
ABSTRACT
The reduced prevalence of insulin resistance and type 2 diabetes (T2D) in countries with endemic parasitic worm infections suggests a protective role for worms against metabolic disorders, however clinical evidence has been non-existent. This 2-year randomized controlled trial of hookworm infection in 40 people at risk of T2D involved treatment with either 20 or 40 Necator americanus third-stage larvae (L3) or Placebo. Primary outcome was safety, with homeostatic model assessment of insulin resistance (HOMA-IR), fasting blood glucose (FBG), and body mass being the key metabolic outcomes. Adverse events were more frequent in hookworm-treated participants, where 44% experienced transient gastrointestinal symptoms. FBG and HOMA-IR were significantly lowered in both hookworm-treated groups at 1-year, and body mass was significantly lowered after L3-20 treatment at 2-years. Overall, hookworm infection was well tolerated in people at risk of T2D, and were associated with improved insulin resistance, warranting further exploration of the benefits of hookworms on metabolic health.
Metabolic syndrome (MetS) represents a collection of related metabolic conditions, including dysregulated lipid homeostasis, hypertension, insulin resistance, and abdominal obesity, that increase the likelihood of developing chronic diseases such as type 2 diabetes mellitus (T2D) and cardiovascular disease1. T2D is a complex illness associated with hyperglycemia; long-term and costly medical care is usually required to prevent complications. The prevalence of T2D is increasing globally, with more than half a billion adults already diagnosed2; hence there is a pressing need to develop new preventative approaches to limit the burden of T2D on individuals and health systems.
The soaring global prevalence of T2D is undoubtedly related to lifestyle factors such as an energy-dense diet and a sedentary lifestyle. In this context, the detrimental role of systemic, low-grade inflammation in promoting insulin resistance is well-established 3. In lean adipose tissue, there exists an anti-inflammatory environment, including regulatory T cells, eosinophils, and alternatively activated macrophages that are stimulated by Type 2 cytokines such as interleukin (IL)-4, IL-5, and IL-13. Conversely, in obesity there is a pro-inflammatory milieu involving Type 1 cytokines such as IFNγ and TNF, classically-activated macrophages4, and a dysregulated gut microbiome 5. This biased Type-1 immune response aggravates insulin resistance through stress-activated kinases that target intermediates in the insulin-signaling pathway6. It follows that maintaining the systemic and adipose-specific inflammatory balance in favor of a Type 2 or regulatory immune response is a rational approach to limiting the inflammatory cascade and preventing the ensuing insulin resistance seen in metabolic disease.
Parasitic helminths (worms) co-evolved with humans and remain endemic in regions of the world with less metabolic and inflammatory diseases 7–10. Helminth infections are associated with Type 2 immune responses such as eosinophilia, elevated IL-4, −5 and −13, Type-2 innate lymphoid cell responses, and modulation of the gut microbiome11. Emerging evidence supports the hypothesis that eradicating worms from industrialized regions may have partly contributed to the increased prevalence of immune-mediated diseases such as T2D8, 12. For example, human epidemiological studies suggest that the presence of helminth infections is associated with lessened inflammatory responses and improved glucose homeostasis12, 13, 10, and two systematic reviews and meta-analyses concluded that adults with previous or current worm infection typically enjoy improved metabolic function14, 15. While cross-sectional studies support the idea of a protective role for worms in metabolic disease, they did not establish causality.
Recent deworming studies provided some causative evidence. The removal of worms from previously-infected individuals was associated with increased insulin resistance (elevated homeostatic model assessment for insulin resistance, HOMA-IR) 16, elevated serum insulin and glucagon 17, enhanced hyperglycaemia and risk of metabolic disease 18, and worsened blood lipid profiles 19. Experimental mouse studies corroborate findings from human studies, where infection with various worm species caused improvements in metabolic indices, Type 2 immune responses, and alterations to the gut microbiome20, 21–24. However, to date, there have been no studies in humans testing whether a controlled helminth infection is safe, can improve metabolic health, and potentially prevent progression to T2D.
Previously, we and others have established the safety of infecting human volunteers with low doses of hookworms in various inflammatory diseases 25–27. While none of these studies investigated metabolic health outcomes, it is well reported that hookworms elicit Type 2 and regulatory immune responses 26 and changes in the microbiome 28 that may be beneficial in the context of T2D. The primary aim of this randomized, double-blinded, placebo-controlled Phase 1b clinical trial was to establish the safety, tolerability, and potential metabolic benefits of experimental infection with infective third-stage larvae (L3) of the human hookworm Necator americanus in otherwise healthy adults at risk of developing metabolic syndrome and T2D. Based on previous animal and deworming studies, we hypothesized that hookworm infection would be safe and improve the primary metabolic outcome for the study, HOMA-IR, which assesses longitudinal changes in insulin sensitivity that correlate well with estimates derived via the euglycaemic clamp 29.
RESULTS
Study population
We conducted a 2-year Phase Ib randomised, double-blinded, placebo-controlled trial of experimental hookworm infection (either 20 or 40 infective third-stage larvae, L3) in otherwise healthy people at risk of T2D (Figure 1A). Recruiting progressed between January 2018 and June 2020, with 85 potential participants meeting screening criteria, of which 41 met the inclusion/exclusion criteria to proceed to randomization (4 short of the recruitment target). Forty-four participants were excluded due to not having elevated baseline HOMA-IR (n=27), not responding to communication (n=11) or excluded medications or medical conditions (n=6) (Figure 1B). One participant who qualified for the study dropped out prior to their baseline visit. Forty participants were randomised and constituted the intention-to-treat (ITT) population (Table 1). Thirteen participants were allocated to receive Placebo treatment, 14 to receive a dose of 20 hookworm larvae (L3-20) and 13 to receive a dose of 40 hookworm larvae (L3-40). (Figure 1B). The majority of participants (85%) were of Caucasian descent. Baseline age and HOMA-IR were higher in the L3-20 group. One participant who was randomized into the Placebo group unintentionally received an L3-20 treatment due to a labelling error. This participant was included in the Placebo group for the ITT analysis but in the L3-20 group for per-protocol analyses.

(A) After screening and informed consent, participants were allocated to receive either placebo (chilli pepper solution) or a total of 20 (L3-20) or 40 (L3-40) N. americanus hookworm larvae delivered to the skin over 2 occasions, at month 0 and month 2. Participants underwent evaluation visits every 6 months, where physical and vitals exams were undertaken, adverse events were reviewed, and biological samples and questionnaires were collected for analysis of safety, pathology, well-being, diet and exercise habits. (B) CONSORT chart showing flow of patients through the clinical trial, and reasons for early termination. (C) Kaplan Meier analysis of rates of trial continuation (%) in each group during the 2-year study.
Intention to Treat Baseline Characteristics for all Randomised Participants (n=40)
Adverse events (AEs)
The study’s primary outcome was the safety and tolerability of hookworm treatment, defined by the frequency and severity of AEs. A total of 20 AEs and no serious AEs were reported (Table 2). As expected, gastrointestinal (GI) adverse events occurred in the L3-20 and L3-40 treatment groups (Table 2), consistent with the worms arriving in the gut and attaching to the intestinal wall. These AEs were experienced by 44% of hookworm-treated participants and included bloating, nausea, vomiting, constipation, diarrhoea, epigastric upset, hungry feeling, stomach cramps and abdominal pain, which were typically mild-moderate and resolved without medical intervention. One GI-related symptom (5%) was recorded as severe, and three warranted early removal of the participants from the study (1 in the L3-20 group, 2 in the L3-40 group) and provision of deworming medication. Two of these individuals recovered promptly after deworming, while symptoms in one participant persisted, indicating their symptoms may have been unrelated to hookworm. No GI-related AEs occurred in the Placebo group. No participant developed anaemia (Supplementary Figure 1), the primary clinical effect of moderate to heavy hookworm infection. AEs deemed unrelated to worm infection were reported across all groups and included one case each of concussion, laryngitis, appendicectomy, gynaecological procedure, salmonella infection acquired overseas, breast cancer diagnosis, erythema, and dermatitis. The chi-square test for trend revealed a significant linear trend for AEs, χ2 (1, N = 40) = 3.846, p = 0.049 with more AEs occurring in the hookworm treatment groups compared to the Placebo group, as anticipated based on studies in other patient populations 30.

Blood hemoglobin concentration at each evaluation visit (median and IQR), shaded area indicates combined normal range for males and females.
Summary of the number of adverse events (AE) and proportions of participants experiencing at least one AE, classified by AE type and symptom severity
Study Progression and well-being
Rates of trial completion and participant mood and well-being were secondary safety outcomes. The CONSORT Flow Diagram (Figure 1B) and Kaplan-Meier curve (Figure 1C) detail study progression. Early dropouts (0-6 months) included the 3 participants with GI symptoms and one participant in the L3-20 group that was removed from the study at 3 months due to an unrelated cancer diagnosis (Figure 1B). Reasons for early terminations later in the study included 4 participants moving away (Placebo n=2, L3-20 n=1, L3-40 n=1), 1 for undisclosed personal reasons (L3-20), 3 for failure to respond to communication or testing exhaustion (Placebo n=2, L3-40 n=1), and 4 for starting medication (L3-20, n=1) or undergoing gastric sleeve surgery (Placebo n=1, L3-20 n=2) that could interfere with the trial outcomes. Four participants (Placebo n=1, L3-20 n= 1, L3-40 n=1) missed one evaluation visit each but completed the remaining evaluation visits. Twenty-four of the 40 randomised participants completed the trial, including 8 (62%) in the Placebo, 7 in the L3-20 (50%), and 9 in the L3-40 group (69%). The difference in study completion between groups was not significant (Figure 1C, Log-rank test for trend, p=0.832). Monitoring of participant mood and depressive state via the Patient Health Questionnaire-9 (PHQ-9) questionnaire revealed that median scores in the Placebo group remained relatively stable throughout (Table 3). There was a trend for reduced median PHQ-9 scores (suggestive of improved mood) compared to baseline in both hookworm treatment groups at all evaluation visits; however, Mixed-effects model analyses and Kruskal-Wallis tests did not detect any significant differences over time or between groups, even when the active hookworm treatment groups were combined (Mann-Whitney test) (Table 3).
Patient Health Questionnaire scores in each treatment group
Analysis of potential confounding variables: diet and exercise habits
Participants completed regular questionnaires to record any changes in diet and exercise habits that could confound results. Analysis of the diet questionnaire (PREDIMED) revealed no significant inter-cohort differences or longitudinal changes in PREDIMED score in any treatment group (Supplementary Figure 2A). Similarly, analysis of the exercise habits of participants by quantifying their median numbers of metabolic equivalent of tasks (METs) per week revealed no significant changes within groups from baseline and no significant differences in median absolute METs/week or changes in METs/week between groups at any time point (Supplementary Figure 2B).

(A) PREDIMED total scores in each treatment group at each evaluation visit (median and IQR). (B) Physical activity (Metabolic Equivalents of task, METs) per week assessed at each evaluation visit (median and IQR).
Evaluation of hookworm establishment
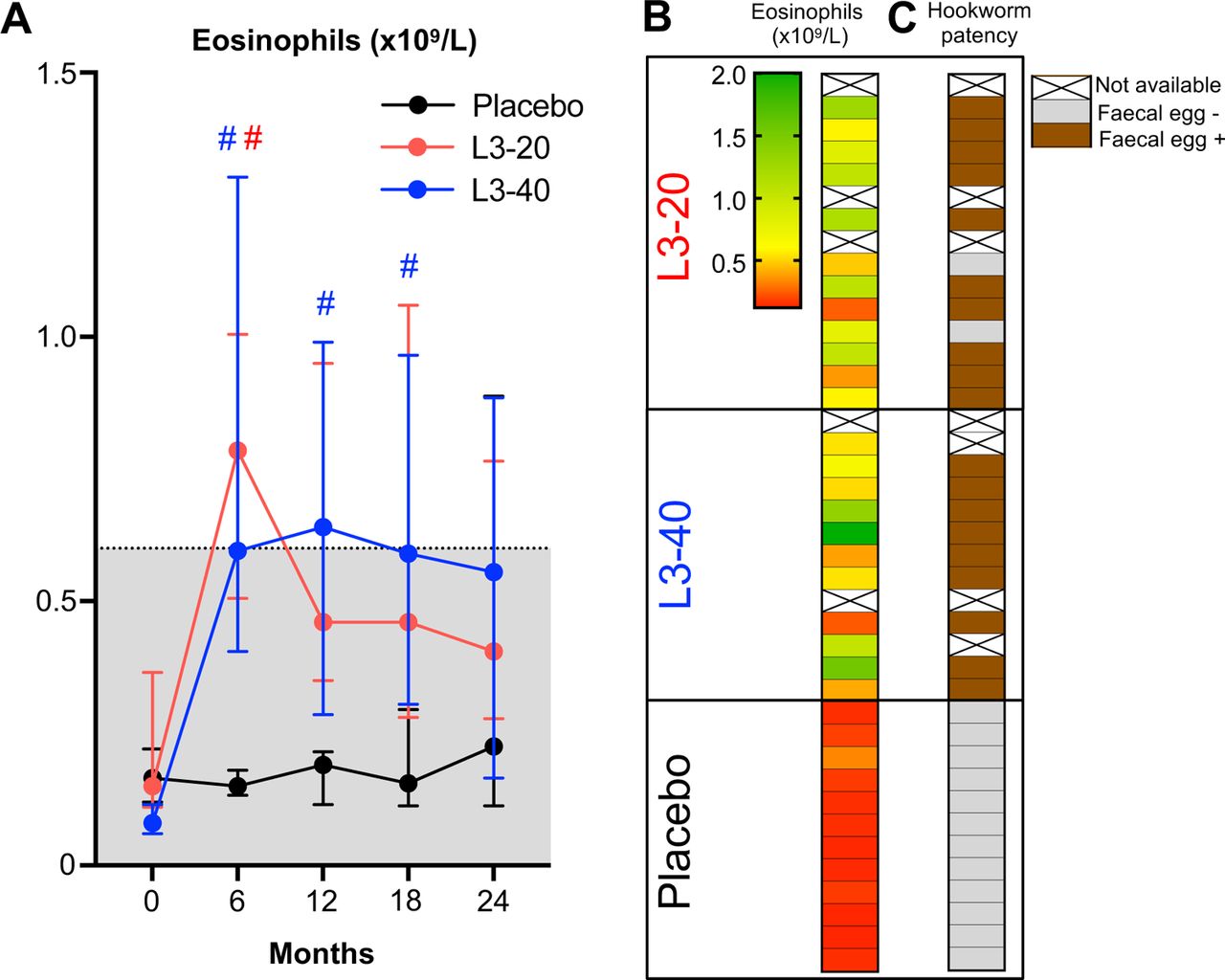
Hookworm infection is associated with the presence of hookworm eggs in stool and peripheral blood eosinophilia. As expected, eosinophil counts remained stable in the Placebo cohort (Figure 2A), and faecal samples were negative for hookworm ova (Figure 2C). In both the L3-20 and L3-40 groups, eosinophil counts were significantly elevated from baseline by 6 months (L3-20 p = 0.047, L3-40 p= 0.002, Tukey’s posthoc test) (Figure 2A). Of the 28 hookworm-treated participants, five faecal samples were unavailable for qPCR testing due to early dropout or inability to deliver a faecal sample. Twenty-one of the 23 participants (91%) tested positive for N. americanus ova (Figure 2C), and the two participants that tested negative still displayed robust increases in eosinophil counts (Figure 2B).

(A) Peripheral blood eosinophil counts (median ± IQR) at each evaluation visit, shaded area indicates normal range. (B) Heat map displaying eosinophil counts the 6 month visit (peak eosinophilia) in each participant and correlation with the (C) detection of hookworm eggs in feces by qPCR (Hookworm patency). Some samples were unable for analysis due to droppoing out prior to the 6-month visit.
Primary metabolic outcome: Insulin resistance (HOMA-IR)
We undertook a per-protocol analysis of metabolic outcome measures to account for the Placebo participant who received hookworm treatment in error. Data collected from the 4 participants described in the Study Progression section who, at 18 or 24 months, were retrospectively discovered to have undertaken gastric sleeve surgery or began taking metformin were excluded from the analysis. Data from one L3-20 participant whose insulin (47 mU/L), glucose (12.4 mmol/L) and HOMA-IR (26 units) values at 6 months were well beyond normal ranges and inconsistent with fasting were also excluded.
The trial’s primary metabolic outcome was the effect of hookworm treatment versus placebo on insulin resistance, as assessed by changes in HOMA-IR. Median HOMA-IR values in the Placebo group fluctuated between improved and worsened from the baseline value of 2.2 [2.0-2.6], reaching a maximum of 2.9 [1.8-4.2] at 12 months, corresponding to a median increase of 0.8 units [−0.7 to 2.3] (Table 4 and Figure 3A). In contrast, median HOMA-IR value in the L3-20 group was significantly lowered from the baseline value of 3.0 [2.3-3.6] to as low as 1.6 [0.9-3.0] at 18 months (p=0.028 Tukey’s post-hoc test). Median change in HOMA-IR values in the L3-20 group was significantly different from Placebo at 12 months (p=0.039, Kruskal Wallis), with a reduction of 1.1 units [−1.5 to −0.5] from the baseline value. Similar trends toward lowered HOMA-IR values were observed in the L3-40 group at 6 months (−0.5 units [−1.2 to 0.2]) and 12 months (−0.4 units [−1.4 to 0.9]); however, these changes were not statistically different from Placebo at any evaluation visit. Since significance tests depend greatly on sample size, and numbers in all groups were low, we calculated the effect sizes of treatment versus control to measure the treatment effect independent of participant numbers. Effect sizes for HOMA-IR changes in the L3-20 versus Placebo group were medium at 6 months (d=0.76) and large at 12 months (d=1.24), 18 months (d=1.01) and 2 years (d=1.03). For the L3-40 group, effect sizes were moderate at 6 months (d=0.55) and 12 months (d=0.75) and negligible at 18 months (d=0.25) and 2 years (d=-0.15) (Supplementary Table 1).
HOMA-IR change effect sizes at each evaluation visit

Changes in the (A) Homeostatic model assessment of insulin resistance (HOMA-IR, units), (B) Fasting blood glucose and (C) fasting blood insulin levels from baseline values at each 6-monthly evaluation visit. Violin plots display each individual data point, median and IQR. Dotted vertical line indicates baseline levels (0 change). *Significant difference to placebo, # Significant difference to baseline value.
Absolute values and changes in HOMA-IR, fasting blood glucose and insulin in each treatment group
Metabolic outcomes: Fasting blood glucose, insulin and glycated haemoglobin
Median FBG levels (mmol/L) in the Placebo group were stable throughout and did not significantly deviate from their starting values (p=0.132, Mixed-effects model analysis) (Table 4 and Figure 3B). In contrast, median FBG levels were significantly reduced from baseline levels after 6 months in both the L3-20 (baseline: 5.2 [4.7-5.6] to 6 months: 4.5 [4.0-5.1]; p=0.045) and L3-40 groups (baseline: 5.3 [4.9-5.4] to 6 months: 4.3 [4.0-5.3]; p=0.016). Similar significant reductions in FBG were seen in the L3-40 group at 12 months (p= 0.007) and 2 years (p=0.015) compared to baseline; however reductions in the L3-20 group were not statistically significant at any other time point (12 months p=0.184, 18 months p=0.069, 2 years p=0.052). Median changes in FBG levels in the L3-20 treatment group were not significantly different to Placebo at any time point, but changes in the L3-40 group were significantly different to Placebo at 6 months (−0.7 in L3-40 compared to 0.0 in Placebo; p=0.027) and 12 months (−1.0 in L3-40 compared to +0.3 in Placebo; p=0.024).
Fasting insulin levels (mU/L) were stable in the Placebo group throughout the study, ranging from a baseline of 11 [9-12] to a maximum of 12 [10-15] at 6 months (Table 4 and Figure 3C). There were no longitudinal changes in insulin levels in the L3-40 group at any time point and no significant differences compared to Placebo. Insulin levels in the L3-20 group were consistently lowered from the baseline level of 13 [12-16] to a minimum of 9 [5-14] at 18 months (p=0.043 compared to baseline), with reductions from baseline values reaching statistical significance compared to Placebo at 12 months (−4.0 in L3-20 compared to +2.0 in placebo; p=0.02).
Levels of glycated haemoglobin (HbA1cIFCC, mmol/mol) displayed an upward trend at all evaluation visits compared to baseline in the Placebo group, ranging from a baseline value of 32 [30-33] mmol/mol to a maximum of 35 [33-37] at 2 years (Supplementary Table 2). Values in the L3-20 group were stable near the baseline value of 33 [30-35] throughout, while values in the L3-40 group experienced similar upward trends to the Placebo group, with values significantly higher than baseline at 18 months (p=0.027).
Absolute values and changes in glycated haemoglobin (HbA1c/IFCC) in each treatment group
Secondary metabolic outcomes: Body mass and blood lipid profile
Median body mass and Body Mass Index (BMI) in the Placebo group remained stable throughout (Table 5, Figure 4 and Supplementary Figure 3). While there were no statistically significant differences in body mass or BMI in the L3-20 or L3-40 groups compared to Placebo (Table 5), body mass and BMI in the L3-20 group tended to be lower than their baseline values at all evaluation visits, with significant reductions in body mass and BMI in the L3-20 group at 18 months (p=0.019 for body mass, p=0.028 for BMI) and 2 years (p=0.031 for body mass and p=0.032 BMI). This corresponded to a median reduction in body mass of approximately 5kg at both time points in the L3-20 group (Table 5 and Figure 4) and a reduction in BMI of 2.2 units and 2.4 units at 18 months and 2 years, respectively (Table 5 and Supplementary Figure 2). No significant longitudinal changes in body mass or BMI were evident in the L3-40 group.

Changes in participant’s body mass index (kg/m2) from baseline values at each 6-monthly evaluation visit. Violin plots display each individual data point, median and IQR. Dotted vertical line indicates baseline levels (0 change). # Significant difference to baseline value.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in participant’s body mass (kg) from baseline values at each 6-monthly evaluation visit. Violin plots display each individual data point, median and IQR. Dotted vertical line indicates baseline levels (0 change). # Significant difference to baseline value.
Body mass and Body Mass Index (BMI) absolute values and changes in each treatment group
Analysis of blood lipid profile revealed that median levels of total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein and total cholesterol/HDL ratio remained relatively stable in the Placebo group at all time points, with only a statistically significant reduction in LDL (p=0.009) and total cholesterol at 18 months (p=0.037) (Supplementary Tables 3 and 4). In both the L3-20 and L3-40 groups, there were no longitudinal changes in any of these parameters compared to baseline and no significant differences compared to Placebo other than elevated LDL (p=0.019) and total cholesterol (p=0.038) at 18 months in the L3-40 group compared to Placebo (Supplementary Tables 3 and 4).
Absolute values and changes in serum cholesterol, high-density lipoprotein (HDL) and cholesterol/HDL ratio in each treatment group
Absolute values and changes in serum Triglyceride and Low-Density Lipoprotein (LDL) levels in each treatment group
DISCUSSION
Over recent decades, helminth infection has emerged as a potential approach for treating allergic and autoimmune disorders, as well as metabolic disorders such as MetS and T2D15, 21, 27. Until now, a potential supportive role for worms in metabolic health has relied on animal studies and human cross-sectional or deworming studies that could not infer causality. The present study provides the first reported controlled-trial clinical evidence for the beneficial effect of helminth infection in metabolic disease. Infection with low doses of hookworms caused significantly reduced measures of glucose homeostasis (lowered HOMA-IR and fasting blood glucose) compared to pre-infection and Placebo treatment, which was associated with modest body mass reductions. Diet and physical activity changes could not explain these improvements. While the study was relatively small and needs to be validated by larger follow-up studies, the results provide critical proof of principle that hookworms and/or the biological changes they invoke in their human hosts are a safe and potentially beneficial intervention for improving determinants of metabolic health and preventing the development of T2D.
The primary outcome of this Phase Ib study was to determine the safety and tolerability of hookworm infection in people at risk of developing T2D. While hookworm infection was associated with a higher incidence of gastrointestinal AEs, these were anticipated during the time that hookworms established in the gut30 and were typically mid-moderate and resolving. Three of the 28 hookworm-treated participants displayed GI symptoms that warranted deworming, and symptoms resolved promptly in two. The third did not improve after deworming, suggesting their symptoms were unrelated to hookworm infection. Overall, the safety profile of hookworm treatment in people at risk of T2D is similar to that in other diseases 30.
In the current study, hookworm infection was associated with improved insulin resistance, consistent with previous mouse or natural human helminth infection studies 7, 21, 31. Lowered HOMA-IR was most apparent in the group that received 20 hookworms and was most pronounced at 18 months, with a reduction in median HOMA-IR from 3.0 units at baseline (consistent with pre-diabetic insulin resistance) to 1.6 units at 18 months (a healthy level). The large Cohen’s d effect sizes in the L3-20 group highlight the statistical and clinical significance of this sustained improvement in metabolic health. Interestingly, the improvements in HOMA-IR in the group that received 40 worms were less dramatic, despite similar trends in reduced HOMA-IR at 6 and 12 months. Both the L3-20 and L3-40 groups showed similar reductions in fasting blood glucose compared to Placebo throughout the study, but only the L3-20 group displayed sustained reductions in insulin. By the later stages of the study, all results from the L3-40 group were comparable to Placebo, indicating that a higher worm dose did not yield superior improvements in insulin resistance. This is somewhat counter-intuitive, but larger clinical trials are required to clarify the optimal dose of hookworms. One factor that may partially explain why participants in the L3-20 cohort responded better to treatment was that pre-trial median age and HOMA-IR were higher; hence there was greater potential for improvements. Future clinical trials designed to demonstrate efficacy should stratify participants based on high and low baseline HOMA-IR.
In conversations with potential participants during recruitment and screening, it was evident that a powerful motivator to enrol was the prospect of body mass reductions, as documented in mouse20–22, 24 or natural human helminth infection studies7, 24, 31, 32. We noted modest reductions in body mass and BMI in the L3-20 group; however, body mass reductions were not consistent for all hookworm-treated participants, possibly due to the relatively low worm burdens compared to those seen in animal studies or natural infections. This caused disappointment for some people, who then elected to pursue gastric sleeve surgery despite improvements in HOMA-IR. Most participants were less concerned and continued with unabated enthusiasm. Bar one, all hookworm-treated participants that completed the study opted to retain their worms, and the sole person who dewormed did so in preparation for a medical procedure.
Interestingly, hookworm infection did not improve blood lipid profiles in contrast to what may have been expected based on previous studies 9, 10, 13, 24, 32. A potential explanation could lie in the different helminth species used in the current trial. Previous studies noting improved blood lipid markers included cross-sectional and deworming studies of infections with multiple soil-transmitted helminths 32 and previous and current schistosomiasis 9, 10, 13, 24 but not hookworm infection alone. Results from a 2019 systematic review and meta-analysis suggested that different helminth species may have different efficacy in altering lipid and glucose homeostasis15. The authors postulated that the liver-specific residence of Schistosoma spp. compared to intestinal helminths could facilitate greater metabolic improvements in schistosomiasis. Future helminth challenge studies such as ours that instead use single-sex infections with schistosome parasites 33 may validate this hypothesis.
The study had several limitations, with the major shortcoming being the small sample sizes that limited our ability to make firm conclusions. This was further curbed by the long duration of the study and attrition of participants in all groups after the 12-month time point. Since T2D takes many years to manifest, future studies will need to follow up with participants for longer periods. Ideally, this would be combined with repeated doses of hookworms to maintain a chronic infection and monitoring of the associated immune response. Such studies could include a deworming arm to determine if an active hookworm infection is required for longer-term benefits and could use HbA1c IFCC as a longer-term primary outcome measure of improved glycaemic control.
Further, participant selection bias limited the generalizability of our findings. Most participants were of Caucasian descent, and it is unclear if different populations, such as people of Asian descent or Australian First Nations people, who disproportionately suffer from MetS and T2D 34, would experience similar improvements. Lastly, within the scope of this study, we could not attain a mechanistic understanding of how and why hookworm infection caused improvements in insulin resistance. Type 2 immune responses and eosinophils are known to influence metabolism20, 35, so it remains plausible that they contributed to stimulating this pathway. Better understanding of the beneficial biological effects of hookworms in the context of MetS may identify novel therapeutic strategies that could mimic the actions of the live hookworm (e. g. immune-modifying or microbiome therapies) or may pinpoint factors that are excreted/secreted by hookworms that could be produced as novel biologic therapies 36.
In conclusion, the hygiene hypothesis8, 12 provides a persuasive explanation for the increasing prevalence of inflammatory and metabolic disorders in populations with a low prevalence of helminth infections. The present study is the first to demonstrate that experimental infection with low hookworm doses is safe and leads to clinically significant improvements in glucose homeostasis in people at risk of MetS and T2D. Results from this proof of concept study will inform the further development of novel preventative interventions in humans at risk of T2D.
METHODS
Study design and regulatory approvals
Between January 2018 and April 2022, we conducted a 2-year Phase Ib randomised, double-blinded, placebo-controlled trial of experimental hookworm infection (either 20 or 40 infective third-stage larvae, L3) in otherwise healthy people at risk of T2D. The study included two clinical sites in Queensland, Australia (James Cook University Cairns and Townsville campuses). The study designated C26 was approved on April 19th 2017 by the Human Research Ethics Committee of James Cook University. The trial was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12617000818336). The clinical study protocol was published in 2019 37.
Participants and sample collection
Inclusion criteria: Otherwise healthy males and females aged 18-50 years with central obesity (waist circumference> 90cm for women and >102cm for men) and increased insulin resistance as assessed via abnormal HOMA-IR>2.12 or at least two other features of metabolic syndrome determined at screening (blood pressure>135/85 mmHg, dyslipidaemia or abnormal liver function tests). Exclusion criteria, in brief, included pregnancy, established chronic disease, historical or current substance abuse, major allergies, known immunodeficiency disorder, unstable asthma or taking medications likely to interfere with study outcomes. Blood samples were taken at each 6-monthly visit into serum separator tubes for serum analyses or heparin-coated tubes for complete blood count analysis (Beckton Dickinson). Participants were asked to provide fresh faecal samples at each study visit, which were frozen at −80°C for future analysis of the presence of hookworm eggs by qPCR.
Randomization and masking
An initial recruitment target of 54 participants allowed for a dropout rate of 20%, leaving a desired recruitment target of 45 volunteers (15 in each treatment group) to participate in the trial. Volunteers who met the eligibility criteria and had given informed consent were randomly allocated on a 1:1:1 ratio according to a computer-generated sequence to one of the three study arms: Placebo, 20x N. americanus L3 (L3-20) or 40x L3 (L3-40). Participants and investigators were blinded to the treatment, other than the assigned producer of the inocula (co-author L.B.).
Preparation and administration of treatments
The inocula were prepared freshly as previously described 38. Hookworm ova were collected from two volunteer donors, initially infected in 2013 or 2018 with 5 N. americanus L3 from a line donated by Professor David Pritchard (University of Nottingham). Visibly motile L3 were individually selected for inclusion in the inocula, contained within 300 µl of de-ionised water. Placebo inocula comprised 300 µl of de-ionised water containing approximately 2 µl of Tabasco® sauce. The inoculation procedure involved dispensing the solution onto a non-absorbent dressing pad placed onto the participant’s forearm. Two doses of inocula were administered eight weeks apart, with L3-20 and L3-40 participants receiving 10x or 20x L3 on each occasion (Figure 1A). Hookworm infection status was monitored at baseline and six months using qPCR on 1g of thawed and homogenised faecal samples, as described previously 39.
Outcome measures
Safety assessments were conducted at each designated visit (Figure 1A) to identify adverse events (AEs) and serious AEs and their suspected causality. Complete blood counts and metabolic indices (glucose, insulin, HbA1c, liver function tests and lipids) were measured in serum samples at an accredited Australian clinical pathology laboratory. HOMA-IR was calculated by multiplying fasting blood glucose (mmol/L) by insulin (mU/L) values and dividing by 22.529. Blood pressure was monitored using automated blood pressure devices. Height was measured using either a wall-mounted measuring tape or a stadiometer. Waist circumference was measured using a flexible measuring tape. Body mass was recorded using digital scales with a maximum capacity of 250kg. Body mass index (BMI) was calculated by dividing mass in kg by height in meters squared.
Diet, physical activity, mood and depressive state monitoring
The 14-item self-administered Prevención con Dieta Mediterránea (PREDIMED) diet questionnaire was used to monitor changes in participants’ diets throughout the trial 40. Using a scorecard, participants recorded their weekly physical activity, including type, duration, frequency, and intensity, which were combined into a single metric41, the metabolic equivalent of task (MET) per week (MET x duration x frequency = METs/week). To track changes in mood and depressive state, we used the validated Patient Health Questionnaire (PHQ)-9 42.
Statistical analyses
The chi-square test for trend was used to determine differences in the safety of hookworm infection, assessed by the proportions of AEs between each group. The Kaplan-Meier model was used to compare progression through the study, with associations between groups assessed using the Log-rank test statistic. Standard descriptive statistics were performed on all characteristics at baseline and each of the four evaluation visits (categorical variables: absolute and relative frequencies; numerical variables: mean and 95% confidence intervals or median and interquartile range, dependent on data distribution). Normality testing indicated that most data were not normally distributed. Thus, Kruskal-Wallis with Dunn’s multiple comparisons tests were used to detect inter-cohort differences in absolute values and changes or Mann-Whitney tests where hookworm groups were combined (PHQ-9). For significant results in tests with posthoc analyses, the adjusted p-value is reported. For test results stated as not significant, p was > 0.05. To calculate effect sizes (Cohen’s d) for HOMA-IR changes, the following equation was used: d = M1 – M2/δpooled (δpooled, pooled standard deviation) with δpooled = √[(δ12 + δ22)/2] (http://www.bwgriffin.com/gsu/courses/edur9131/content/EffectSizeBecker.pdf).
A research team member and an independent monitor reviewed data from each participant to identify and address missing information. To account for missing data, this study followed the method prescribed in Jakobsen et al.43. Specifically, as missing data exceeded 40%, no imputation was undertaken, and results were interpreted in the context of this limitation. The mixed-effects model (which allows missing values) with Tukey’s multiple comparisons tests was applied for longitudinal analyses with missing values. Statistical analyses were performed in GraphPad Prism 9.0.
Role of the funding source
The funders had no role in the design or conduct of the study
Data Availability
All data produced in the present study are available upon reasonable request to the authors
AUTHOR CONTRIBUTIONS
Conceptualization: RM, AL, TR, JC, and PG. Data analysis: DP, FT, RM, PG. Funding: DP, AL, RM, PG, MF. Investigation: DP, MM, LM, LB, CL, AL, RM, PG. Methodology: DP, MM, LB, JC, AL, RM, PG, MF. Project administration: DP, MM, LM, FT, CL, RM, PG. Writing – original draft. DP and PG. Writing – review & editing: All authors
DECLARATION OF INTERESTS
P.R.G and A.L are founders and shareholders of Macrobiome Therapeutics, which is developing hookworm-derived proteins as drugs for treating inflammatory conditions.
ACKNOWLEDGEMENTS
The work was funded by the Far North QLD Hospital Foundation (PG, RM, AL), Australian Institute of Tropical Health and Medicine (RM, PG, AL), Australian National Health and Medical research Council (NHMRC) Senior Principal Research Fellowship (AL), Program Grant (AL), Advance Queensland Fellowship (PG) and an Australian Research Training Program Stipend (DP). Funders had no role in the design or conduct of the study. We also thank Rebecca Traub, Sze Fui Hii and Patsy Zendajas (University of Melbourne) for assistance with hookworm qPCR assays, Sally McDonald, Lynne Reid, Melissa Piontek, Tyler Gilstrom, Melissa Campbell and Geraldine Buitrago for assistance with clinical trial operations.
REFERENCES



