
Abstract
Background Multiple sclerosis (MS) is a debilitating demyelinating disease and recent evidences are giving cues towards correlation of disease severity to gut microbiome dysbiosis. However, there haven’t been any reported interventions that beneficially modifies the gut microbiome to yield a clinically discernible improvement. Having earlier reported the clinical effects of a biological response modifier beta-glucan (BRMG) produced by the N-163 strain of Aureobasidum pullulans, commercially available as Neu-REFIX, which decreased the biomarkers of inflammation and produced beneficial immune-modulation in twelve MS patients in 60 days, we evaluated their gut microbiome in the present study.
Methods Twelve patients diagnosed with MS participated in the study. Each consumed 16 g gel of the NEU-REFIX beta-Glucan for 60 days. Whole genome metagenomic sequencing was performed on the fecal samples before and after Neu-REFIX intervention.
Results Post-intervention analysis showed that Actinobacteria followed by Bacteroides was the major family. Abundance of beneficial genera such as Bifidobacterium, Collinsela, Prevotella, Lactobacillus and species such as Prevotella copri (p-value=0.4), Bifidobacterium longum (p-value=0.2), Faecalibacterium prausnitzii (p-value=0.06), Siphoviridae (p-value=0.06) increased while inflammation associated genera such as Blautia (p-value=0.06), Ruminococcus (p-value=0.007) and Dorea (p-value = 0.03) decreased in abundance.
Conclusion Restoration of gut eubiosis in terms of both increase in abundance of the good microbiome and suppression of the harmful ones which also correlate with earlier reported clinical improvement in MS patients makes this Neu-REFIX beta-glucan, a potential disease modifying therapy (DMT) requiring larger studies for validation in MS and other auto-immune-inflammatory conditions where a safe intervention for immune modulation is vital.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune condition that causes demyelination, axonal loss, and inflammation of the central nervous system (CNS). There are 2.5 million people with MS worldwide and it imposes severe burden on the affected patients, their families and the society as a whole. Although the exact cause of MS is unknown, host genetics and environmental variables have been theorised to play a role. MS is a diverse illness that is influenced by both environmental and genetic factors, such as the relationship with HLA-DRB1*15:01 and vitamin D status, obesity, smoking, and Epstein-Barr virus (EBV) infection. MS patients’ dysregulated immune responses and aberrant metabolism raise the possibility that the disease’s pathogenesis involves a number of systems [1]. MS pathogenesis is influenced by changes in the peripheral immune system, blood brain barrier permeability, and intrinsic CNS immune cells (such microglia). Neurodegeneration and acute and chronic inflammation both occur over the course of the illness, with acute inflammation being more prominent during the relapsing phase. Although the question of whether MS is neurological or autoimmune by origin is still being debated, majority of genetic profiling demonstrates a preponderance of immune-mediated molecules that are activated during the illness process. Both innate and adaptive immune responses play a role, as shown by animal models and clinical findings in MS patients. Myeloid-derived macrophages and microglia are innate immune cells that play important roles in MS. Autoimmune CD4+ T cells, in particular Th1 cells that are reactive to myelin proteins, and CD8+ cytotoxic T cells are adaptive immune cells that are involved in MS. B cells have a significant role in the pathogenesis of human MS through the generation of proinflammatory cytokines and chemokines, antibody creation, and antigen presentation to T cells [1]. Multiple pathogenic mechanisms, including activated microglia, leptomeningeal inflammatory infiltrates causing subpial demyelination, mitochondrial dysfunction and oxidative injury driven by macrophages and microglia, are thought to contribute to the development of progressive MS [2].
In this background, the role of the gut microbiome which has a bi-directional influence on the central nervous system, immune and inflammation mediated processes is becoming increasingly associated with the initiation and progression of MS. Changes in the gut microbiota trigger immunological and physiological changes in the host, which are crucial for preserving the gut microbiota’s homeostasis. The intricacy of the gut environment, as currently understood, points to the importance of dysbiosis, which is defined as changes in the microbiome’s composition acting as a potential disease-causing mechanism. Dysbiosis can impact immune reactions to the microbiota, but it can also negatively impact the integrity of the epithelia, which form cellular barriers necessary to preserve the health of the intestine and the central nervous system (CNS) [3].
We have earlier reported the beneficial effects of N-163 strain of Aureobasidium pullulans, produced biological response modifier beta-glucan (BRMGs), trade name - Neu-REFIX on the gut microbiome in pre-clinical and clinical studies in Non-alcoholic steatohepatitis (NASH) [4] and Duchenne muscular dystrophy (DMD) [5]. These effects included the regulation of gut dysbiosis, enhancement of butyrate producers, and metabolites, including endogenous butyrate production and amino acids. Importantly, these results correlated with the improvement in the clinical parameters of relevance [6,7].
The clinical improvement in immunological and inflammatory parameters such as decrease in IL-6, improvement in CD4+ve, CD19+ve, CD3+ve, and CD8+ ve cell count, increase in Lymphocyte to C-reactive protein ratio (LCR), Leukocyte to CRP ratio (LeCR) and a decrease in Neutrophil to Lymphocyte ratio (NLR) apart from improvement in Kurtzke’s expanded disability severity score (EDSS) have been studied in the clinical trial done in MS patients [8].
In the same patients, in the current study, we have evaluated the effects of this Neu-REFIX on their gut microbiome.
Methods
This trial was an open label, prospective, non-randomised, non-comparative single arm clinical study. The study was of 60 days duration. The inclusion and exclusion criteria are available in the study on clinical parameters reported earlier [8]. Patients with MS diagnosed as per McDonald diagnostic criteria (2005) were included in the study.
Prior to the study, the patients’ treatment plans varied in terms of the medications they took and how long they were given to work, but the majority of them included steroids, muscle relaxants, and in the case of some patients, interferon beta-1b (IFNB) and immunomodulators like alemtuzumab, fingolimod, or natalizumab.
In addition to their above-mentioned standard treatment plan, the patients took two sachets of the N-163 strain of A.pullulans (each sachet of 8g gel contains 48 mg of active substance; trade name: Neu-REFIX) produced beta-glucan, every day along with a meal for 60 days.
Using a sterile faeces collection kit (OMNIgene Gut collection kit), faeces samples were taken from all the subjects at baseline and 60 days after the intervention. DNA extraction was performed and samples were stored at minus 80 °C until they were needed for analysis. Following the manufacturer’s instructions, total microbial DNA was extracted from each sample of faeces using the QIAamp DNA Mini Kit (Qiagen). An extraction control (negative buffer control) was used to extract each group of samples.
The samples were sequenced using Novaseq V1.5 with a read length of 151 bp. The samples were subjected to whole genome metagenome analysis. Initially, the reads were filtered for human DNA contamination. The alignment to human genome was around 0.01% - 1.6%. The filtered reads were further used downstream analysis. De novo metagenome assembly was carried out using Megahit assembler. Assembly was performed using de-Bruijn graph method.
The assembled scaffolds were taken for further downstream analysis. Open reading frame (ORF) prediction was done using Prodigal (v2.6.3). The assembled scaffolds from the de novo assembly was taken for the ORF prediction. The obtained ORFs were filtered using in house Perl scripts. ORFs of length below 200 bp were filtered out. The abundances at the phylum, genus and species level were evaluated. Pair-wise comparison phylum to species taxapair-wise comparison phylum to species taxa was performed
Statistical data were analyzed using GraphPad Prism software. The statistical significance level was set at 5%. Non-parametric tests such as Mann Whitney test for independent measures were employed were used for metagenomic sequencing data, including taxonomy.
Results
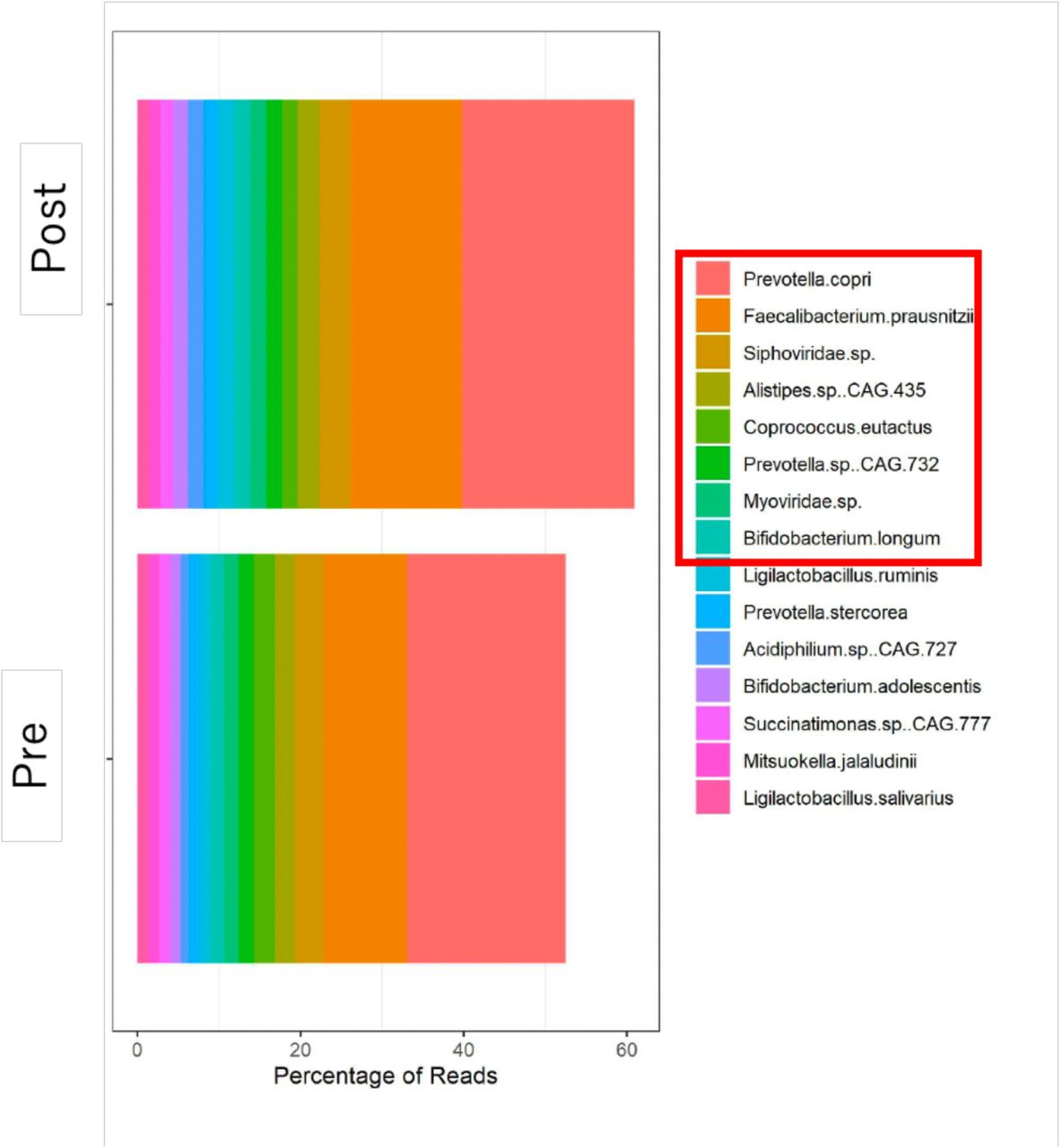
Gut bacterial gene richness were similar pre-and post-intervention. Post-intervention, the abundance of Actinobacteria, Bacteroidetes and Proteobacteria increased at genus level (Figure 1). At phylum level, post-intervention, Bifidobacterium, Prevotella, Collinsella increased while Blautia and Dorea decreased (Figure 1). When individual species and genera were analysed (Figure 2), there was increase in mean abundance of Bifidobacterium longum from 1.01 ± 0.8 to 1.3 ± 0.8 (p-value= 0.2), Prevotella copri from 6.529 ± 11.14 to 7.22 ± 12.13 (p-value= 0.4), Faecalibacterium prausnitzii from 4.7 ± 4.2 to 7.29 to ±4.54 (p-value= 0.06), Siphoviridae sp from 2.79 ± 1.8 to 2.97 ± 1.9 (p-value= 0.06) (Figure 3). The mean abundance of Blautia decreased from 0.24 ± 0.l8 to 0.01 ± 0.05 (p-value = 0.003), Dorea decreased from 0.63 ± 0.77 to 0.33 ± 0.73 (p-value = 0.03) and Ruminococcus decreased from 0.93 ± 0.56 to 0.37 ± 0.31 (p-value = 0.007) post intervention (Figure 4).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
Multiple sclerosis (MS) is one of the rare demyelinating, devastating diseases which has very complex pathogenesis, ambiguous aetiology and extensive heterogeneity in terms of clinical features, genetics, pathogenesis and responsiveness to treatments. The clinical course of MS is either relapsing-remitting (RR), which represents around 60% of prevalent cases, or progressive [9]. About 10% of MS cases have a primary progressive (PP) course, while transition to the secondary progressive (SP) phase occurs in around half of RR MS. Standard care of treatments include DMTs such as interferon beta (IFNB) 1-a and 1-b, glatiramer acetate (GA), mitoxantrone, natalizumab, fingolimod, teriflunomide, dimethyl fumarate, and alemtuzumab, off label use of azathioprine, cyclophosphamide, methotrexate and rituximab but most of these treatments are associated with increased risk of serious adverse events, which may even be fatal in rare cases [9]. Therefore, there is a need to develop safe DMTs. With reference to the aetiology of the disease, there are several hypothesis of environmental, genetic factors, such as the relationship with HLA-DRB1*15:01 and vitamin D status, obesity, smoking, auto-immune and Epstein-Barr virus (EBV) infection [1]. However, the DMTs mentioned above are not specific and efficacy still is largely limited with neurological disability continuing to worsen over time. Specific targeted immune-suppression is also not possible with these DMTs.
In this background, the only solace is the correlation of gut microbiome and disease severity which opens a new avenue to explore gut microbiome based approaches as the pathophysiology of MS appears to be significantly influenced by the gut flora, and it appears to be involved in controlling the host’s immune system, affecting the BBB’s integrity and functionality, causing autoimmune demyelination, directly engaging many CNS cell types. In earlier studies, when compared to healthy individuals and MS patients in the remittent phase, people with MS in the relapse phase exhibited increase in firmicutes and a decline in the phylum Bacteroidetes [10–12]. Additionally, it was discovered that Prevotella had decreased. Prevotella has been shown to reduce the anti-inflammatory metabolite propionate and therefore its decrease in MS is harmful. Genera like Blautia, Ruminococcus and Dorea have been reported to be in greater abundance in patients with MS compared to healthy controls [13]. Instead, the prevalence of Bacteroidetes genera like Parabacteroides, Bacteroides, and Prevotella was reduced [10–12]. Because they may activate IFN, metabolise sialic acids, and breakdown mucin, certain species of Dorea may be pro-inflammatory, according to research by Schirmer et al [13]. In light of this, Dorea could serve as an illustration of a bacterium that shows pro or anti-inflammatory functions depending on the nearby gut flora and/or nutrients that are accessible. In fact, since Blautia uses the gases generated by Dorea, a higher concentration of Dorea in MS patients may encourage the formation of Blautia [12]. Bifidobacteria may play a protective function in MS, according to a number of lines of evidence. Numerous strategies, such as a change in lipid profile, stimulation of Treg differentiation, and modification of the Th1/Th2 balance, might be the mechanisms underlying such a protective impact [14]. Due to its function in butyrate generation, Faecalibacterium is linked to a decreased inflammatory state, and methods to increase Faecalibacterium abundance have been proposed as potential treatments for ulcerative colitis patients. Earlier reports have shown that subjects with increased Caudovirales and Siphoviridae levels in the gut microbiome had better performance in executive processes and verbal memory [15]. All these studies have only reported a correlation of gut microbiome to the disease severity of the disease. However to our knowledge, till date, there has been no study which has reported an intervention that has relevance to clinical outcome and the gut microbiome. Herein comes our study’s results wherein a clinically encouraging outcome in terms of EDSS, inflammatory and immune-modulatory biomarkers which was earlier reported [8], which in follow-up of evaluation of gut microbiome in our present study, a striking increase in beneficial bacteria with a significant reduction in harmful bacteria, we have been able to prove. In our study there has been an increase in phylum Bacteroidetes and Prevotella post-intervention. There is a reversal effect of decrease in genera like Blautia, Ruminococcus and Dorea with increase in Bacteroidetes, Bifidobacterium, Faecalibacterium and Siphoviridae levels in our study which is beneficial.
While the relevance of gut microbiome has been reported in several earlier studies, manipulating it beneficially involves methods like fecal microbiota transplantation (FMT) or probiotics which essentially are exogenous supplementation of beneficial microbiome [16]. However, they don’t essentially address the harmful bacterial colonies and their metabolites and the environment. Our approach does both; decreasing the abundance of harmful organisms while increasing the beneficial ones more in an endogenous manner apart from immune modulation and producing clinically relevant outcome. Further, the Neu-REFIX Beta-Glucan is safe and is easily consumable making it a potential disease modifying adjunct for MS both clinically and in relevance to the gut microbiome.
Limitations of the study include small sample size, heterogenous presentation of MS, geographical influences as this study consisted of participants of Indian ethnicity alone while western populations have reported a higher prevalence of MS. Therefore further validation in different populations with global multi-centric clinical trials is needed. Now having found a small step in beneficial reconstituting the gut microbiome in this pilot clinical study, an in depth exploration is needed to find if gut dysbiosis is a cause or effect in the background of underlying inflammation in response to an unknown antigen. This question may have been partially answered in this study because Neu-REFIX beta-glucan has shown beneficial effects of restoring the gut microbiome and also the improvement in clinical parameters could be attributed as an effect. Going by the earlier reports of gut dysbiosis caused by specific drugs in neurological illness [17,18], in line with those evidences, whether similar drugs are part of MS regimen have to be looked into or diseases that have direct correlation to gut dysbiosis when subjected to a clinical study, the appropriate drug or molecule should be studied for implications on gut microbiome as well.
Conclusion
In this pilot clinical study of patients with MS, who have reported improvement in clinical biomarkers of inflammation and immune-modulation such as decrease in IL-6, improvement in CD4+ve, CD19+ve, CD3+ve, and CD8+ ve cell count, increase in Lymphocyte to C-reactive protein ratio (LCR), Leukocyte to CRP ratio (LeCR) and a decrease in Neutrophil to Lymphocyte ratio (NLR) apart from improvement in EDSS [8], their gut microbiome after intervention has shown a significant correlation. Such correlation is very well falling in line with the reported indicators of severity of clinical findings, wherein specific gut microbiome associated with relapse of disease, have decreased after Neu-REFIX beta-glucan in the present study. This is one of its kind report in the literature yielding a dual advantage improving the good microbiome and suppressing the harmful ones, making us recommend Neu-REFIX beta-glucan a potential DMT requiring larger studies for validation not only in MS but also other auto-immune-inflammatory conditions.
Data Availability
All data generated or analysed during this study are included in the article itself.
Acknowledgements
The authors thank
The Government of Japan and the Prefectural Government of Yamanashi for a special loan and M/s Yamanashi Chuo Bank for processing the transactions.
Ms. Ann Gonsalvez and members of Multiple Sclerosis Society of India (MSSI)- Chennai Chapter for their coordination with the participants of the study.
Dr. Malcolm Jeyaraj, Neurologist for his clinical inputs and evaluation of the patients.
Prof. Dr. R. Raveendran, Dept. of Pharmacology, Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Pondicherry, India for providing his valuable inputs on the statistical analysis of the study.
Dr. Ragaroobine, Mr. Rajmohan from Nichi-In Centre for Regenerative Medicine (NCRM) for their assistance with data collection.
Mr. Masato Onaka, Mr. Yasushi Onaka of Sophy Inc, Kochi, Japan for technical advice.
Ms. Yoshiko Amikura and staff of GN Corporation Co Ltd, Japan for their liaison assistance with the conduct of the study.
Footnotes
Declarations:
Ethics approval and consent to participate
The study was registered in Clinical trials registry of India, CTRI/2022/05/042497 and approved by Universal Ethics Committee (A Unit of Aurous HealthCare Research and Development India Pvt. Ltd).
Consent for publication
Not applicable
Availability of data and material
All data generated or analysed during this study are included in the article itself.
Funding
No external funding was received for the study
Competing interests
Author Samuel Abraham is a shareholder in GN Corporation, Japan which holds shares of Sophy Inc., Japan., the manufacturers of novel beta glucans using different strains of Aureobasidium pullulans; a board member in both the companies and also an inventor to several patents of relevance to these beta glucans.
Authors’ contributions
NI and SA contributed to conception and design of the study. VD and CV helped in data collection. NY and RS helped with data analysis. SA and SP drafted the manuscript. KI and HK performed critical revision of the manuscript. All authors read and approved the final manuscript.



