between all the continuous variables is presented. (Table 2)
An interesting correlation between the LDL level and the diameter of the aorta basement has been seen. (Figure 4) It has been shown that when the left ventricle wall thickness increases the EF dramatically decrease. (Figure 4)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A direct correlation between LDL level and the aorta diameter. Additionally, an opposite correlation between the left ventricle (LV) wall thickness and the EF.
Discussion
Post-MI changes include early and late pathophysiological changes, early post-MI complications include ventricular rupture, aneurism, arrythmia, sudden cardiac arrest and death [11–13]. However, the late changes include pericarditis, pneumonitis, pleuritis, and post infarction cardiosclerosis and dyskinesia [14, 15]. Such manifestations are associated with some laboratory and instrumental changes. Assessment of these changes help prevention or slow down, or at least make a prognosis for the MI patients. Low level of thrombocytes in patients with concomitant CHF return to the use of anti-aggregatnts and anticoagulants for a long time.
High leukocytes level in diabetic patients endorses the hypothesis of chronic mild inflammatory syndrome in patients with metabolic syndrome [16–19]. The high TAG values in diabetic patients is due to the lipogenesis from high glucose serum levels and metabolic disorders associated with the chronic lipid peroxidation and biogenesis disorders [16, 20].
The dramatic increase in the wall thickness of patients with COPD is an indicator of a stable stage of pulmonary heart, which is associated with pulmonary hypertension and blood stagnation in the pulmonary circulation [21, 22]. Typically, these patients experience cough and shortness of breath on the background of distress syndrome, fluid accumulation in the pulmonary tissue, and impaired ability of the pneumocytes for gas exchange. As a compensation for the respiratory hypoxemia, the elevation in the levels of the erythropoietin and the further erythropoiesis elevation, which is demonstrated in the high level of Hb in COPD patients.
Leukocytosis is seen in patients with varicose vein is indicator of the persistent inflammation with elevation in the tissue hypoxia and further elevation in hypoxia inducing factor to stimulate the erythropoietin production and further increasing in the RBC level in patients with varicose veins [23, 24]. This persistent inflammation is confirmed by the elevation in the ESR level in patients with varicose veins [25–28].
Post MI complications reported in 4/5 of the sample and these complications associated with some laboratory and instrumental changes. Suggesting that post MI laboratory changes are not limited to the local myocardial infarction changes to involves systemic manifestations such as kidney function impairment or development of new kidney disease. Of these changes include increase in the aorta basement diameter, increase in the right ventricle wall thickness, decrease in the level of RBC, serum potassium level, and serum calcium level, with increase in the serum myoglobulin.
Re-infarct worsens the kidney function and induces renal failure [29–32]. Aging is a risk factor for MI and arrythmia development. Arrythmia increases CPK-MB, LDH, AST, wall thickness of both atriums, and decrease EF. The higher the troponin level the less EF and the poorest further sequalae.
Early post-MI aneurysm significantly impairs the cardiac output and further reduces the systemic systolic blood pressure. These changes are associated with the reduction in the blood flow in to the renal afferent fibers, which are sensed by the juxtaglomerular apparatus that leads to activation the renin angiotensin aldosterone system with the anti-diuretic hormone. Therefore, reduction in the kidney function is seen in MI patients. Additionally, elevation of creatinine in aneurysm patients is typical for impaired kidney function particularly filtration due to hypoperfusion of the glomeruli.
Patients with pneumonitis are having a high leukocyte in serum and in the urine, high ESR, and high CKP-MB fraction. However, these patients experience small diameter of the aorta basement.
Conclusions
The early prognostic value of the instrumental and laboratory changes is complication dependent. With age increase the level of D-dimer and thrombocytes. The higher the troponin level the less EF and the poorest further sequalae. Systemic manifestations include kidney function impairment or development of new kidney disease. Of these changes include increase in the aorta basement diameter, increase in the right ventricle wall thickness, decrease in the level of serum red blood cell, serum potassium level, and serum calcium level, with increase in the serum myoglobulin.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Declarations
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study approved by the National Research Mordovia State University6 Russia, from “Ethics Committee Requirement N8/2 from 30.06.2022”.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the participants for publication of study results and any accompanying images.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
Footnotes
Competing interests: No competing interests regarding the publication.
All authors read and approved the final version of the manuscript
Postal address: Russia, Mordovia republic, Saransk, Bolshevitskaya Street, 31, 430005
List of abbreviations
- CHF
- chronic heart failure
- DM
- Diabetes mellitus
- CKD
- Chronic kidney disease
- COPD
- Chronic obstructive pulmonary disease
- MI
- myocardial infarction
- HR
- heart rate
- ESR
- erythrocytes sedimentation rate
- RBC
- red blood cells
References
{kind=link}



