
Abstract
Background 1H-MRS is increasingly used in basic and clinical research to explain brain function and alterations respectively. In psychosis research it is now one of the main tools to investigate imbalances in the glutamatergic system. Interestingly, however, the findings are extremely variable even within patients of similar disease states. One reason may be the variability in analysis strategies, despite suggestions for standardization. Therefore, our study aimed to investigate the extent to which the basis set configuration – which metabolites are included in the basis set used for analysis – would affect the spectral fit and estimated glutamate (Glu) concentrations in the anterior cingulate cortex (ACC), and whether any changes in levels of glutamate would be associated with psychotic-like experiences and autistic traits.
Methods To ensure comparability, we utilized five different exemplar basis sets, used in research, and two different analysis tools, r-based spant applying the ABfit method and Osprey using the LCModel.
Results Our findings revealed that the types of metabolites included in the basis set significantly affected the glutamate concentration. We observed that three basis sets led to more consistent results across different concentration types (i.e., absolute Glu in mol/kg, Glx (glutamate+glutamine), Glu/tCr), spectral fit and quality measurements. Interestingly, all three basis sets included phosphocreatine. Importantly, our findings also revealed that glutamate levels were differently associated with both schizotypal and autistic traits depending on basis set configuration and analysis tool, with the same three basis sets showing more consistent results.
Conclusions Our study highlights that scientific results may be significantly altered depending on the choices of metabolites included in the basis set, and with that emphasizes the importance of carefully selecting the configuration of the basis set to ensure accurate and consistent results, when using MR spectroscopy. Overall, our study points out the need for standardized analysis pipelines and reporting.
1 Background
Proton Magnetic Resonance Spectroscopy (1H-MRS) was developed in the late 1980s and has since then become a powerful tool to measure brain metabolites non-invasively. In many neurological and psychiatric diseases, the brain metabolism is altered, leading to changes in metabolite concentrations across the brain. Therefore, 1H-MRS offers a chance for enhancing our understanding of diseases and potentially allowing improvement in developing diagnosis or treatment strategies. By measuring the frequency and intensity of the resonance signals of hydrogen atoms (protons) in certain molecules, 1H-MRS can provide information about the types and amounts of chemicals present in the scanned tissue (1). Among many others, glutamate (Glu) and gamma-aminobutyric acid (GABA) – two of the most important neurotransmitters in the brain – can be detected and quantified in the in vivo brain tissue.
1H-MRS is an extremely important method for psychiatric research. Studies suggest that an imbalance in different neurotransmitter systems, especially the excitatory glutamatergic and the inhibitory GABAergic systems, contributes to the development of the complex set of symptoms in psychotic disorders and autism spectrum disorder (ASD) (2–6). The glutamate hypothesis of schizophrenia, for example, is based on the finding that psychotic symptoms could be induced by antagonists of a glutamate receptor, specifically the N-methyl-D-aspartate (NMDA) receptor (7,8). Changes in glutamate in the anterior cingulate cortex (ACC) (9) and the bilateral medial prefrontal cortex (10) have been linked to psychotic-like experiences in healthy people as well as to symptoms in both first-episode psychosis (11–13) and chronic psychosis (14). In high-risk individuals, structural changes and symptoms seem to be associated with alterations in ACC glutamate concentrations (11). Similarly, in ASD research, studies found increased glutamate concentrations in the ACC in adolescent autistic males (15) and in children (16).
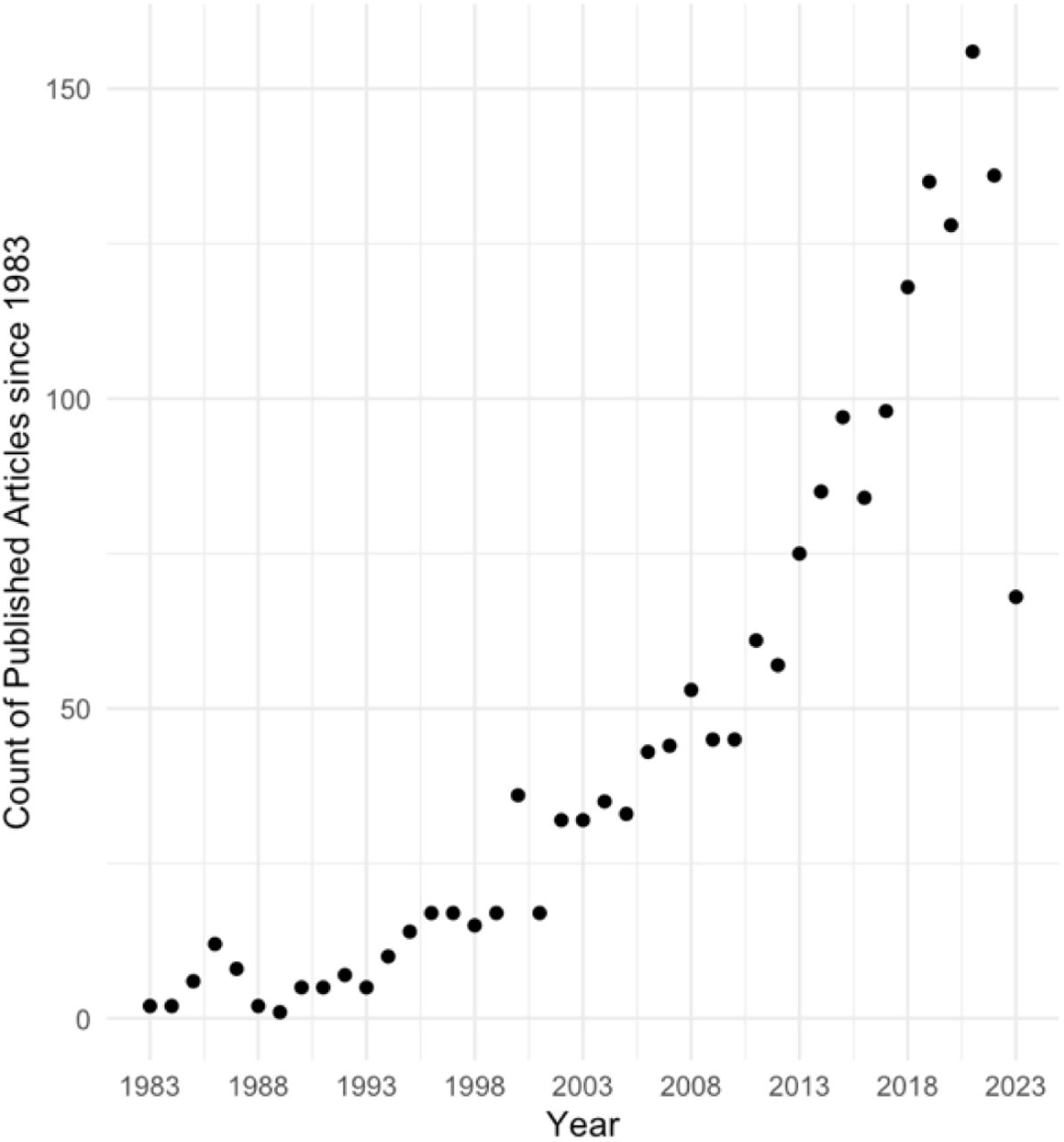
Due to the relevance of this method for understanding the underlying mechanism of psychiatric disorders, the use of this imaging technique has vastly increased, which is illustrated by an exemplary literature search for 1H-MRS and psychotic disorders since the 1980s (Figure 1), and new analysis tools and methods were developed, e.g. FSL-MRS (17), Gannet (18), INSPECTOR (19), Osprey (20), spant (21), and several more. Unfortunately, however, this has resulted in increased variability in the outcomes, which makes it challenging to compare results across studies. Bhogal et al. (22) showed for example, that the metabolite quantification was impacted by the selection of processing parameters and software. But even when using the same software, different processing options had an impact on metabolite quantification. Craven et al. (23) compared seven modelling algorithms for GABA 1H-MRS and detected systematic differences for the metabolite estimates between datasets acquired on hardware from different vendors and across algorithms. These and further studies (24–26), assessing the impact of analysis strategies on metabolite quantification, emphasize the importance of creating standards for 1H-MRS preprocessing, analysis, and reporting schemes. As a consequence, Lin et al. (27) proposed much needed minimum Reporting Standards for in vivo MRS to enhance the reproducibility of study outcomes and to provide a crucial technical assessment of methodologies and analyses. One important aspect that is often neglected is the impact of the basis set composition on the metabolite levels, and whether potential further analyses using these concentrations show inconsistencies. Here we would like to increase the awareness as many scientists who may conduct mainly clinical research might not know of the importance of selecting metabolites included in the composition of the basis set, and may simply follow departmental routines, which might have been set up for different purposes.


As an illustrative example we will concentrate on the investigation of levels of glutamate in patients with psychosis. When investigating levels of glutamate using 1H-MRS assessed in psychosis patients, it becomes apparent that there is considerable inconsistency in the results even within the same region. One study reported higher levels (28), whereas others found reductions (29–31) or no significant differences (32,33) in first-episode psychosis or schizophrenic patients in the ACC. The same irregularity can be found for subjects at risk for psychosis, in the ACC higher (4,11,34–36) and lower (10) glutamate levels, or even no significant results (37–39) have been described. Besides the differences between patient groups, even of the same disease stage (e.g., due to medication status), exact voxel placement, and acquisition with different scanner hardware; one problem, adding heterogeneity to the results, could be the choice of the components of a basis set.
A basis set comprises individual metabolite spectra for quantifying acquired signals (i.e., metabolites of interest) and is used to fit the obtained spectrum. Previous studies showed that a basis set used for the analysis of recorded spectroscopy data crucially requires matching acquisition parameters (i.e., pulse sequence, B0 field strength, time of echo (TE), spectral bandwidth (BW), and data points) with those of the measured spectrum to enable an accurate fitting result (22,40). Importantly, however, also the selection of metabolites represented in the basis set may affect the fit and concentration of the metabolites of interest. For example, when glutathione (GSH) is excluded from the basis set, those metabolites that have overlapping resonance peaks with GSH, such as GABA, glutamine (Gln), and glutamate (Glu), exhibit notable differences in their concentration (41). Therefore, a potential reason for the diversity in the results regarding levels of glutamate in psychosis could be the choice of basis set components. Indeed, basis sets, if reported, vary grossly between studies and are also describing different results (see Table S1). For example, in a study by Shukla et al. (42) glutamate levels in the ACC covarying for age, were significantly higher in controls compared to patients with schizophrenia, using the following basis set components: alanine (Ala), aspartate (Asp), creatine (Cr), GABA, glucose (Glc), Glu, Gln, GSH, glycine (Gly), glycerophosphocholine (GPC), lactate (Lac), myo-Inositol (mI), N-acetylaspartate (NAA), N-acetylaspartylglutamate (NAAG), phosphocholine (PCh), phosphocreatine (PCr), phosphoryl ethanolamine (PE), scyllo-Inositol (sI) and taurine (Tau). Whereas a study by Rowland et al. (43) on patients with schizophrenia found lower levels of ACC glutamate compared to controls, using these basis set components: Ala, Asp, Cr, GABA, Glc, Gln, Glu, GSH, GPC, Lac, mI, NAA, NAAG, PCh, sI and Tau. Especially for clinical research and the ultimate translation into healthcare, it is crucial that potential causes for variability between studies are detected and that guidelines for standardized 1HRS analyses are created. This study, therefore, aims to investigate (1) whether or rather to which extent the choice of metabolites included in the basis set alters spectral fit and/or estimated glutamate concentrations in a voxel; and (2) whether, within and across different basis sets, different representations of glutamate concentrations such as absolute values of glutamate or creatine scales levels of glutamate are differently associated with subclinical traits.
2 Materials and Methods
2.1 Participants
The study population consisted of 53 healthy subjects (age, 23.6 ± 3.8 years; range, 18–35 years) recruited from the general population in Munich, Germany. All participants (26 women, and 27 men) completed two clinical online questionnaires prior to participating in the study at the Technical University of Munich. To assess their psychotic-like experiences, we applied a German translation (44) of the modified version of the Schizotypal Personality Questionnaire (SPQ) (45) using a 5-point Likert scale version. The German translation of the Autism Spectrum Quotient (AQ) (46) was used to capture the autistic traits. Furthermore, we collected their demographic data and medical history during a brief telephone screening. Additional information regarding the inclusion criteria, demographic data, and symptom scores can be found in the supplementary materials (Table S2). The study was approved by the medical research ethics committee of the Technical University of Munich. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
2.2 MR Data acquisition
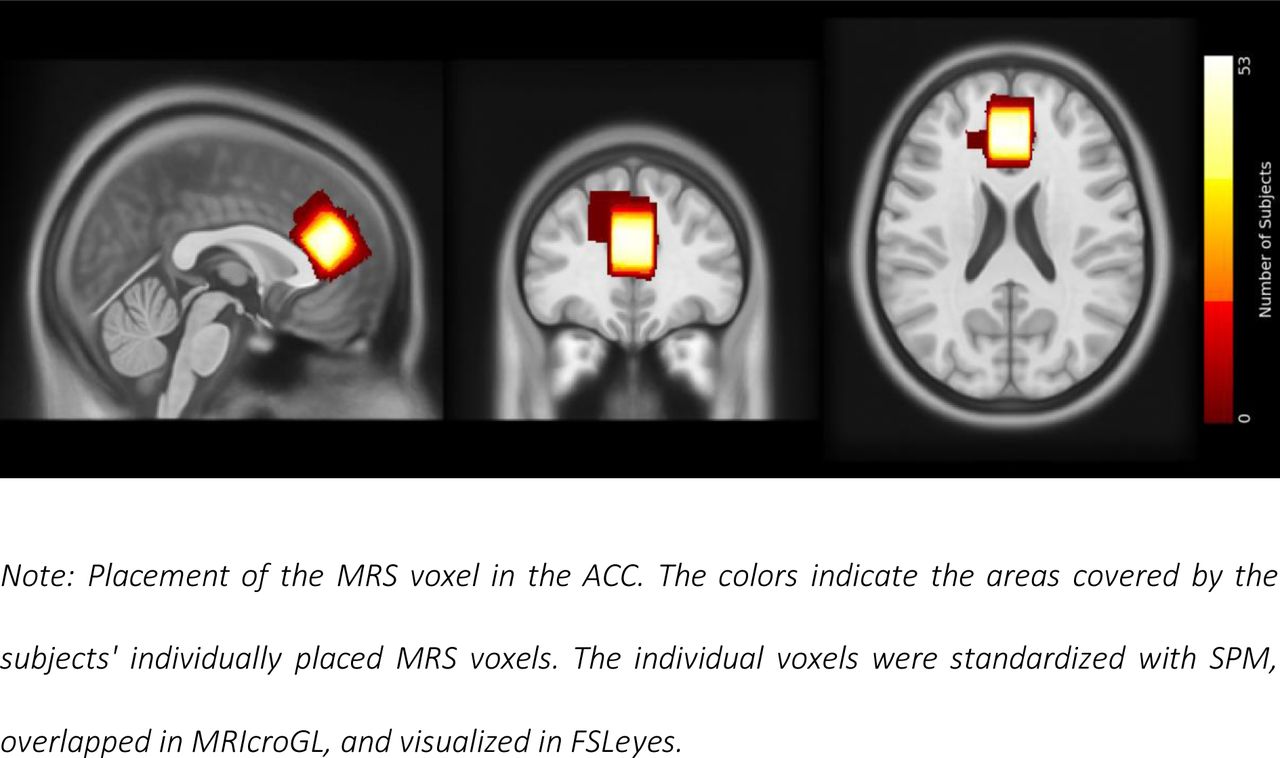
Structural MRI and 1H-MRS data were acquired using a 32-channel head coil on a 3T Philips Ingenia Elition X MR-Scanner (Philips Healthcare, Best, The Netherlands). We obtained T1- weighted magnetization prepared rapid gradient echo (MPRAGE) images for spectroscopic voxel placement and tissue segmentation (TE, 4ms; Repetition Time (TR), 9ms; Flip angle (α), 8°; shot interval, 3000ms; slice number, 170; matrix size, 240×252 and voxel size, 1×1×1mm³). Single-voxel spectra were collected from a voxel (20×20×20mm3) in the ACC. See Figure 2 for voxel placement overlap. Scan parameters for the ECHO volume Point Resolved Spectroscopy Sequence (PRESS) sequence were as follows: TE set to shortest, which resulted in a range of 35.6ms-41.2ms (this is being accounted for in the basis sets); TR, 2000ms; 16 phase cycle steps; acquisition BW, 2 kHz; 1024 data points; flip angle, 90°. To minimize residual water, we used the conventional Philips water suppression technique (excitation) that performs Automatic Water Suppression Optimization (AWSO) pre-scans.

2.3 1H-MRS Processing
The 1H-MRS data were analyzed independently using two different toolboxes: Spectroscopy Analysis Tools (spant) version 2.6.9 (21) (https://martin3141.github.io/spant/index.html) implemented in the open-source R toolbox; and Osprey version 2.4.0, an all-in-one software suite for state-of-the-art processing and quantitative analysis of in-vivo MRS data (20). The scanner’s automatic preprocessing included coil combination, phase-frequency alignment, and averaging of repetitions. In spant, we performed two steps: spectral alignment by referencing the spectrum to the tNAA resonance peak at 2.01 ppm and water removal, which eliminated the residual water signal with a Hankel singular value decomposition (HSVD) filter (47). In Osprey, we excluded eddy-current correction for the automatic preprocessing. Subsequently, Osprey executed the necessary processing steps based on the provided data, including frequency-and-phase alignment, water removal, frequency referencing, and initial phasing. For a more comprehensive overview of the process, see Figure S1.
2.4 Basis sets
Due to the varying TE in our 1H-MRS data between and within the individual voxels, we utilized MARSS in INSPECTOR version 11-2021 (40) to generate six distinct PRESS basis sets for each TE (36, 37, 38, 39, 40, 41), employing a bandwidth of 2000Hz and 1024pts in each simulation. Based on the literature, we selected five different exemplar basis set compositions for illustration. First, Rowland et al. (48) provides evidence for changes in glutamatergic and GABAergic function in relation to the progression of schizophrenia and the manifestation of cognitive and negative symptoms in individuals with schizophrenia. The study utilized a set of 16 metabolite components: Ala, Asp, Cr, GABA, Glc, Glu, Gln, GSH, GPC, Lac, mI, NAA, NAAG, PCh, sI, and Tau. Second, the standard toolbox for 1H-MRS analyses – LCModel – provides a recommendation for the basis set in their manual (49) including 17 metabolites: Ala, Asp, Cr, GABA, Glc, Glu, Gln, GSH, GPC, Lac, mI, NAA, NAAG, PCh, PCr, sI and Tau. Third, Maddock et al. (50) measured glutamate and GABA simultaneously in first-episode psychosis patients and healthy individuals and achieved comparable results for glutamate for the MEGA-PRESS off-resonance to separately-acquired PRESS spectra. They chose 15 metabolites as components of their basis set: Asp, Cr, GABA, Glc, Glu, Gln, GSH, GPC, mI, NAA, NAAG, PCr, PCh, sI, and Tau. Forth, Reid et al. (13) described lower glutamate levels in the ACC in first-episode schizophrenic patients. Their basis set included 19 metabolites: Ala, ascorbate (Asc), Asp, Cr, GABA, Glc, Glu, Gln, GSH, GPC, Lac, mI, NAA, NAAG, PCr, PCh, PE, sI and Tau. Finally, Kozhuharova et al. (10) also simulated 19 basis spectra, which were partially but not fully overlapping with Reid et al. (13), and found lower glutamate levels in high schizotypy individuals in the medial prefrontal cortex, an area often overlapping with the ACC in 1H-MRS studies. Their basis set contained: Ala, Asc, Asp, Cr, GABA, Glc, Glu, Gln, glycine (Gly), GSH, GPC, Lac, mI, NAA, NAAG, PE, PCh, sI, and Tau. We added the default macromolecular and lipid components provided by spant or Osprey.
2.5 Spectral Fitting
Spant uses an adaptive baseline fitting algorithm (ABfit) (51), which accurately estimates the optimal baseline – hereafter referred to as spant+ABfit. This is important because the smoothness of the baseline is a critical analysis parameter for metabolite estimation. Additionally, spant combines the capabilities of R with a blend of conventional and up-to-date MRS data processing methods, enabling it to perform a fully automated routine MRS analysis (21). We performed the segmentation of the structural T1 image into grey matter (GM), white matter (WM), and cerebrospinal fluid (CSF) using SPM12 (52). For estimation of absolute levels of glutamate (absolute Glu), we utilized the ABfit method to quantify glutamate into a tissue and relaxation-corrected molal glutamate concentration (mol/kg). The correction for tissue fractions was applied using the method described by Gasparovic and colleagues (53).
In Osprey, we used the LCModel (LCM) implementation to fit and quantify our data, hereafter referred to as Osprey+LCM. The LCModel algorithm fits spectra in the frequency domain using a linear combination model (54). The processing adhered to standard parameters, employing a metabolite fit range spanning from 0.5 to 4.0 ppm and a water fit range ranging from 2.0 to 7.4 ppm. A knot spacing of 0.4 ppm was utilized. Osprey calls the SPM12 (52) segmentation function to segment the structural image into tissue probability maps. These are then overlaid with the coregistered voxel masks, created by the Coregistration module, to calculate the fractional tissue volumes for GM, WM, and CSF. For the estimation of absolute levels of glutamate (absolute Glu), Osprey+LCM estimates the tissue and relaxation corrected molal concentration (mol/kg) according to the Gasparovic method (53).
We ran the analysis in both tools for all five basis sets separately. Afterwards, we extracted the scaled estimates for Glu (Glu/tCr), absolute Glu and Glx (Glu+Gln). Note that the basis set of Kozhuharova (10) and Rowland (48) did not include PCr, so the scaled estimates for Glu were calculated to Cr instead of tCr.
2.6 Quality assessment
Quality parameters used in this study were the Signal-to-Noise Ratio (SNR), the Full Width at Half Maximum (FWHM) and the Cramer-Rao lower bounds (CRLB). However, we would like to point out that the two analysis tools differently determine some of them. Spant+ABfit calculates the SNR by taking the signal from the maximum point in the fit and subtracting the mean noise value after fitting the data (spant(21): calc_spec_snr). Thus, it is dependent on the baseline intensity. In Osprey+LCM, however, the SNR is calculated by dividing the amplitude of the NAA peak by the standard deviation of the detrended noise in the range of -2 to 0 ppm (20).
Osprey+LCM reports the linewidth as the width of the water peak at half the maximum amplitude calculated as the average of the FWHM of the data and the FWHM of a Lorentzian fit. The threshold was set to the resulting water FWHM > 13 Hz according to recommendations for B0-shimming provided by Juchem et al. (55). In spant+ABfit, the linewidth was given in ppm as tNAA linewidth, full-width half-maximum of a single-Lorentzian fit to the NAA peak (between 1.8 and 2.2 ppm). Based on a consensus paper by Wilson et al. (56), a FWHM greater than 0.1 ppm should be regarded as being of poor quality.
Further exclusion criteria for both analysis methods included either a visual failure of the fitting algorithm or CRLB exceeding 20% for Glu and Glx. Based on these criteria, no subject had to be excluded.
2.7 Analysis of group differences between the different basis sets
All statistical analyses were performed using R Statistical Software (version 4.2.2) (57). We tested the different metabolite concentrations across all basis sets for normality using the Shapiro–Wilk method (58) (stats package (57), version 4.2.2) and for homogeneous distribution of their variances by the Levene’s test (59) (cars package (60), version 3.1-1). As the normality assumption and the homogenous distribution of variances were not fulfilled for the metabolite concentrations (Glu/tCr, absolute Glu and Glx) and the spectral quality parameters(Glu CRLB and Glx CRLB), we used the Friedmann test (61) (rstatix package (62), version 0.7.1) to determine group differences across the different basis sets. For post-hoc multiple pairwise-comparison between basis sets, we applied the paired Wilcoxon signed-rank test (63) (rstatix package (62), version 0.7.1). For the group comparison of the SNR, we computed repeated measures ANOVA and multiple pairwise paired t-tests (rstatix package (62), version 0.7.1). P- values were adjusted using the Bonferroni multiple-testing correction method. An adjusted p- value <0.05 was considered significant. The differences were visualized with boxplots with the ggpubr package (64) (version 0.5.0).
2.8 Correlation analysis of each metabolite concentration between the basis sets
To investigate the comparability between all our results, we calculated Spearman’s rank correlation coefficients as the normality, linearity, and homoscedasticity assumptions were not met, between the results of the different basis sets and toolboxes for each metabolite estimate (Glu/tCr, absolute Glu, Glx). For these correlation analyses, we used the stats package (57) (version 4.2.2). The correlation heat maps were visualized with the ggcorrplot package (65) (version 0.1.4).
2.9 Association between the concentrations and traits
Finally, we explored the relationship between the different metabolite concentrations and clinical scores. First, we factored the SPQ score into positive-like symptoms, negative-like symptoms, and disorganized traits (66). Then, we calculated Spearman’s rank correlation coefficients using the SPQ subscales and autistic traits together with the different metabolite concentrations. The correlation analyses were performed in R using the stats package (57) (version 4.2.2). The visualization of the correlation heat maps was created with the ggcorrplot package (65) (version 0.1.4).
3 Results (687)
3.1 Spectral quality
All acquired spectra were of good quality with CRLB < 10%, SNR > 60 and for spant FWHM < 0.06 ppm or for Osprey FWHM < 8 Hz. Example fits for the different basis sets are shown in Figure 3. Examining the residuals at the top of every plot, we can see that the fitted models of the basis sets from the LCModel Manual (49), Maddock et al.(50), and Reid et al. (13) had the best fit indicated by lowest fluctuations. Comparing CRLB of Glu and Glx between the basis sets, we found significant overall effects (spant+ABfit: CRLB Glu X2 = 40.33, p<0.0001; CRLB Glx: X2 = 12.40, p=0.0146; Osprey+LCM: CRLB Glu X2 = 17.45, p=0.0016; CRLB Glx: X2 = 27.47, p<0.0001) (Table S3). Pairwise post-hoc analyses for CRLB of Glu revealed differences between the basis sets of Rowland et al. (48) and Reid et al. (13) spant+ABfit, and Osprey+LCM and between Maddock (50) and Reid (13) in spant + ABfit (Table S5). Pairwise post-hoc analyses for CRLB of Glx showed significant differences between the basis sets of Maddock et al. (48) and Kozhuharova et al. (10) in spant+ABfit, and Osprey+LCM, and several more in Osprey+LCM (Table S6). Furthermore, we compared SNR between the basis sets (Table S3). In spant + ABfit, but not Osprey, we found differences in SNR among the fitted models (F1.68, 87.49 = 31.03, p <0.0001). Lastly, we compared FWHM for spant+ABfit between the basis sets (Table S3), which revealed a significant difference (X2 = 150.7, p <0.0001). Post-hoc results are presented in Table S7. FWHM for Osprey+LCM showed identical results across basis sets due to analysis method and was not statistically compared.

3.2 Group differences between the metabolite concentration estimates
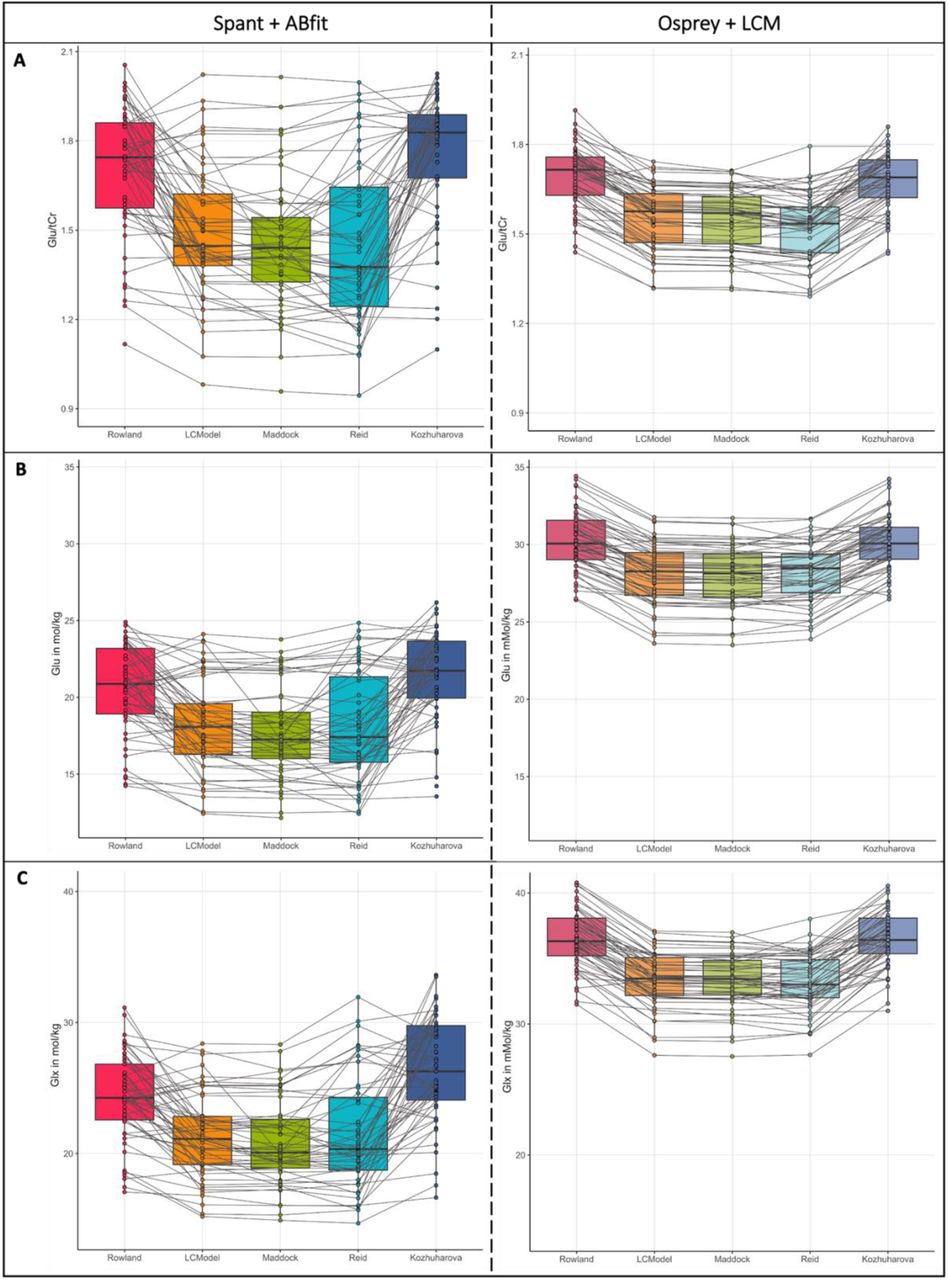
Comparisons between the estimates for Glu/tCr, absolute Glu, and Glx are summarized in Figure 4, results are presented in Table S8-11. The Friedmann test (61) showed significant group differences for t Glu/tCr, absolute Glu, and Glx with always p < 0.0001. Estimates were consistently lower for the analysis in spant+ABfit compared to the ones analyzed with Osprey+LCM. Based on the visualization of the individual data points and their connection over the different basis sets, we found a higher heterogeneity of the metabolite concentration estimates in spant+ABfit compared to Osprey+LCM.


3.3 Correlations of each metabolite estimate between the basis sets
Correlations between metabolite (Glu/tCr, absolute Glu, Glx) and basis set per toolbox reveal that the metabolite concentrations between the basis sets had higher correlations using Ospreys LCM integration than spant+ ABfit. For Osprey+LCM, we found strong correlations between all basis sets (r>0.75). The quantification results in spant+ABfit showed a much higher variability. We found weak, moderate, and strong correlations. Overall, the three visually best-fitting basis sets (LCModel Manual (49), Maddock et al. (50), and Reid et al. (13); Figure 3 B, C, and D) showed the best results with spearman correlation coefficients between 0.93-1 for Osprey+LCM and 0.88-0.94 for spant+ABfit (Figure 5). Another notable aspect is, that the two basis sets Rowland (48) and Kozhuharova (10), which both do not include PCr in their basis set composition, showed a strong correlation within each analysis tool, Osprey+LCM and spant+ABfit. Between the toolboxes, the correlations were weak to moderate. Correlation strength was classified according to Akoglu (67).

3.4 Association between the concentrations and traits
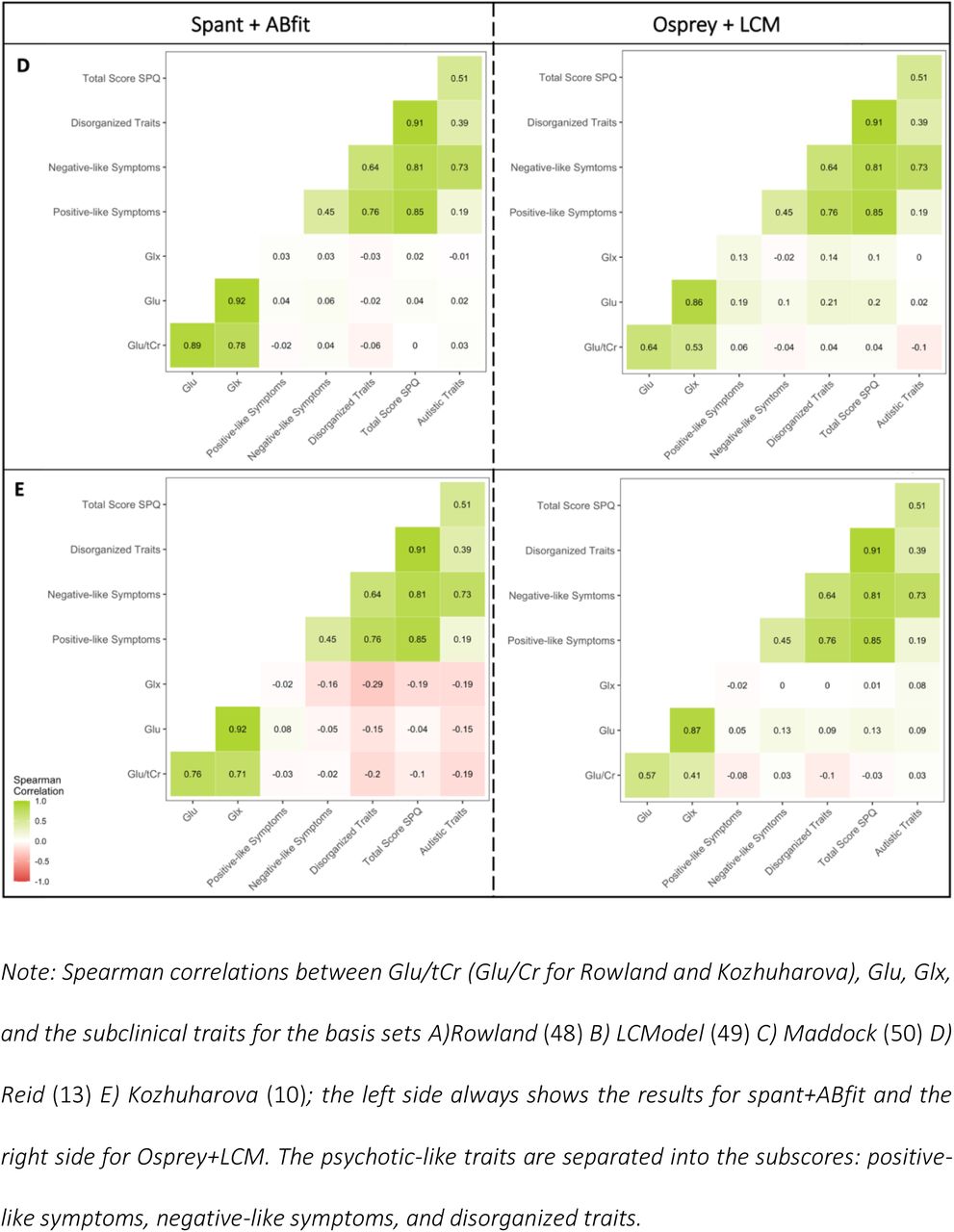
Finally, we analyzed Spearman’s rank correlations for clinical scores with the extracted concentration scores. Overall, the results in Osprey+LCM displayed a more homogenous pattern regarding the tendency of their non-significant correlations with a maximum difference of 0.18 between the coefficient scores for the correlation of Glx and disorganized traits, whereas in spant+ABfit the correlations coefficients showed greater variability ranging from positive to close to negative values, with a maximal difference of 0.42 for the same correlation. These results also indicated that the correlation coefficients differed between the two toolboxes. However, the difference between the toolboxes was smaller than the difference across the different basis sets, and reached a maximum of 0.29 again for the correlation of Glx and disorganized traits. The correlations are shown in Figure 6.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
4 Discussion
In this study, we investigated whether the choice of metabolites included in the basis set for a 1H-MRS analysis alters spectral fit and/or estimated glutamate concentrations in a voxel placed in the ACC. Importantly, we examined whether potential changes in glutamate concentrations were differently associated with schizotypal and autistic traits. For comparability, we contrasted the effects using five basis sets used in psychosis research and two different analysis tools (i.e., spant+ABfit, Osprey+LCM). We found that (1) glutamate concentrations differed significantly depending on the metabolites included in the basis set with those including phosphocreatine (PCr) showing more consistent results; (2) differences in concentration between the basis sets were similar across the different types of concentration estimates (i.e., absolute Glu, Glx, Glu/tCr); (3) fit and quality measures revealed differences, again with those including phosphocreatine showing better results; and finally (4) concentrations estimated based on different basis sets led to varying symptom correlations, with differences between basis sets being larger than between toolbox, although, Osprey+LCM showed greater consistency in the results compared to spant+ABfit.
Our results indicate that those basis sets containing PCr (i.e., Reid (13), Maddock (50), LCModel Manual (49)) showed better spectral fit and more consistent levels of glutamate. This effect was similar across the different types of concentrations (i.e., absolute Glu, Glx, Glu/tCr). This may be due to the robustness and well-defined chemical shift of the PCr within the MRS spectra of a voxel, which may be caused by its a relatively high and stable concentrations across the brain (68,69). Therefore, basis sets which did not include PCr may produce more variability in the data due to a worse fit. Interestingly, the inclusion of PCr seems to override differences regarding to the number of metabolites included between the basis sets, as Maddock et al (50) include four spectra less compared to Reid et al (13). This result was consistent between both toolboxes, spant+ABfit and Osprey+LCM. To test this, we added the metabolite PCr to the basis sets of Rowland (48) and Kozhuharova (10) and re-ran the analyses. The new Rowland basis set with PCr was now identical to the basis set of the LCM Manual. Interestingly, after adding PCr, both basis sets produced comparable results to those basis sets containing PCr from the beginning (i.e., Reid (13), Maddock (50), LCModel Manual (49)), see Figure S2 and S3. Here, our results seem to identify PCr as a crucial metabolite for the fitting of different glutamate concentrations (i.e., absolute Glu, Glx, Glu/tCr).
This result was confirmed by the finding that those three basis sets containing PCr also showed the strongest intercorrelations (r=0.88-1) across all different concentration types within the same toolbox. Across the toolboxes, correlations were weaker. However, the three basis sets containing PCr showed the strongest (r=0.39-0.47) and most consistent correlations across the three glutamate concentrations. Furthermore, those three basis sets also showed significantly less variation compared to the other two basis sets.
When comparing SNR between the basis sets, we found differences in spant+ABfit, but not in Osprey+LCM, where values are identical across the fitted models. This may be explained by the different methods used for SNR calculation. These processing differences may account for the fact that differences were detected in spant+ABfit but not Osprey+LCM.
Considering the results of this study and the inconsistencies reported in the literature regarding, for example, differences in glutamate concentrations in psychosis patients (4,70,71), one pressing question is whether the latter variability is further increased or partially caused by the differences in analysis strategies and parameters, for example the choice of metabolites included in the basis set but also the analysis software or toolbox itself. While there is further variation due to voxel size and placement, analysis software, analysis parameters and field strength (29–31), the configuration of the basis set is easily controllable, and would potentially reduce the variability in the results across studies, for example in psychosis research (29–31). For different measures of glutamate (i.e., absolute Glu, Glx, Glu/tCr), this study indicates that the inclusion of PCr is crucial. However, more research is needed to confirm these results especially using clinical populations. This emphasizes once more that guidelines for 1H-MRS analysis (27,55,56,72), especially the configuration for basis sets to estimate concentrations of much studied metabolites, such as glutamate, are essential in order to produce reliable research that allows translational and clinical implications. The findings discussed here are highly important as treatment options are being discussed (29,73) on the basis of findings that may be impacted by analysis choices.
This study has several limitations. First, we analyzed only one voxel in the ACC, and chose five different, exemplar basis sets and we used two different analysis software tools. Although, those choices are not comprehensive, they provide some important insights and they were motivated based on published research, and demonstrate possible analysis strategies. Future research should replicate these analyses in different brain areas, and potentially using additional basis sets and analysis tools. However, the most insightful strategies would be to run a phantom study, which assess the accuracy and stability of levels of glutamate with different basis sets (74). Second, we used personality traits in a healthy general population sample.
Therefore, the distribution of a clinical expression of symptom scores is skewed, and possible effects may be less prominent compared to potential effects in clinical groups. Interestingly, however, even with trait makers that are relatively low our results show differences of the magnitude of a weak to moderate correlation, indicating the impact of analysis choices. Third, our sample was moderate in size with 53 subjects. With larger cohorts, results may stabilize. Nevertheless, one should consider that many patient studies have smaller sample sizes with cohorts of 20-30 subjects. Therefore, it is extremely valuable to show the impact of analysis choices on smaller cohorts. Fourth, we did not calculate test-retest reliability for evaluating individual differences and establishing a certain robustness of our results as we did not conduct a follow-up measurement. This and an experimental quantification of the glutamate would be needed to objectively state the best basis set composition. Fifth, as the focus of this study was to increase the awareness of the matter, we are unable to provide specific recommendations regarding the aspects of preprocessing and analysis methods. However, future studies specifically designed to assess the best fitting basis set composition should provide those, that ought to be part of the minimum Reporting Standards for in vivo Magnetic Resonance Spectroscopy.
In conclusion, our study demonstrates the importance of using consistent basis set compositions for accurate spectral fitting but especially for comparable generation of metabolite estimates. This requires a standardized analysis approach. Potential consequences of the variability in the analysis techniques and strategies used in current research become apparent in the differences of symptoms correlations depending on analysis choices. Therefore, this study once more emphasizes the need for standardized analysis and reporting guidelines in spectroscopy but also imaging research in general.
5 Declarations
Ethics approval and consent to participate
The medical research ethics committee of the Technical University of Munich gave ethical approval for this work. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable
Availability of data and materials
The datasets generated and/or analysed during the current study are available in the OSF repository, [https://osf.io/zjtd8/?view_only=9763e1e752e7409892730ecafed71bf7].
Competing interests
The authors declare that they have no competing interests.
Funding
This work was supported by the doctoral program “Translationale Medizin” of the Technical University of Munich funded by Else Kröner-Fresenius-Stiftung (EKFS) to VD.
Authors’ contributions
VFD, FK, CZ conceptualization; VFD, FK, EFS data collection; VFD, FK formal data analysis; MW advise on formal analysis; FK, VFD writing for first draft; VFD, FK, MW, EFS, CZ editing and reviewing of manuscript.
Data Availability
The datasets generated and/or analysed during the current study are available in the OSF repository, [https://osf.io/zjtd8/?view_only=9763e1e752e7409892730ecafed71bf7].
https://osf.io/zjtd8/?view_only=9763e1e752e7409892730ecafed71bf7
Acknowledgements
We would like to thank all participants for their time and engagement.
Footnotes
The abstract was structured for more clarity. In the background section, we clarified the goal of the study - increasing the awareness of the impact of the basis set composition. In the methods section, the subheader "2.6Quality assessment" was added to give more details on the MRS analysis quality parameters (SNR, FWHM and CRLB). In the supplements, we added the subheader "4.3 Association between the concentrations and traits" to strengthen our finding that those basis sets including phosphocreatine (PCr) showed more consistent results. Figure S2 was attached to the supplements showing the group comparisons and Spearman correlations for those newly created basis sets.
6 List of abbreviations
- 1H-MRS
- Proton Magnetic Resonance Spectroscopy
- ABfit
- Adaptive baseline fitting algorithm
- ACC
- Anterior cingulate cortex
- AQ
- Autism Spectrum Quotient
- ASD
- Autism spectrum disorder
- Asp
- Aspartate
- AWSO
- Automatic Water Suppression Optimization
- BW
- Spectral bandwidth
- Cr
- Creatine
- CRLB
- Cramer-Rao lower bounds
- CSF
- Cerebrospinal fluid
- FWHM
- Full Width at Half Maximum
- GABA
- Gamma-aminobutyric acid
- Glc
- Glucose
- Gln
- Glutamine
- Glu
- Glutamate
- Gly
- Glycine
- GM
- Grey matter
- GPC
- Glycerophosphocholine
- GSH
- Glutathione
- HSVD
- Hankel singular value decomposition
- Lac
- Lactate
- LCM
- LCModel
- MI
- Myo-Inositol
- MPRAGE
- Magnetization prepared rapid gradient echo
- MRS
- Magnetic Resonance Spectroscopy
- NAA
- N-acetylaspartate
- NAAG
- N-acetylaspartylglutamate
- NMDA
- N-methyl-D-aspartate
- PCh
- Phosphocholine
- PCr
- Phosphocreatine
- PE
- Phosphoryl ethanolamine
- PRESS
- Point Resolved Spectroscopy Sequence
- SI
- Scyllo-Inositol
- SNR
- Signal-to-Noise Ratio
- spant
- Spectroscopy Analysis Tools
- SPQ
- Schizotypal Personality Questionnaire
- Tau
- Taurine
- TE
- Time of echo
- TR
- Repetition Time
- WM
- White matter
7 References



