
Abstract
The increased prevalence of obesity is due to a decreased level of physical activity and increased intake of fast food. Furthermore, obesity among children and adolescent is a risk factor for life-threatening conditions including cardiovascular diseases (CVD), Cardio-metabolic disorders, type 2 diabetes mellitus, hypertension, cancer and reproductive disorders. The aim of this study is to describe the determinants of obesity. A cross-sectional study was conducted on a total of 377 adolescents aged 13 to 20 years from 16 secondary schools in Thulamela Municipality, Vhembe District Limpopo Province, South Africa. Information about socio-demographic characteristics, household income, disease family history, and level of education of parents was obtained using a self-administered questionnaire. Anthropometric measurements such as weight, height and waist circumference were taken by trained field workers and body mass index (BMI), and the waist-hip ratio were determined. Biochemical measurements and clinical assessment were done by a professional nurse following standard procedures. The prevalence of obesity is 22.2% in males and 32.6% in females by abdominal obesity by (waist circumference), whilst 11.1% (males) and 28.3% (females) by waist to hip ratio (WHR). Gender (β=0.32, p=0.018, 95%CI); age (β=1.28, p=0.015, 95%CI); source of income (β=3.25, p=0.008, 95%CI) and systolic blood pressure (β=1.04, p=0.01, 95%CI) were associated with obesity. Overweight and obesity were more prevalent in females than in males in Thulamela municipality. There is a need to bring up children and adolescents in a health-promoting environment in an effort to reverse and stop the increasing trend of overweight and obesity.
INTRODUCTION
Obesity is defined as excessive or abnormal body fat accumulation that may result in serious health problems [1]. Globally obesity among children and adolescents is a serious public health concern [2,3]. Children and adolescents’ obesity indicates a higher risk of transition to adulthood [4-6]. The increased prevalence of obesity is due to decreased level of physical activity and increased intake of fast food [7-9]. Furthermore, obesity among children and adolescent is a risk factor for life-threatening conditions including CVD, Cardio-metabolic disorders, type2 diabetes mellitus, hypertension, cancer and reproductive disorders [10,11].
The prevalence of global obesity has doubled from the year 2000 to 2016, with an estimation of 650 million adults being obese in 2016 [9]. WHO [12] reported that over 340 million children and adolescents were obese in 2016. In 2010, 43 million children were obese with 81% coming from developing countries [13]. Obesity is considered a problem in developed countries however, it is currently on the rise in developing countries [1,14,15]. In South Africa, the prevalence of overweight and obesity has increased from 49.4% in 1980 to 57.8% in 2015 [16]. Studies, [17-20] reported that the prevalence of overweight and obesity is high in girls than in boys. Most studies focused on the prevalence of obesity in urban areas, the ones tracking the determinants of obesity were conducted in urban areas [21]. Little is known about the prevalence and determinants of obesity in the Vhembe district. The aim of this study is to describe the determinants of obesity in Vhembe district, Limpopo Province, SA.
METHODS
Participants and study design and sampling
The study is descriptive in nature and followed a cross-sectional design. Slovin’s formula was used to determine the sample size. The formula yielded 400 however 377 adolescents agreed to participate in the study. The participants were selected using stratified random sampling whereby five participants were selected per grade (grades: 8-12). From each secondary school, 25 adolescents were selected. Adolescents attending were free from illness and whose parents gave consent to participate in the study. Pregnant adolescents were excluded from the study. The response rate was 94.25%.
Study participation
A total of 377 adolescents aged 13 to 20 years from 16 secondary schools participated in the study from February 2018 to August 2018. Participants were recruited in January 2018. The research took place in secondary schools in Thulamela Municipality, Vhembe District, Limpopo Province, South Africa. Vhembe District covers a geographical area that is predominantly rural. Information about socio-demographic characteristics, household income, disease family history, and level of education of parents was obtained using a researcher-administered questionnaire.
Anthropometric measurements
Body height was measured, without wearing shoes, by trained fieldworkers with an accuracy of 0.1 cm, using a portable Harpenden stadiometer (Holtain Ltd., Crymych, UK). Bodyweight was measured with participants wearing light clothing using a calibrated electronic scale (SECA, Birmingham, UK) with an accuracy of 0.1 kg. Body mass index (BMI) in kg/m2 was determined and classified according to International Obesity Task Force (IOTF) cut-off points for children and adolescents [22]. BMI was used as a proxy for overall obesity.
Waist circumference was measured using an inelastic flexible measuring tape. The participants were wearing light clothing. The researchers located the top of the right iliac crest, the highest point of the hip bone on the right side. The measuring tape was in a horizontal plane around the abdomen at the level of the iliac crest. The measurements were recorded to the nearest 0.1 cm and waist circumference for adolescents 18 years and below was classified according to age and sex [23]. For adolescents above 18 years, the WHO cut-off points of WC were used [24].
The participant stood erect with arms at the side and feet together. The measurement was taken at the point yielding the maximum circumference over the buttocks, with the tape held in a horizontal plane, touching the skin but indenting the soft tissue [25]. Waist and hip circumferences were measured to determine Waist-to-hip-ratio (WHR). WHR was calculated and the WHO cut-off points were used [24]. Waist circumference was used as a proxy to determine android obesity.
Biochemical measurements
A professional nurse was responsible for collecting blood samples. One participant was brought to the room at a time. The participant’s skin was cleaned with alcohol-soaked gauze pads at the tip of the finger. The participant’s finger was pricked, and the blood drops were allowed fall on the test panel of a Cardio-check device. A Cardio-check device (model CE 0197) was used to determine total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), triglycerides (TG), and glucose level. TC, LDL-C, HDL.C and TG were classified according to age and gender lipoprotein for adolescents [26]. Glucose level was classified according to laboratory standards.
Clinical assessment: Blood pressure (BP)
A professional nurse was responsible for taking blood pressure readings using standard procedures. BP reading was taken using a digital automated device OMRO (model CE0197). Each participant sat quietly for 5-10 minutes after their arm was placed at heart level and BP was measured at least 3 times in 5 minutes intervals. If BP varied in these determinations by greater than 10mmHg, 3 additional trials were performed to measure systolic and diastolic blood pressure. BP for adolescents less than 18 years were classified according to sex, age, and height [27]. For adolescents ≥18 years BP was classified according to American Heart Association (AHA) for adults [28].
Assessment of dietary Intake
A quantified food frequency questionnaire (FFQ) was used to assess the dietary intake of the study participants. The researchers gave the adolescents a pile of pictures with food items and instructed them to put pictures of food items he/she ate in the past week on the right hand and the ones they did not eat on the left-hand side. From the selected food items, adolescents were then asked about how many times per week and per day they consumed the foods. The standard portion sizes for food items were included in the FFQ. With both the frequency of consumption and the standard portion sizes the total portion sizes were calculated. The food models and the line drawing from the DAEK manual assisted the adolescents to estimate the portion sizes. The data gathered were analysed using the Food Finder computer software (version 1.1.3) to assess the dietary intake. The aim of the analysis was to determine the amount of each nutrient and energy consumed per day. These nutrients included carbohydrates, lipids, proteins, minerals, and vitamins.
Physical activity
A physical activity questionnaire by Sharkey and Gaskill [29] was adopted to assess the physical activity level. A questionnaire included physical activity patterns in and around the house, travelling to school and recreations that participants engaged in. Information such as sedentary lifestyle, after-school activities, time spent on television viewing, and sleep duration frequency was included in the questionnaire. Table 1 indicate the interpretation of physical activity indices. The following formula was used to calculate physical activity indices:

Statistical analysis
Data were checked for completeness and consistency. Data were entered, cleaned, and analysed using SPSS (IBM Corporation, USA) version 26 statistical package software. Descriptive statistics like frequencies and proportions were used to summarize the data. Shapiro Wilk and Kolmogorov Smirnov test were used to test for normality. The data was homogenous. ANOVA was used to determine the differences between BMI classifications. Logistic regression was used for bivariate and multivariate analyses to calculate unadjusted and adjusted odds ratios (AOR) for determinants of obesity. Statistical significance was set at p < 0.05.
Ethics approval
The study was approved by the Research and Ethics Committee of the University of Venda and the Ethical clearance certificate was issued (SHS/17/NUT/03/1506). Permission to conduct the study was granted by the Provincial and District Departments of Basic Education. No participant could participate in the study without signed informed consent by parents and an assent form by participants after a full and adequate explanation of the study. The data obtained from the study were kept on a computer database in such a manner that it maintains the participants’ confidentiality (a code was assigned to each participant for these purposes).
RESULTS
Demographic characteristics
The characteristics of the study participants are indicated in Table 2. The mean age of the study participants was 16.56±2.10. Majority were of Vha-Venda ethnic group. The frequency of buying food at school was more prevalent in the overweight and obese group for both boys and girls. Majority of the guardians had secondary education. Parents with secondary school education had children with the highest prevalence of overweight and obesity. Learners whose parents/guardians receive a salary or wages had a higher prevalence of overweight and obesity.
Anthropometry, clinical assessment, and biochemical measurements of study participants
The prevalence of abdominal obesity among boys and girls was 22.2% and 32.6% respectively. The high prevalence of substantially increased WHR was seen in overweight boys and obese girls. Among the classified as obese, only 13% had hypertensive SBP (Table 3).
BMI classification of the study participants
The mean BMI of boys was 20.81±3.45 and that of girls was 23.3±4.90. There was a significant difference between boys and girls in terms of BMI P-value was less than 0.005. The results of the study population show that the prevalence of overall combined overweight/obesity is 21.5%. The prevalence of overweight and obesity was higher in girls than in boys (Figure 1).

BMI classification
Determinants of obesity
The determinants of obesity are shown in Table 4. Gender (female) (β=0.32, p=0.018, 95%CI); age (β=1.28, p=0.015, 95%CI); source of income for parents who earn salary or wages (β=3.25, p=0.008, 95%CI) and systolic blood pressure (β=1.04, p=0.01, 95%CI) were associated with obesity.
Comparison of means of variables
Table 5 below compares the means of variables. For WC there was a significant difference between BMI categories in both males and females. Among females, there was a significant difference between BMI categories in W/HR, SBP, HDL and TCHDL.
Comparison of means of nutrient intake
The comparison of means of nutrient intake is discussed in Table 6. The result of the study shows that boys who were in obese and normal category did not meet daily energy requirements, whereas obese girls were consuming more energy. Boys in the obese category were consuming low Total fats as compared to boys in the normal and overweight classification and girls in all classifications who were consuming more than recommended daily total fats intake. When it comes to Total fibre only obese boys who do not meet daily fibre intake. All adolescents were consuming more than the daily recommendations in carbohydrates.
Physical activity
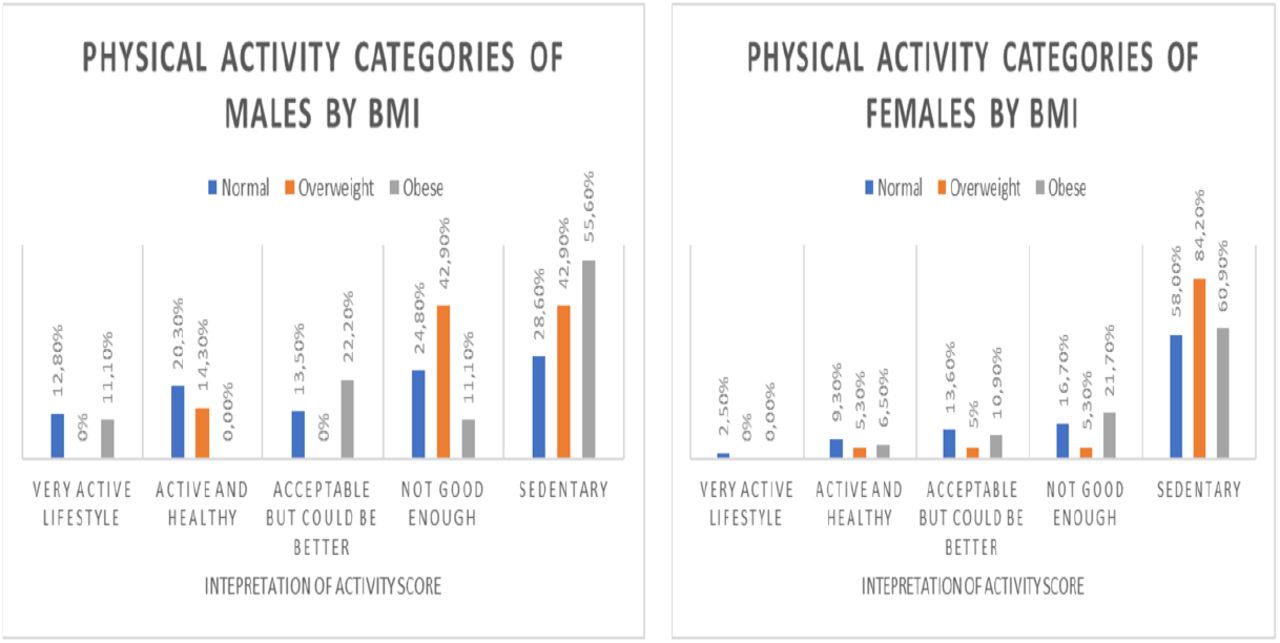
Majority of overweight and obese boys and girls led a sedentary lifestyle. The results show that the prevalence of a sedentary lifestyle was high in overweight and obese girls than in boys. At least a few percentages of obese boys had a very active lifestyle as compared to girls (Figure 2).

{kind=link}
{kind=link}
Physical activity categories of males and females by BMI. Physical activity
DISCUSSION
The aim of the study was to describe the determinants of obesity among rural secondary school learners in Thulamela Municipality, Vhembe District, Limpopo province, South Africa. The findings showed the prevalence of overweight and obesity to be 21.5%. The prevalence of overweight and obesity was lower than that of 35% by Debeila et al. (2021) [30] in rural high schools in Limpopo province South Africa. It was also lower than the prevalence found in the provincial dietary intake study conducted in Gauteng (overweight 27.7% vs obese 39.1%) and the Western Cape (overweight 20.4% vs obese 50.6%) [31]. The overall prevalence of overweight and obesity in this study is lower than the national range of 8.6% to 27.0% among adolescents aged 15 to 19 years reported by UNICEF 2018 [32]. The prevalence of overall overweight and obesity is lower than that of other studies conducted in urban and rural settings in South Africa. Recently, a prevalence of 22.9% of overweight/obesity among adolescents in urban high schools in the Western Cape in South Africa has been reported [33]. The prevalence of overweight and obesity reported in this study is lower compared to studies conducted by Negash et al. (2017) and UICEF (2018) [33,32] in South Africa. Although the prevalence in the present study is lower than that of other studies, it is evident that overweight and obesity is increasing in the rural population [34].
The result of the current study showed that the prevalence of overweight and obesity was higher in females (28.7%) than in males (10.7%). The results are comparable with several studies done in South Africa [33,18,20]. However, the combined prevalence of overweight and obesity reported in girls is almost the same as that of Negash et al. (2017) [33] with the prevalence of overweight and obesity in girls being 28.8%. Physiologically girls require less energy than boys [35]. On a behavioural level, girls are reported to be more attentive to food and its effect on health and weight control than boys [36]. In addition, adolescent girls are less likely to meet physical activity recommendations than boys [37].
In addition to the overall overweight and obesity prevalence, the results found a prevalence of abdominal obesity indicated by elevated WC (5.9%) and elevated WHR (8.5%). As seen in the results, abdominal obesity was high in girls than in boys. The result suggests that girls are significantly affected by abdominal obesity. Sekokotla et al. (2017) [38] reported abdominal obesity among adolescents in South Africa. Studies done amongst students in Ghana by [39,40] Mogre et al. (2014) and Mogre et al. (2015) highlighted higher odds of abdominal obesity amongst females compared to males. Adolescent females are twice as likely to be abdominal obese than males based on WC and WHR indicators. The prevalence reported in this study highlight a public health implication. Abdominal obesity in children and adolescents is strongly associated with metabolic risk factors compared to overall obesity [41,42].
The results of the study show that majority of the participants were leading a sedentary lifestyle. Females were less active compared to males. This is not surprising since studies have reported that girls are less likely to be physically active as compared to boys [37,43-47]. The WHO report ranks physical inactivity as the fourth leading cause of global mortality, with responsibility for 6% of deaths worldwide [48,49]. Kallio et al. (2021) [50] reported that a physical inactivity lifestyle is associated with cardiometabolic risk factors. Additionally, Tremblay et al. (2011) [51] found that higher sedentary behaviour is associated with adverse health outcomes.
The results of the study suggest that being female increased the odds of being obese. Studies [52,33] tracking the determinants of obesity arrived at similar conclusions where it was reported being female was a determinant of obesity and females were twice likely to be obese than males. Female adolescents tend to have higher BMI as a result of rapid growth and early sexual maturity [53].
An increase in age was associated with the odds of being obese. Similarly, the study conducted in India reported that adolescents above 14 years and older had 2.09 times more odds of being obese [54]. Studies tracking the prevalence of obesity in SA indicate that the prevalence of obesity increases with the age, peaking at age 12 years and declining thereafter [55,17]. This may be due to the increase in adipose tissue and overall body weight in adolescents during puberty [56]. According to Kimani-Murage et al. (2010) [4], the risk of obesity increases with sexual maturation, indicating a higher risk as the adolescent transitions to adulthood.
In the current study parent who earns salary or wages as a source of income was strongly associated with obesity. The results of the current study show that parent source of income is a significant determinant of obesity among adolescents. The results of the study are consistent with the findings of Choukem et al. [57] where high SES was strongly associated with obesity among children, with almost 2.5 times more likely to be obese than those with low SES. Concurrently a study conducted on Moroccan adolescents, reported that high family income was a determinant of obesity [58]. Money gives children a certain degree of autonomy in purchasing and consumption [59,60] some of which entail health risks [61] such as smoking and substance abuse [62-66]. Studies from US, Europe, India, Korea and Vietnam suggest that pocket money is a potential risk factor for child’s unhealthy eating and thus overweight and obesity [59,60,67-70].
The odds of obesity increased in participants who do not engage in moderate exercise. As observed in the current study, many of the females were not physically active. Therefore, it can be deduced that females are at greater risk of being obese. Ahmad et al. [53] maintain that girls engage in less physical activity and sport, as compared to boys of great concern, is the cultural influence that girls do not move around than boys leading to physical inactivity and eventually the development of obesity [3]. Studies, [71,46] reported a decline in physical activity among adolescents. Furthermore, physical inactivity and increased sedentary time play a role in the development of obesity [71].
The results of the study revealed that 1 mmHg of SBP was associated with an increase in the odds of being obese. Concurrently, Ghomari-Boukhatem et al. and Negash et al. [72,33] reported that hypertension increases the odds of being obese among adolescents. Confirming the findings of the current study, are studies conducted in SA where SBP was associated with obesity [73,74]. The association of hypertension and obesity among adolescents may highlight those cardio-metabolic comorbidities which do not only occur in adults but may develop in children and adolescents, particularly in the presence of obesity [33]. The relationship between hypertension and obesity decrees effects which may be attributable to the nutrition transition which results in sedentary living and overfeeding [73].
The present study reveals that high TC, LDL, and low HDL as determinants of obesity. This is similar to the study conducted by Ghomari-Boukhatem et al. [73] which reported elevated TC, LDL-C, TG and low HDL-C as risk factors for obesity. Furthermore, a study conducted in the USA among children and adolescents shows that youth with obesity had a higher prevalence of high TC and low HDL-C than those with normal weight [77]. Bibilon et al. [76] stated that obese children were associated with the existence of at least one abnormal lipoprotein concentration. Studies, [77-80] reported that abnormalities in these lipoproteins as the strongest risk factor for CVD. Miller et al. and D’Adamo et al. [77,81] maintain that atherogenesis is associated with lipoprotein and obesity.
High consumption of energy, total fats, total trans fats, carbohydrates and added sugar were reported as determinants of obesity in the current study. Similarly, Appannah et al. [82] reported that energy-dense and high fat intake is associated with cardiometabolic risk factors insulin resistance and obesity among adolescents. Allioua et al. [83] also reported that high consumption of fats was associated with obesity among adolescents. A high energy intake is a major risk factor for obesity in children and adults [17]. In addition, high energy intake together with high total fats, high saturated fats, high carbohydrates, high added sugar and low fibre intake has been classified as western diet which contributes to the development of chronic diseases [17]. Studies [19,84,85] show that a high intake of fats and sugar increases the risk of childhood obesity, as well as non-communicable diseases such as type 2 diabetes and CVD, later in life. Low fibre intake was observed in obese boys, while other adolescents were meeting the daily recommendation. Dreher. [86] reported that fibre is one of the under-consumed nutrients and low intake increases weight gain over time. Studies, [86,87] show that high fibre intake to be associated with lower anthropometric indices including weight and WC.
Adolescents are nutritionally vulnerable, they frequently make poor food choices [85]. Furthermore, school children spend more time at school and most vendors sell energy-dense food such as crisps, fat cakes, French fries, sweets, and carbonated sweet drinks [88]. The association between high total fats, trans fats and carbohydrate intake and obesity in the present study suggests that there is a peak in the nutritional transition and weight status in rural communities.
LIMITATIONS
The study has several limitations. The study was cross-sectional in nature using adolescents from the different geographical areas within Thulamela municipality. The number of adolescents included in the study was small and generalisability within this group would be limited. The study did not determine the BMI and dietary intake of the parents. Tanner staging was not determined in the current study.
CONCLUSION
The prevalence of obesity was higher in girls than in boys. The determinants of obesity include gender, age, source of income, SBP, LDL low HDL, Total trans fats and carbohydrates. Majority of overweight and obese adolescents led a sedentary lifestyle. The results observed in the study confirm the trend that is observed in urban children and adolescents. Lifestyle and diet modification should be encouraged to curb the onset of obesity. Nutrition and physical activity education components should be infused in the school curriculum to promote an active lifestyle. Department of Education together with health professionals and policymakers should develop a nutrition guide for food sold by vendors and revisit its school feeding scheme for optimal benefits. There is a need to conduct more studies to address gaps in government intervention programmes in South Africa with a view to promoting adolescent health.
Data Availability
The data used for the research in this paper is owned by the University of Venda Research Ethics Committe.
AUTHOR CONTRIBUTION
Conceptualization: Brenda Baloyi and Solomon Mabapa.
Data curation: Brenda Baloyi
Formal analysis: Brenda Baloyi and Solomon Mabapa.
Methodology: Brenda Baloyi and Solomon Mabapa.
Writing – original draft: Brenda Baloyi and Solomon Mabapa
Writing – review & editing: Brenda Baloyi, Lindelani Fhumudzani Mushaphi and Solomon Mabapa.
CONFLICT OF INTEREST
The authors declare that they have no financial or personal relationships which may have inappropriately influenced them in writing this article.
ACKNOWLEDGEMENTS
This work is based on research supported by the National Research Foundation (NRF) of SA, and the University of Venda, which are acknowledged for their contributions. The authors would also like to express their gratitude to the research team, the schools and learners who participated in the study
Footnotes
Emails: Brenda.baloyi{at}univen.ac.za; Lindelani.Mushaphi{at}univen.ac.za; Solomon.Mabapa{at}univen.ac.za.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.
- 65.
- 66.↵
- 67.↵
- 68.
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.
- 79.
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵



