
Abstract
While systemic corticosteroids quicken patient recovery during acute exacerbations of COPD, they also have many adverse effects. The optimal duration of corticosteroid administration remains uncertain. We performed a systematic review and meta-analysis to compare patient outcomes between short-(≤7 day) and long- (>7 day) corticosteroid regimens in adults with acute exacerbations of COPD.
MEDLINE, EMBASE, CENTRAL, and hand searches were used to identify eight eligible RCTs and three retrospective cohort studies. Risk of bias was assessed using the Cochrane RoB 2.0 tool and ROBINS-I. Data were summarized as odds ratios (ORs) or mean differences (MDs) whenever possible and qualitatively described otherwise.
A total of 11532 participants were included, with 1296 eligible for meta-analyses. Heterogeneity was present in the methodology and settings of the studies. The OR for mortality was 0.76 (95% CI=0.40–1.44, n=1055). The MD for hospital length-of-stay was -0.91 days (95% CI=-1.81–-0.02 days, n=421). The OR for re-exacerbations was 1.31 (95% CI=0.90–1.90, n=552). The OR for hyperglycemia was 0.90 (95% CI=0.60–1.33, n=423). The OR for infection incidence was 0.96 (95% CI=0.59–1.156, n=389). The MD for one-second forced expiratory volume change was -18.40 mL (95% CI=-111.80–75.01 mL, n=161).
The RCTs generally had low or unclear risks of bias, while the cohort studies had serious or moderate risks of bias. Our meta-analyses were affected by imprecision due to insufficient data. Some heterogeneity was present in the results, suggesting population, setting, and treatment details are potential prognostic factors. Our evidence suggests that short-duration treatments are not worse than long-duration treatments in moderate/severe exacerbations and may lead to considerably better outcomes in milder exacerbations. This supports the current GOLD guidelines for corticosteroid administration.
No funding was given for this review. Our protocol is registered in PROSPERO: CRD42023374410.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent decreases in a patient’s ability to breathe and perform gas exchange. It can present as chronic bronchitis— which involves inflammation of the airways—or emphysema—which involves tissue damage within the lungs. It is a leading cause of mortality and morbidity worldwide, causing 3.3 million deaths in 2019 primarily in lower-income countries [1]. Depending on the data source and definition, COPD was estimated to afflict from 212.3 to 384 million people worldwide in 2019, making it one of the most common illnesses in the world [1,2]. Symptoms can be relatively benign during earlier stages but can progress to hinder even simple everyday actions such as dressing oneself. COPD is generally irreversible, so treatment focuses on delaying the progression of the disease. The global societal burden of COPD was estimated to be 71.1 million disability-adjusted life years in 2019 [1]. From 2020–2050, the total global economic cost of COPD was estimated to reach $4.3 trillion USD (2017 prices) [3]. As the global population increases and ages, the burden of COPD is bound to increase.
COPD is usually diagnosed via spirometry by measuring an individual’s one-second forced expiratory volume (FEV1) and forced vital capacity (FVC). According to the GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines, an FEV1/FVC ratio of less than 0.7 is necessary for COPD diagnosis [4]. The severity of airflow limitation is also assessed via an individual’s % predicted FEV1, which is the proportion of an individual’s measured FEV1 compared to what would be expected from a healthy reference. Airflow severity is graded from GOLD 1 (mild) to GOLD 4 (very severe) [4].
While COPD is a chronic condition, many patients also suffer from acute exacerbations of symptoms which can last from days to weeks [5]. Respiratory infection is a major contributor to exacerbation, with others including environmental irritants such as pollutants and smoke from burning biomass [6]. While milder exacerbations can often be managed in an outpatient setting, severe exacerbations often require hospitalization. Severe exacerbations represent a major source of mortality for COPD patients, with a study by Hoogendoorn et al. reporting a 15.6% case-fatality rate [7]. Exacerbations account for about 40% of the treatment costs for COPD [8], with costs increasing with exacerbation severity [9]. Furthermore, frequent exacerbations are correlated with faster deterioration of lung function, though it is unclear if this is due to the exacerbations themselves or a third common factor [10].
For mild exacerbations, GOLD guidelines recommend treatment using only short-acting bronchodilators, whereas for moderate and severe exacerbations corticosteroid administration should also be considered [4]. Corticosteroids have anti-inflammatory properties, which are useful since COPD exacerbations are strongly associated with both local and systemic inflammation [11]. There is strong evidence that systemic corticosteroids improve patient outcomes during moderate and severe exacerbations [12,13]. However, there are many adverse effects associated with corticosteroid use, such as hyperglycemia, osteoporosis, muscle weakening, and infection due to immunosuppression [11]. These effects are directly correlated with the dosage and duration of corticosteroid administered [11]. Thus, they are not usually recommended as maintenance therapy for stable COPD and there is interest in minimizing the amount of corticosteroid given during exacerbations while still retaining their benefits [4].
There is no strong consensus on the duration or dosage of corticosteroids that should be given to a patient during exacerbations, with studies hampered by a seemingly large degree of patient-to-patient variation in their responses to corticosteroid treatment [11]. Although guidelines from GOLD and other organizations exist, poor adherence during exacerbations remains an issue and is related to worse outcomes for patients [14,15]. A systematic review and meta-analysis conducted by Walters et al. in 2018 found that short-duration systemic corticosteroid regimens (7 days or less) are not likely to lead to worse outcomes than long-duration regimens (more than 7 days) in adult patients with COPD exacerbations [16]. However, the authors also concluded that there were not enough data to form a definitive conclusion. In this study, we revisited the comparison with additional data from a large RCT and three retrospective cohort studies which were not included in the 2018 review. These data increased our confidence that short-duration regimens are not inferior in terms of mortality, re-exacerbation, infection, hyperglycemia, hospital length-of-stay (LOS), and FEV1 change. However, there was still not enough data for a conclusive verdict, and further studies would be beneficial.
Methods
This systematic review and meta-analysis was conducted in accordance with the PRISMA 2020 guidelines and the protocol registered in PROSPERO (ID: CRD42023374410) [17]. Our completed PRISMA 2020 checklist is available in S1 Figure.
Information sources and search strategy
To find studies, we systematically searched MEDLINE, EMBASE, and CENTRAL using Ovid. Medical Subject Heading terms were used to define the search strategy, which is available in S2 Figure. No language or date restrictions were imposed on the searches, which were conducted in September 2022. Additionally, references from similar previous systematic reviews were hand-searched in May 2023 to identify studies missed by the database search.
Selection process
After removing duplicates, studies were imported into Covidence—a web-based screening platform by Cochrane—where they were each subjected to a round of title/abstract screening followed by a round of full-text screening [18]. In each round, two reviewers independently assessed each study, and disagreements were resolved through discussion involving a third reviewer. Each study required unanimous approval from its reviewers to advance into the next stage.
Studies were included if they included adults (18 years or older) who were receiving corticosteroids as an acute-phase treatment for an exacerbation of COPD as defined by each individual study. Each study had to include a group who received a short-duration corticosteroid regimen (≤7 days) and a group who received a long-duration corticosteroid regimen (>7 days). All corticosteroid types and administration methods were included, as well as studies with co-interventions such as bronchodilators and antibiotics. Studies using corticosteroids for maintenance therapy (as opposed to treatment for exacerbations) and studies including asthmatic patients were excluded. While we originally intended to also examine the differences between low and high doses of corticosteroids in our protocol, there was too much heterogeneity among the studies during the preliminary screening. Thus, our review only examined the differences between short- and long-duration regimens.
Data extraction
Each study was randomly assigned to two reviewers who independently extracted data, with conflicts being resolved through discussion and arbitration by a third reviewer. The data extraction form was created a priori and included the outcomes mortality, length of hospital stay, number of re-exacerbations during follow-up, FEV1 change, respiratory infection, and hyperglycemia. All data points within the follow-up period were included. Additional collected information included bibliographic information, study type (RCT or cohort), details of corticosteroid regimen, study period, country, definition of exacerbation, inclusion/exclusion criteria, co-interventions, comorbidities, time until follow-up starts, follow-up duration, and demographic data.
Risk of bias assessment
Risk of bias assessment for each study was conducted independently and in duplicate by the same reviewers who performed the data extraction for that study. RCTs were assessed using the Cochrane RoB 2.0 tool which assessed five domains: bias due to the randomization process, deviations from intended interventions, missing outcome data, measurement of outcome, and selection of the reported result [19]. Cohort studies were assessed using the ROBINS-I tool which assessed seven domains: bias due to confounding, selection of patients into the study, classification of intervention, deviations from intended intervention, missing data, measurement of outcomes, and selection of reported results [20]. We tried to minimize the risk of publication bias by using a broad search strategy. We also intended to use funnel plots and statistical testing to assess the risk of publication bias but were unable to do so due to an insufficient number of studies.
Data analysis
Data from studies were compiled into meta-analyses and visualized where possible using the RevMan Web application (version 5.8.0) from Cochrane [21]. Mantel-Haenszel odds ratios (ORs) were used for the number of re-exacerbation, hyperglycemia, and infection events during follow-up, while Peto ORs were used for mortality due to the rarity of events. Mean differences (MDs) were used for hospital length-of-stay and FEV change. Point estimates were presented along with the 95% confidence interval (CI) and p-value for the combined data and RCT-only data for each outcome, along with cohort study-only data if it was significant. For each meta-analysis, heterogeneity was assessed using visual inspection of the forest plots as well as the I2 statistic. I2 values greater than 50% were considered significantly heterogeneous while values greater than 75% were considered seriously heterogeneous. Fixed effects models were used for analyses, with sensitivity analyses using random effects models being conducted when significant unexplainable heterogeneity was present.
We attempted to contact study authors to obtain missing data. If needed, missing standard deviations were estimated using methods described in the Cochrane Handbook for Systematic Reviews. Certainty of evidence was assessed using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) framework, with each outcome being graded as being of high, moderate, low, or very low certainty [22]. In accordance with guidelines, outcomes started off as “high” certainty, and the ratings were lowered by one level for a moderate degree (or two levels for a serious degree) of risk-of-bias, imprecision, inconsistency, indirectness, or publication bias. Two authors independently assessed each outcome, with any disagreements being resolved through discussion.
Results
Search Results
After removing duplicates, 4947 studies were identified from database and hand searches (Fig 1). Eight RCTs and three retrospective cohort studies were included in our review, with seven RCTs and two cohort studies being included in the meta-analyses. The characteristics of the studies are summarized in Table 1. Of the eight RCTs, four were only available as abstracts. We also referenced the 2018 Cochrane review by Walters et al. to fill gaps in our data [16]. There were four records in our search for which we could not find the article for, but their titles suggested none of them would have fit our inclusion criteria. Excluded studies which were similar to those we included are listed in S1 Table along with the reason for exclusion. The main results from the included studies are summarized in Table 2.

Risk of bias
The Cochrane Risk of Bias 2.0 tool was used to assess the RCTs in our study. Three of the RCTs available as full articles (Leuppi 2013, Sayiner 2001, and Chen 2008) were deemed to be at low risk of bias. The fourth full article, Zhou 2021, was an open-label trial and rated as having moderate risk of bias. However, we lowered its risk to “low” for mortality and re-exacerbations due to the objectivity of the outcomes; a lack of blinding would not likely have affected the outcome measurement. The four abstract-only studies did not have enough information to properly assess overall risk of bias (Table 3). One abstract, Sirichana 2008, was an open-label trial and therefore was rated as “moderate” for bias in the “deviation from intended domains” and “measurement of the outcome” domains.
The ROBINS-I tool was used to assess risk of bias for the cohort studies by comparing their designs to hypothetical, well-designed RCTs assessing the same question in the same setting (Table 4). All three studies had issues with confounding and selection as the choice of corticosteroid regimen duration could have been affected by the severity of the patient’s exacerbation. This was mitigated in Sivapalan 2019 as they specifically used data which spanned a guideline change for corticosteroid regimen duration in Denmark. This meant the choice between a shorter- and longer-duration regimen was more likely to be due to the specific guideline in effect at that time than the severity of exacerbation [31]. The studies were also rated as “moderate” for “risk of bias from selection of the reported result” as they did not report a separate protocol or statistical analysis plan. Alshehri 2021 was rated as “unknown” for “bias in deviations from the intended interventions” as it did not report data for some co-interventions and co-morbidities.
Results of syntheses
Mortality
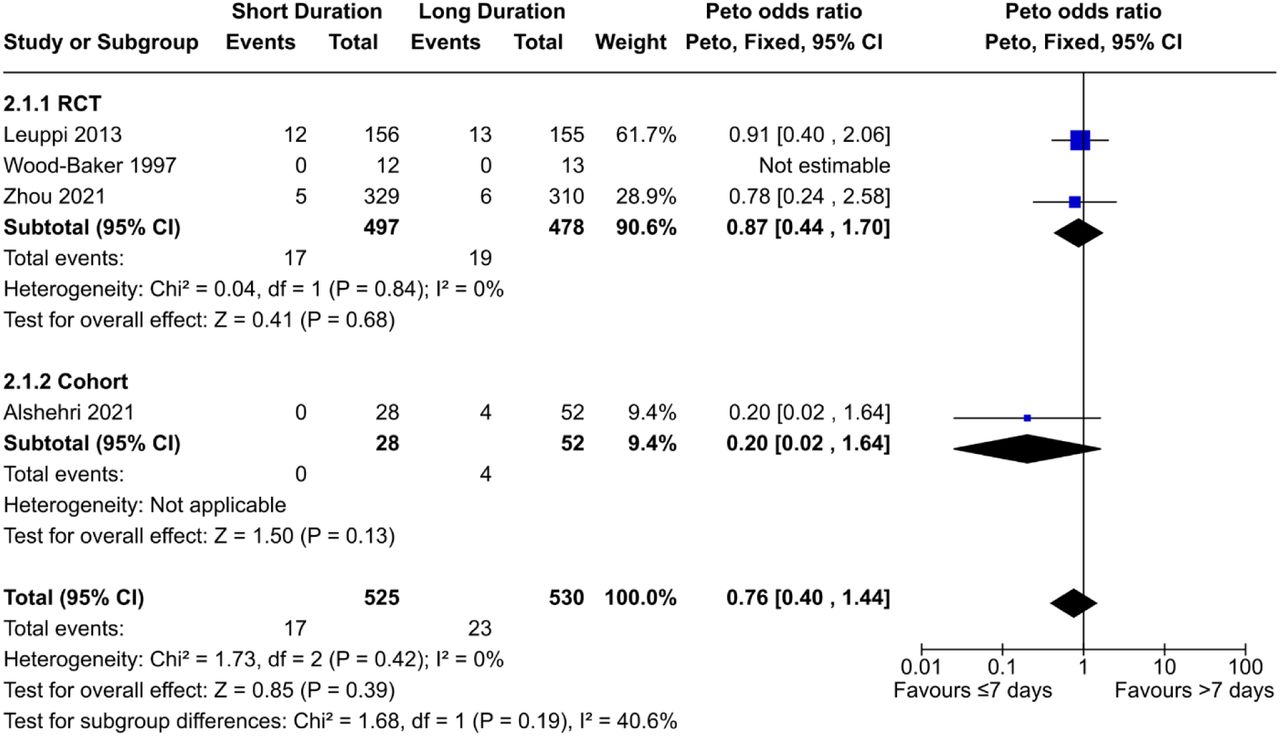
Three RCTs and one cohort study contributed a total of 1055 participants to the meta-analysis for mortality (Fig 2). One RCT (Wood-Baker 1997) reported zero deaths and was unable to produce an OR. The combined OR between the long- and short-duration groups was 0.76 (95% CI = 0.40–1.44, p=0.39), while the OR with only RCT data was 0.87 (95% CI = 0.44–1.70, p=0.68).

In contrast, another cohort study by Sivapalan et al. found that corticosteroid regimens over 10 days resulted in higher mortality compared to those less than 10 days, with an adjusted hazard ratio of 1.8 (95% CI = 1.5–2.2) one year after treatment. Notably, this study was conducted using a Danish outpatient registry, whereas the other studies were conducted on inpatients with comparatively more severe exacerbations.
Both Leuppi 2013 and Zhou 2021 were judged to be at low risk of bias for this outcome. Alshehri 2021 had serious risk of bias, while Sivapalan 2019 had moderate risk of bias. The certainty of evidence from the RCT data was downgraded to “moderate” due to imprecision, while the certainty from cohort study data was downgraded to “very low” due to imprecision and risk of bias. Altogether, our data shows there is likely no difference in mortality between short-(≤7 days) and long- (>7 days) duration regimens, though mortality may be lower in short-duration regimens specifically in outpatients with less-severe exacerbations.
Hospital length-of-stay
Three RCTs contributed a total of 421 participants to the meta-analysis for hospital length-of-stay (Fig 3). One of the RCTs (Leuppi 2013) did not report SDs, instead only reporting medians, IQR, and means. We used the reported means and estimated the SDs by dividing the IQRs by 1.35. However, this method relies on the assumption that the data is normally distributed, so we performed a sensitivity analysis by excluding the study. With Leuppi 2013 included, the mean difference is marginally significant at -0.91 days (95% CI = -1.81–-0.02 days, p=0.05). However, excluding the study causes the difference to become non-significant at -0.07 days (95% CI = - 1.47–1.33 days, p=0.93). Alternative methods of interpretation yield different results; a similar analysis conducted in a previous review by Walters et al. used the medians instead of the means and produced a non-significant result of -0.61 days (95% CI = -1.51–0.28 days, p=0.18) [16]. Notably, the significance of the difference in length of stay was reported as p=0.04 in Leuppi 2013 via the log-rank test, which is likely closer to the null than the data in our meta-analysis [27]. The true degree of significance is unknown, but we believe it is unlikely to be strongly significant.

Two cohort studies were unable to be included in the meta-analysis as they did not report the required statistics. Alshehri 2021 found no significant difference (p=0.88) between long-duration and short-duration regimens, while Poon 2017 found shorter stays in the short regimen group (p<0.05).
Chen 2008 and Leuppi 2013 had low risk of bias, while Wood-Baker 1997 had unknown risk. Alshehri 2021 and Poon 2020 had serious risk of bias. The evidence from the RCTs was downgraded to “moderate” due to imprecision, while the evidence from the cohort studies were downgraded to “very low” due to risk of bias and imprecision. Altogether, our data shows that hospital LOS is likely to be either the same between short- (≤7 days) and long- (>7 days) duration regimens or slightly shorter in short-term regimens.
Number of re-exacerbations
Four RCTs and one cohort study contributed a total of 552 participants towards the meta-analysis for the number of re-exacerbations during follow-up (Fig 4). The odds ratio for all the data was 1.31 (95% CI = 0.90–1.90, p=0.16), while the ratio for RCT data only was 1.04 (95% CI = 0.70–1.56, p=0.84). The odds ratio for the cohort study was significant at 5.21 (95% CI = 1.93–14.08, p=0.001). There was considerable heterogeneity in the data (I2=56%) due to the cohort study. Bias notwithstanding, it is possible this difference is due to the different study population; the RCTs were conducted in Europe and east Asia, while Alshehri 2021 used data from Saudi Arabia. Alshehri et al. noted the low compliance rate for COPD maintenance therapy in the Middle East, with low compliance being linked to higher exacerbation rates [24]. However, the impact resulting from this difference in populations is unclear. Another difference is follow-up duration, with Alshehri 2021 and Sirchana 2008 using a 30-day follow-up while Leuppi 2013 and Sayiner 2001 both using 180 day follow-ups (the follow-up duration for Chen 2008 was unknown). However, data for Leuppi 2013 was non-significant at 30 days via log-rank test (p=0.87). Sensitivity analysis excluding Alshehri 2021 and Sirichana 2008 does not produce a significant result (OR 1.01, 95% CI = 0.66–1.55, p=0.95), and neither does changing to a random-effects model (OR 1.62, 95% CI = 0.79–3.32, p=0.18).

Additionally, Zhou 2021 reported frequency exacerbations as a rate, which was not significant between the two groups (p>0.05) after 1, 3, 6, 9, and 12 months.
Three RCTs (Chen 2008, Leuppi 2013, and Zhou 2021) were deemed to be at low risk of bias, while one (Sirichana 2008) had unknown risk of bias but was unblinded. Zhou 2021 was deemed to be at low risk despite being open-label due to the objectivity of the outcome. Alshehri 2021 had a serious risk of bias. The certainty of evidence was downgraded to “moderate” due to imprecision, while the certainty for the cohort data was downgraded to “very low” due to risk of bias and imprecision. Altogether, our data shows the number of re-exacerbations during follow-up is likely to be either the same between short- (≤7 days) and long- (>7 days) duration regimens or slightly higher in short-duration regimens.
Hyperglycemia
Two RCTs and one cohort study contributed a total of 423 participants to the meta-analysis for hyperglycemia (Fig 5). The OR for the combined data was 0.96 (95% CI = 0.59–1.55, p=0.58), while the OR for the RCTs only was 0.99 (95% CI = 0.64–1.53, p=0.96). Both RCTs were deemed to be at low risk of bias, while the cohort study had significant bias.

Additionally, one abstract (Sirichana 2008) noted that fasting plasma glucose was not different after 14 days, though that is only a proxy for hyperglycemia. Also, the study was unblinded and not enough information was available to assess overall risk of bias.
The certainty of evidence from the RCTs was downgraded to “moderate” due to imprecision, and the certainty from the cohort study was downgraded to “very low” due to risk of bias and imprecision. Overall, our data shows there is likely no difference in hyperglycemia incidents between short- (≤7 days) and long- (>7 days) duration regimens.
Infection Incidence
One RCT and one cohort study contributed 389 patients to the meta-analysis for infection incidence (Fig 6). The OR for the combined data was 0.96 (95% CI = 0.59–1.56, p=0.87), while the OR for the RCT only was 0.99 (95% CI = 0.61–1.62, p=0.97).

However, another cohort study (Sivapalan 2019) reported an adjusted hazard ratio of 1.2 (95% CI=1.0–1.3, p=0.011) after 1 year, with more incidents in the long-duration group. However, this data only included pneumonia events and only included outpatients, who had comparatively less severe exacerbations.
Leuppi 2013, Sivapalan 2019, and Poon 2017 had low, moderate, and serious risk of bias, respectively. The certainty of evidence from Leuppi 2013 was rated as “moderate” due to imprecision, while the evidence from the cohort studies was rated as “very low” due to risk of bias, imprecision, and indirectness in the case of Sivapalan 2019. Our data shows there is likely to be no difference in infection risk between short- (≤7 days) and long- (>7 days) duration regimens, but there may be less incidents in short-duration regimens specifically in outpatients with less-severe exacerbations.
FEV1 change
Three RCTs contributed 161 patients to the meta-analysis of FEV1 change (Fig 7), which used the post-treatment FEV1 (measured on the last day of the long-treatment regimen) as a proxy for the increase in FEV1. This choice was made to increase the number of studies that could be included in the analysis, and because the baseline pretreatment FEV1 between the two groups in each study were not significant. The mean difference was -18.40 mL (95% CI = -111.80– 75.01 mL, p=0.70), but there was considerable heterogeneity in the studies (I2=71%).

Compared to the other two studies, data from Sayiner 2001 had a mean difference that heavily favoured long duration regimens. This may be due to the relatively short duration of treatment of 3 days for the experimental arm, while the short duration arm for Chen 2008 and Sirichana 2008 were 7 and 5 days, respectively. If this is the case, this heterogeneity may represent a form of dose-dependent relationship between corticosteroid regimen duration and FEV1 change. The effect of corticosteroids on FEV1 recovery seems to be most apparent in the initial 3–5 days of treatment. In that case, the short-duration group of Sayiner 2001 would have ended at the beginning of this period. Neither excluding the study nor switching to a random-effects model produced a statistically significant result (MD 54.50 mL, 95% CI = -53.87–162.88 mL, p=0.32, and MD -49.90 mL, 95% CI = -251.05–151.26 mL, p=0.63, respectively). Excluding Sirichana 2008 with or without excluding Sayiner 2001 also did not produce a significant result (MD 60 mL, 95% CI = -56.24–176.24 mL, p=0.66 and MD -22.32 mL, 95% CI = -120.62–75.99 mL, p=0.31, respectively).
Leuppi 2013 found no difference in FEV1 at discharge, nor at 0, 6, 30, or 180 days (p=0.94). Gomaa 2008 also reported no significant difference in FEV1 change after 7, 14, and 30 days. Al Mamun 2011 found no significant difference at days 7 and 14 (p=0.100, p=0.079, respectively). Zhou 2021 only provided data in terms of % of predicted FEV1. Neither the % predicted baseline FEV1 nor % predicted FEV1 after 180 days were significant across the two groups (p=0.174 and p=0.134 respectively), with the mean being slightly higher in the long duration arm in both time points.
Leuppi 2013, Chen 2008, and Sayiner 2001 had low risk of bias. Sirichana 2008 and Zhou 2021 were both open-label, with the former having unknown overall risk of bias and the latter having moderate risk of bias for this outcome. Gomaa 2008 and Al Mamun 2011 had an unknown risk of bias. The certainty of evidence for this outcome was downgraded to “low” due to imprecision in the effect estimate and inconsistency from unexplained heterogeneity. Our data shows there may be no difference in FEV1 change between short- (≤7 days) and long- (>7 days) duration regimens.
Discussion
To our knowledge, this review addresses the question of optimal corticosteroid regimen duration in COPD exacerbations using the largest dataset to date. The impetus of this study was the conclusion of the 2018 Cochrane review by Walters et al., which concluded that although 7- and 14-day regimens did not seem result in significantly different outcomes, there was a relative paucity of evidence that necessitated further research [16]. In our review, we included additional data from a large recently published RCT (Zhou 2021), three retrospective cohort studies, and qualitative data which could not be included in the meta-analyses. Overall, we believe this new data reinforces the conclusion that short-duration regimens are not worse than long-duration regimens in terms of mortality, re-exacerbation, hyperglycemia, hospital LOS, and FEV1 change. Notably, Sivapalan 2019 was a relatively large and rigorous cohort study which specifically examined outpatient data unlike the other studies which primarily focused on hospitalized patients. It reported clinically relevant decreases in mortality and pneumonia incidents in the short-duration regimen. While it is only a single study examining two outcomes, it validates previous concerns regarding the non-generalizability of research from severe exacerbations to those with milder exacerbations [16]. This is also consistent with the GOLD guidelines, which do not recommend the use of corticosteroids in treating mild exacerbations [4]. The European Respiratory Society and American Thoracic Society tentatively suggest consideration of 14 days or fewer of oral corticosteroid use in ambulatory patients with exacerbations [34]; the findings of Sivapalan 2019 suggest that duration should be decreased even further.
Limitations of our study
Although we were able to include more studies compared to past reviews, our analyses still suffered from a relative lack of data. Of the 11 studies we included in our review, only 4 of them were full-article RCTs, and only 2 of those RCTs had more than 100 participants. This issue manifested as wider CIs in the summary estimates, which resulted in us downgrading the certainty of every outcome due to imprecision since we felt that the clinical decisions would be different at either end of the CI. Additionally, we were hesitant to give much weight to the cohort studies during our interpretation of the results due to their small size and inherent risk of bias [35]. The low number of studies also meant we were unable to perform subgroup analysis, so the effects of prognostic factors such as blood eosinophil count were unable to be assessed [36]. There was heterogeneity in the specifics of the corticosteroid regimens used in each study in terms of corticosteroid type, administration methods, treatment duration/dosage, and the presence of a taper. For example, while Wood-Baker 1997 compared 3- and 14-day regimens, the cumulative dosages were much more similar at 7.5 mg/kg and 6.3 mg/kg respectively [32]. There was also heterogeneity in the settings of each study. For example, Alshehri 2021 was conducted in Saudi Arabia and reported significantly more re-exacerbations in the short-duration group, contrary to other studies [24]. The authors cited differences in treatment adherence as a possible explanation; another study found that patients in Saudi Arabia had lower adherence to COPD maintenance treatment compared to those in Turkey—where Sayiner 2001 was conducted [37]. Poor adherence to guidelines during exacerbations remains an issue and is related to worse outcomes for patients [14,15]. This reiterates the concern that data from our included studies may not be generalizable to all populations. Relatedly, our sole study that specifically assessed outpatients raises questions about the generalizability of our results in outpatients, which represent over 80% of all exacerbations [4]. RECUT—a currently ongoing RCT which specifically recruits outpatients—will hopefully shed more light on this issue [38].
While we adhered to the PRISMA guidelines and other best practices whenever possible, some limitations exist in the methods we used. We were unable to statistically or graphically check for publication bias due to an inadequate number of studies. Such tests generally require at least 10 studies to be sufficiently powered [39], while the most studies we had in an outcome was five. None of the full articles reported conflicts of interests arising from funding or other sources (abstracts were unable to be assessed) or were designed/reported in an obviously intentionally biased way. We do not believe considerable publication bias was present, but we cannot be certain. Another limitation is that we did not report on all outcomes that were relevant to the topic. We decided on our outcomes a priori to minimize our ability to perform selective reporting. Some outcomes we did not address were mean time to re-exacerbation, treatment failure, quality of life, other spirometric parameters such as FVC, and other adverse effects. A past review by Walters et al. did not find any significant difference in any of those outcomes [16], although notably, Zhou 2021 found a significant decrease in the mean time to next exacerbation in the short-duration cohort [33].
Implications for the future
The certainties of evidence for each outcome were all either “moderate” or “low” for RCT data, and “very low” for cohort study data. While short-duration regimens are unlikely to be worse than long-duration regimens in general, we cannot fully preclude the possibility of inferiority for all individual outcomes, especially re-exacerbation rate. Additional research is needed, with data on hospital LOS, re-exacerbation, and FEV1 change being the most likely to change the summary estimate in a clinically relevant way. Additionally, preliminary data suggests short-duration regimens may be considerably preferable to long-duration regimens for patients with milder exacerbations, but further data from RCTs are needed to confirm this. Overall, our findings support the recommendations of GOLD that systemic corticosteroids are given for 5–7 days for moderate to severe COPD exacerbations [4].
Acknowledgements
We would like to thank Winston Hou for providing guidance throughout this study.
Funding and conflicts of interest
The author(s) received no specific funding for this work. The authors have declared that no competing interests exist.
Data availability statement
All relevant data are within the manuscript and its Supporting Information files.
Supporting information




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgements
We would like to thank Winston Hou for providing guidance throughout this study.
References



