
Abstract
Bacille Calmette-Guérin (BCG) vaccination supposedly imparts and augments “trained immunity” that cross-protects against multiple unrelated pathogens and enhances general immune surveillance. Gradual reductions in tuberculosis burden over the last 3-5 decades have resulted in the withdrawal of BCG vaccination mandates from developed industrialized countries while reducing to a single neonatal shot in the rest. Concurrently, a steady increase in early childhood Brain and CNS (BCNS) tumors has occurred. Though immunological causes of pediatric BCNS cancer are suspected, the identification of a causal protective variable with an intervention potential has remained elusive. An examination of the countries with contrasting vaccination policies indicates significantly lower BCNS cancer incidence (per hundred-thousand) in countries following neonatal BCG inoculations (n=146) vs. non-BCG countries (n=33) [Mean: 1.26 vs. 2.64; Median: 0.985 vs. 2.8; IQR: 0.31–2.0 vs. 2.4–3.2; P=<0.0001(two-tailed)]. Remarkably, natural Mycobacterium spp. exposure likelihood is negatively correlated with pediatric BCNS cancer incidences in all affected countries [r(154): —0.6085, P=<0.0001]. Seemingly, neonatal BCG vaccination and natural “boosting” are associated with a 15-20-fold lower BCNS cancer incidence. We attempt to synthesize existing evidence implying the immunological basis of early childhood BCNS cancer incidences and briefly indicate possible causes that could have precluded objective analysis of the existing data in the past. A comprehensive evaluation of immune training as a potential protective variable through well-designed controlled clinical trials or registry-based studies as feasible may be warranted for its potential applications in reducing childhood BCNS cancer incidences.
Statement of Significance Potential causal protective variable for childhood Brain and other CNS (BCNS) tumors has eluded discovery. Neonatal BCG vaccination and boosting by Mycobacterium tuberculosis complex exposure seem associated with over 15-20 times lower BCNS cancer incidences. Data suggests neonatal BCG vaccination followed by “boosting” may be preventive for early childhood BCNS cancer incidences.
INTRODUCTION
Bacille Calmette-Guérin (BCG), a derivative of Mycobacterium bovis (a member of M. tuberculosis complex), is the most widely used early childhood vaccine that is in use for over 100 years for protecting against tuberculosis (TB) [1]. It offers the greatest protection against miliary TB and tuberculous meningitis and to a lesser extent against pulmonary TB [2]. However, the non-specific protection offered by BCG against other common pathogens, sepsis, and unrelated conditions has been associated with a reduction in early childhood mortality rate by up to 50% in different studies [3-7]. BCG is supposed to provide this protection through the induction of granulopoiesis, the activation of heterologous T-cell immunity, and enhanced non-specific innate immunity committed through epigenetic and metabolic reprogramming [REFs 8-15]. Mechanistically, the inoculation is supposed to bring about functional reprogramming of the cells of innate immune response (e.g., Monocytes, macrophages, NK cells, etc.) that leads to better immune surveillance and response [REFs 9-16]. In the case of children growing up in ‘hygienic’ conditions, it has been hypothesized to provide the necessary immune stimulus required for a ‘normal’ immune system development that may reduce incidences of common childhood cancers and immune conditions including autoimmune diseases [REFs17-21]. The ability of BCG to potentiate cell-mediated response, which is believed to be important for cancer, has led to its evaluation for preventive and therapeutic potential in many observational studies and clinical trials [REFs 15,18-20,22-28]. However, except in the case of bladder cancer, its preventive and therapeutic potential remains debated and largely uncertain due to the lack of comprehensive and consistent data along with a theoretical framework that could at least attempt to explain different conflicting observations [REFs 15,19,20,22]. The evidence generated so far seems to be overwhelmingly negating the potential of BCG in protecting against cancers. We envision this apparent uncertainty about BCG vaccinations’ potential benefits and conflicting outcomes in different studies to be resulting from the inappropriate generalization of the potency of different BCG vaccines in activating the innate immune system [29,30], omissions about the requirement of boosters [REFs 31-32], longevity of conferred non-specific ‘trained immunity’ that seldom lasts few years in the absence of a booster [31,32,33], treating all cancers as a homogeneous lot disregarding their origin (e.g., embryonal, mutational: sporadic, germline, primary, secondary, etc.), and associated inherent differences, non-consideration of the immune status of subjects and their exposure to a specific intervention and risk factors, etc. in different studies reported in [10,15,17-20,22].
Early childhood cancers are hypothesized to result from embryonic aberrant remnants that could have been otherwise eliminated during ‘normal’ development had the appropriate immune stimulus and training been available in the form of common pathogens and microbes to which we have been exposed during evolution [17-20,22,28]. Based on the observation of children brought up in supposedly more hygienic conditions, a critical role for natural exposure to pathogens for immune reprogramming and maturation has been proposed [17-20,34-36]. ‘Hygienic’ conditions have been associated with increased allergy and atopic conditions, susceptibility to life-threatening infections, and even a higher incidence of cancer [REFs.9,11,17,19-22]. However, for the lack of consistent evidence pinpointing a preventive/protective agent or intervention that may have a direct causal relationship, ambivalence about their actual potential in cancer incidence prevention has remained [REFs15,17,19, 22,28].
RESULTS
Changing Incidences of Early Childhood Brain and Central Nervous System (BCNS) Cancer and Potential Risk Factors
Brain and other central nervous system (BCNS) cancer remains the second most frequently occurring childhood cancer and the most frequent cause of cancer mortality [37]. The updated estimates for all cancers and ages periodically produced by the International Agency for Research on Cancer, WHO as a part of the GLOBOCAN project (https://gco.iarc.fr/today/home) are a comprehensive source of cancer incidence estimates and related information. Incidentally, the industrialized Western world with high living standards and hygiene has higher incidence rates of both early childhood and later-age BCNS cancer [37]. Most of the countries for which estimates are available have been steadily registering an annual increase in childhood BCNS cancer incidences for the last 3-5 decades [37]. The improvement in TB prevalence and incidences resulting from improved hygiene and living standards globally had also seen a concomitant reversal of BCG mandates, and changes in BCG booster schedules, or altogether scrapping in several countries [38,39]. For the majority of countries/territories with data, the estimated annual % change in total BCNS cancer incidences has been positive (10 out of 42) for recent decades (Supplementary Figure 1) [37]. The childhood BCNS cancer incidence is highest in 0-4-Year-olds (0-4Y-Old or younger than 5 years) and decreases in older 5-14Y-old children. GLOBOCAN study estimates BCNS cancer incidence and associated mortality among 0-4Y-olds during the year 2020 to be 9252 and 4256, respectively, which accounted for about 16% of incidence and 20% of associated deaths from all cancer types combined [37]. Despite, advances in diagnostics and therapeutics, the preventive vaccines and causative risk factors for the majority of early childhood BCNS cancers remain unidentified and uncharacterized [40-43]. Though previously the occurrence of malignant and embryonic origin BCNS tumors in children <5 years has been associated with risk factors like socioeconomic position [41,42,44], allergy [REFs. 42,45,46], infections or exposure to pathogens early in life [REFs. 47,48], human developmental index (HDI), etc. [REFs. 41-48], the identification of potential protective risk factors with an intervention potential (i.e., employable or actionable) to reduce the incidence of BCNS cancers has so far remained an unfulfilled aspiration.
Compared to BCNS cancers arising in any other age group, the early childhood incidences are predominantly of embryonal origin and malignant, and their incidence rates decrease with age [REFs 40-43]. The scientific community may be aware of the fact that although globally BCNS cancer incidence rates pick up again around 20 years of age and keep going up with age [37,40,41], they are overwhelmingly not of the same origin (up to 10-fold) [42,43]. This offers an opportunity to evaluate any potential role of immune modulation and maturation, more specifically that of BCG vaccination, the most widely given vaccine, on the incidence of childhood BCNS cancer, if any. We surmise that if early childhood BCG vaccination-induced/primed non-specific trained immunity could play any role in cancer incidences arising from abnormal immune system development and maturation, their effect would be more discernible in early childhood cancers, which allegedly arise from embryonic remnants that could not be eliminated during early development for the lack of appropriate and timely immune system stimulation (priming and maturation). The policy on BCG vaccination varies by country (Table 1) [39]. Currently, the majority of middle-to low-income countries follow the BCG vaccination policy for newborns, while non-BCG mandating countries (No-BCG) are mostly affluent high-income countries [49] with very high (vh-) to high (h-) HDI – a composite measure of “a long and healthy life, access to knowledge and a decent standard of living” [50]. The existence of disparities in BCG vaccination policies [39] and TB incidence rates (i.e., M. tuberculosis complex exposure possibility) across countries [51] provides a unique opportunity to test the hypothesis that BCG vaccination and/or “boosting” may be potentially protective (alternatively non-protective) in early childhood BCNS cancer.
Early Childhood Brain and other Central Nervous System (BCNS) cancer incidence in countries with varying tuberculosis (TB) incidence rates (potential exposure) and correlation analysis
BCG Countries Frequently Have Lower Incidence Of Early Childhood BCNS Cancer
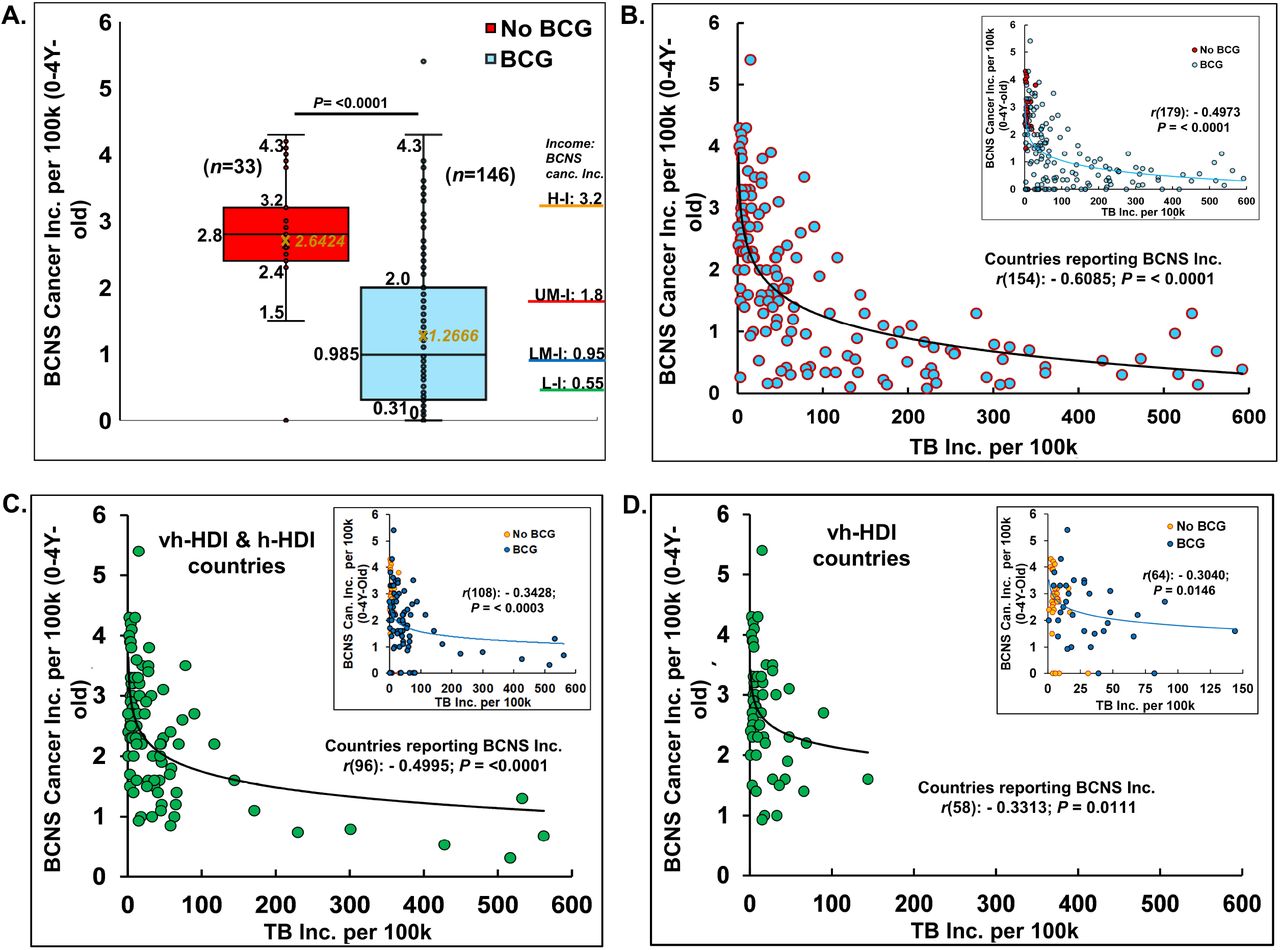
Globally, the distribution of updated age-standardized incidence rates (ASR) of BCNS cancer for the recent year 2020 [37] varies widely from 0 to 5.4 per 100,000 (100k) in 0-4Y-olds (Table 1). Nevertheless, the widely mandated BCG vaccination seems associated with reduced childhood BCNS cancer incidences in 0-4Y-olds (Figure 1A). The countries of Europe and North America with no neonatal BCG vaccination policy in place (‘No-BCG’ or ‘NB’) are some of the worst affected countries, while incidence rates in countries with BCG vaccination in place (BCG countries) do have some similar high incidence rate countries, but the majority seem to cluster towards lower incidence rates. The incidences in No-BCG and BCG countries significantly differ (Mean: 2.64 vs 1.26; Median: 2.8 vs 0.985; IQR; 2.4–3.2 vs 0.31–2.0; P = <0.0001 (two-tailed)). The high to low incidence rates of BCNS cancer among countries also display an interesting association with countries’ income brackets [49]. The higher income brackets have higher average incidence rates than the lower income brackets (Figure 1A: right side Y axis). The previous observations made in small-scale studies performed in different countries that identified the socioeconomic position (SEP) of families as a potential risk factor positively associated with childhood BCNS cancer incidences [52,53], seem to be applicable globally. However, the occurrence of high incidence rates (ASR) in certain BCG vaccinating countries of Europe [notably, Montenegro (5.4), Estonia (4.3), Croatia (4.3), North Macedonia (3.6), Republic of Moldova (3.5), Lithuania (3.4), Serbia, Poland (3.3)] along with wide variation in incidence rates among BCG vaccinating countries 0 – 5.4, casts doubt on the ability of single BCG shots alone to protect young children from BCNS cancers, as could have been the case in some of the past studies reported in [15,19,20,22] that failed to find an association between BCG vaccination and cancer incidence.

{kind=link}
Globally, the distribution of age-standardized BCNS cancer incidence rates (ASR) among countries (n=179) are shown as Box and whisker plot (A). BCG-vaccinated children had significantly reduced incidences (t-test: two-tailed, equal/unequal variance) than the non-vaccinated (No BCG). The average incidence rate seems directly proportional to income levels [H-I: High ($13,205 or more); UM-I: Upper Middle (between $4,256 and $13,205); LM-I: Lower Middle ($1,086 and $4,255); L-I: Low income (≤$1,086) as defined by World Bank, 2023 [49] (For CI refer to [37]). The probability of natural boosting (exposure to the M. tuberculosis complex) is associated with lower BCNS cancer incidence in the affected countries/territories: All (B); vh-HDI and h-HDI (C) and vh-HDI countries (D). Inset has countries color-coded for BCG and No BCG groups. The trend lines are drawn to guide the eye. Note: Outliers presence in No-BCG and BCG groups (A). Most of the high BCNS incidence displaying countries of the BCG group including the outlier are clustered in low background M. tuberculosis complex exposure regions with TB incidence rate <100 per 100k (B,C) for the year 2020.
Globally, Higher Natural “Boosting” Potential Negatively Associated With Pediatric BCNS Cancer Incidences In Countries
A missing explanatory variable for the observed reduced BCNS cancer incidences in BCG countries could be the ‘boosting’ stimulus (also priming for No-BCG countries) arising from natural exposure to boosting events in the form of M. tuberculosis complex exposure specific to populations. It may be pertinent here to reiterate for the scientists from other backgrounds that M. tuberculosis complex exposure does not invariably cause TB but rather only sustained long-term exposure of susceptible individuals, which constitutes a small fraction of the population – variously estimated to be <1-5%, is supposed to result in clinical TB [REFs. 33,54]. Assuming the BCG vaccination could be playing a role in the BCNS cancer incidences in young children, the higher incidences in some countries could be envisioned to result from the inability of a single BCG inoculation to sufficiently activate the immune system in the absence of proper, timely boosting. Revaccination has been indicated to enhance the non-specific protective effects of BCG in early childhood [REFs. 3,55,56]. The neonates in countries with higher TB prevalence or incidence rates [51] could be more frequently exposed to natural boosting events than those born in low TB incidence countries.
Surprisingly, when we look at the covariation of BCNS cancer incidence rates [37] with countries’ TB incidence rates [51] they are found to be significantly negatively correlated even when completely disregarding their BCG vaccination policy (Table 1). This correlation further improves on consideration of the countries reporting childhood BCNS cancer incidences [Table 1, Affected countries: r(154): - 0.6085, P = <0.0001; All countries (affected + non-affected) r(179): - 0.4973; P= <0.0001]. The consideration of only BCG countries slightly decreases the correlation that could be potentially indicative of the important role of exposure to the M. tuberculosis complex in No-BCG countries as well. Looking at the distribution of BCNS cancer incidences, it seems to be decreasing exponentially with the increase in TB incidence rates of the countries (i.e., increased probability of natural exposure: priming and boosting). The seeming outlier of the BCG vaccination group that reported BCNS cancer incidences of 5.4 (i.e., Montenegro) as well as other high-incidence reporting countries happened to be some of the least TB incidence (M. tuberculosis complex exposure) countries of the No-BCG and BCG group of countries (Figure 1B). The increase in TB incidence rates up to 100 per 100,000 (100k), is seemingly associated with a four-fold reduction in BCNS cancer incidences among 0-4Y-olds, which further goes down by two-fold on an increase in TB incidence to 200 per 100k. The same trend follows till the highest TB incidence rate of about 600 per 100k, potentially indicating TB incidence rates in populations as a risk factor inversely correlated with early childhood BCNS cancer incidences.
In Very High- and High-Human Development Index (HDI) Countries, Childhood BCNS Cancer Incidences Negatively Associated With the Natural “Boosting” Possibility
The reporting of childhood BCNS cancer incidences across countries has not been uniform. The projected estimates could be more skewed in low HDI countries because of the possible lack of education, medical infrastructure, diagnostics, affordability, and reporting. Historical estimates for many countries display fluctuations in 3–8-year periods with extreme variations in sex-specific incidences, potentially indicative of more imprecise estimates, and underline a need for better data reporting and collation than current [37]. Thus, consideration of the latest BCNS cancer incidence estimates in very high HDI (vh-HDI) and high HDI (h-HDI) countries may be expected to more reliably illustrate the association, if any. Remarkably, the BCNS cancer incidence among 0-4Y-olds in vh-HDI and h-HDI countries during 2020 was also found to be significantly but negatively correlated with their TB incidence rates [Figure 1C-D; Table 1, Affected vh-& h-HDI: r(96): −0.4995; P = < 0.0001; All (affected + non-affected) vh-& h-HDI: r(108): −0.3428, P = < 0.0003). For the associations in various subgroups, refer to Table 1. The negative association between childhood BCNS cancer incidences and exposure to the M. tuberculosis complex remained significant for vh-HDI and h-HDI countries separately as well (Table 1 subgroups).
DISCUSSION
The early childhood BCNS cancer incidence in countries appears to be negatively associated with the prevailing possibility of exposure to the M. tuberculosis complex. The observations presented could be construed as indicative of non-exposure to M. tuberculosis complex or “boosting” as an unidentified risk factor for childhood BCNS cancer, possibly functionally related to the “Hygiene Hypothesis” and associated trained immunity. The boosting event(s) could be necessary for supposed priming or activation (immunomodulation), and reprogramming of the metabolism for desired outcomes. We suspect the current regimen of single neonatal BCG inoculation may not be sufficient to cause desired immune activations in environments lacking boosting opportunities. Possibly, multiple shot regimens, as used to be given earlier in many countries [39] or suggested for enhancing nonspecific effects [55,56] may be necessary for providing the required stimulus and boosting to stem the steady annual rise of early childhood BCNS cancer incidences globally [37]. However, since a large majority of early childhood BCNS cancers are supposedly embryonic developmental remnants, the likelihood of the mother’s immune system getting modulated by exposure to BCG and/or M. tuberculosis complex itself and in effect modulating and moderating that of the embryo (in utero, including endocrine) for ‘normal’ development remains a possibility [20,28]. We would be inclined to suggest the pouring and pooling of resources for a thorough evaluation of BCG’s potential in reducing childhood BCNS cancer incidences. With BCNS cancers in children on the rise, carefully planned, appropriately controlled, multicentric clinical trials preferably coordinated and managed by WHO be performed in high-incidence countries, both No-BCG and BCG countries to reliably evaluate the qualitative and quantitative contributions of neonatal BCG inoculation(s), boosting, and the mother’s immune system modulation. The countries with zero incidence rates could provide additional insights in terms of etiological agents as well as help identify unknown risk factors specific to countries that are responsible for huge differences in the BCNS cancer incidence rate even among socially similar vh-HDI countries (e.g., Iceland, Luxembourg vs. Germany, Ireland, Greece, Montenegro, etc.). If immunomodulation has a role in the increased incidence of BCNS cancers in childhood, the recent change in schedule and policy from multiple to single to no BCG inoculations could be costing us >10-fold higher incidence and mortality.
The inherent limitations of the cancer incidences dataset arising from data availability and methodology employed [57] should also be considered when planning for exploratory evaluation studies. As BCNS cancer incidences and reporting globally remain fragmentary [37,57], the studies, whether prospective or registry-based retrospective, should wherever possible be performed in high-incidence but low TB prevalence countries, carefully controlling for age, trained immunity status, mothers’ immunization, etc. to arrive at meaningful conclusions about its preventive interventional potential. Consideration of existing trends of incidence in previous relevant years [37] as a baseline could provide additional pointers to help reliably estimate the impact of specific interventions in clinical trials.
CONCLUSION
BCG vaccinations coupled with timely natural “boosting” could be causally associated with a reduction in childhood BCNS cancer incidences. Future research may be directed at evaluating the same in carefully controlled trials and identifying country-specific differences and modifiers. It is needed to improve our understanding of the role of BCG vaccination and the mechanistic details of the potential protective immune augmentation process. It may help devise ways to stem the steady rise of early childhood cancer incidences with similar components. Additionally, the findings could indicate inoculation regimens that are better suited for lowering early childhood cancer incidences. The revised multiple BCG vaccinations, as they used to be, may have to be reintroduced globally to reduce childhood cancer incidences. The countries with higher incidence rates (ASR per 100k), e.g., Montenegro (5.4), Estonia (4.3), USA (4.3), Greece (4.2), Canada (4.1), Israel (4), Slovakia (3.9), Slovenia (3.9), etc., are going to gain the most in terms of morbidity and mortality reduction. However, a lot needs to be done to reliably ascertain the potential benefits of BCG vaccination in reducing cancer incidence, or the lack thereof, before this could be again reintroduced or written off.
MATERIALS AND METHODS
The estimates of cancer incidence rates in different age groups in individual countries are from GLOBOCAN 2020, International Agency for Research on Cancer, WHO [37]. The BCG vaccination policy information is from the World Atlas of BCG Policies and Practices, 3rd Edition [39]. The categorization of countries in different income groups is from the World Bank Group, 2023 [49]. The countries’ categorization as very high- and high-Human Development Index in 2020 is primarily from Human Development Report 2021/2022 by United Nations Development Programme [50]. The estimates of Tuberculosis incidence in 2020 are from WHO, Global Tuberculosis Programme [51]. Basic statistical analysis is performed using Excel 2019. The P-value <0.05 is reported as significant.
Data Availability
All data produced in the present work are contained in the manuscript and available online
Author Contributions
SS conceived the idea, designed the research, analyzed the data, and wrote the paper. RKS and AD wrote the paper.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they have no conflict of interest.
Competing Interests statement
No competing interest to disclose
Data Availability Statement
All pertinent data is available in the public domain and is included in the manuscript and the associated supplementary file. The raw data generated as a part of the analysis is also available on request.
Ethics statement
The study complies with ethical requirements and standards. No identifiable human data is used.
Figure Legends
Supplementary Figure 1. Estimated Annual Percentage Change of Brain and Central Nervous System Cancer Incidence ASR per 100,000 in 0-4Y-olds. Majority of No-BCG and BCG countries/territories (n=44) display positive annual percentage change in combined incidences for sexes in 0-4Y-olds (last 15 years data). Bars show CI (Available at https://gco.iarc.fr/overtime/en/dataviz/eapc?populations=38000_3600_7600_10000_11200_12400_15200_15600_17000_19100_18800_20300_20800_21800_25000_27600_23300_35200_35600_37200_37600_39200_41000_41400_42800_44000_47000_52800_55400_57800_6 1600_70300_70500_72400_75200_75600_76400_79200_80000_80400_82630_82610_84000_82620&sexes=1_2&multiple_populations=1&years=2018&cancers=23&types=0&key=asr&ag e_end=0&group_cancers=0&multiple_cancers=0&mode=population&age_start=0&group_year s=0&eapc_span=15&ul=1). Note: The historical estimates remain weak. The observed sex-specific incidence variation in the past for specific years or over time could be indicative of reporting issues. (Available at https://gco.iarc.fr/overtime/en/dataviz/trends?populations=38000&sexes=1_2&multiple_po pulations=1&years=1943_2018&cancers=23&types=0&key=asr&age_end=0&group_cancers= 0&multiple_cancers=0&mode=population&age_start=0&group_years=0).
Acknowledgments
The laboratory of SS is supported by a seed grant from IoE, Banaras Hindu University. The work presented is unfunded.
REFERENCES



