
ABSTRACT
Importance The influence of total daily and light intensity activity on cancer risk remains unclear, as most existing knowledge is drawn from studies relying on self-reported leisure-time activities of moderate-vigorous intensity.
Objective To investigate associations between total daily activity, including step counts, and activity intensity on incident cancer risk.
Design, Setting, and Participants Prospective analysis of cancer-free UK Biobank participants who wore accelerometers for 7-days (between 2013-2015), followed for cancer incidence through national registries (mean follow-up 5.8 years (SD=1.3)).
Exposures Time-series machine learning models derived daily total activity (average acceleration), behaviour time, step counts, and peak 30-minute cadence from wrist-based accelerometer data.
Main Outcomes and Measures A composite cancer outcome of 13 cancers previously associated with low physical activity (bladder, breast, colon, endometrial, oesophageal adenocarcinoma, gastric cardia, head and neck, kidney, liver, lung, myeloid leukaemia, myeloma, and rectum) based on previous studies of self-reported activity. Cox proportional hazards regression models estimated hazard ratios (HR) and 95% confidence intervals (CI), adjusted for age, sex, ethnicity, smoking, alcohol, education, Townsend Deprivation Index, and reproductive factors. Associations of reducing sedentary time in favour of increased light and moderate-vigorous activity were examined using compositional data analyses.
Results Among 86 556 participants (mean age 62.0 years (SD=7.9) at accelerometer assessment), 2 669 cancers occurred. Higher total physical activity was associated with a lower overall cancer risk (HR1SD=0.85, [95%CI 0.81-0.89]). On average, reallocating one hour/day from sedentary behaviour to moderate-vigorous physical activity was associated with a lower risk (HR=0.92, [0.89-0.95]), as was reallocating one hour/day to light-intensity physical activity (HR=0.94, [0.92-0.96]). Compared to individuals taking 5 000 daily steps, those who took 9 000 steps had an 18% lower risk of physical-activity-related cancer (HR=0.82, [0.74-0.90]). We found no significant association with peak 30-minute cadence after adjusting for total steps.
Conclusion and Relevance Higher total daily physical activity and less sedentary time, in favour of both light and moderate-vigorous intensity activity, were associated with a lower risk of certain cancers. For less active adults, increasing step counts by 4 000 daily steps may be a practical public health intervention for lowering the risk of some cancers.
Question What insights can we gain about the relationships between total daily activity, step counts, and activity intensity on cancer risk using accelerometer data?
Findings In an analysis of 86 556 individuals from the UK Biobank who provided a week of accelerometer-based activity data, higher levels of total physical activity, reducing sedentary time in favour of light or moderate-vigorous intensity activities, and higher daily step counts were associated with a lower risk of certain cancers.
Meaning For less active adults, increasing activity time and accumulating more daily steps may be practical interventions for lowering the risk of some cancers.
INTRODUCTION
Epidemiological data indicate that over half of all new cancers in high-income countries could be avoided by modifying lifestyle factors, including addressing physical inactivity.1,2 However, quantifying the dose-dependent benefits of specific physical activity (PA) behaviours for cancer prevention remains challenging. Many existing studies rely on self-report questionnaires, which emphasize time spent in leisure-time activities of a moderate-vigorous intensity and may have recall errors and reporting biases.3,4 Time use data studies suggest that most individuals spend a significant amount of time devoted to work and household activities, with the majority of physically active time obtained from light-intensity physical activity (LIPA).5–7 Global adherence to PA recommendations, which primarily emphasize moderate-vigorous physical activity (MVPA), is generally poor.8 Consequently, there is a growing interest in understanding whether more accurate measures of MVPA show protective effects for cancer risk and if interventions to increase LIPA could be a valuable disease prevention strategy.
Wearable accelerometer devices provide objective measures of all daily activities, including sedentary and physically active time accumulated at home, work, during transportation, and in leisure-time.9 Accelerometer data can also be used to investigate how reallocating time from sedentary behaviour to either LIPA or MVPA could influence disease risk. Existing accelerometer-measured activity studies in cancer have primarily focused on cancer mortality and,10–14 to a limited extent, breast cancer risk.15,16
To address these gaps and challenges, we aimed to understand the relationship between total daily activity and intensity, step counts, and incident cancer risk using a composite outcome of 13 cancer sites previously associated with low PA in studies of self-reported leisure time activity.17 As a secondary analysis, we assessed the risks for all 13 PA-related cancers individually and, as case numbers allowed, for other site-specific cancers. We also conducted compositional data analyses to explore the impact of reallocating time from sedentary behaviour to LIPA and MVPA. Finally, for potential translation to the clinical and public health settings, we examined the dose-response relationship between step count, stepping intensity, and incident cancer. Step counts are an easily understandable metric among the general population and are reported by many consumer wearable devices and fitness trackers.18
METHODS
Study population
The UK Biobank is a prospective study that enrolled 502 536 adults in England, Scotland, and Wales between 2006-2010.19,20 At baseline, participants completed a questionnaire, provided biological data, and consented for linkage to electronic medical records. From June 2013 to December 2015, participants with valid emails were invited to wear an Axivity AX3 wrist-worn accelerometer for 7 days.7
Accelerometer data processing
Accelerometer data were processed using methods described by Doherty (“accelerometer”, v7.1.0).21 Total physical activity (PA) was calculated as the mean vector magnitude per epoch to derive an overall mean per day acceleration in milligravity (mg) units. This metric reflects the activity duration and intensity and has been validated against doubly labelled water.21
Proportions of time spent across sleep, sedentary behaviour (SB), light-intensity physical activity (LIPA), and moderate-vigorous physical activity (MVPA) per day, were calculated using random forest and hidden Markov model machine-learning methods.7 Missing time due to non-wear was imputed by averaging the behaviour in the corresponding times across all valid days.7
Step counts were calculated using a hybrid self-supervised learning model trained on ground truth free-living stepping data (“stepcount”, v3.1.1).22 Daily step count was reported as the median number of daily steps during the seven-day measurement period. Peak 30-minute cadence was calculated as the mean of the 30 highest daily cadence values, averaged across all days.23 Further processing details are described in eTable 1.
Outcome ascertainment
The main outcome was a composite cancer outcome of 13 sites previously found to be associated with low PA (bladder, breast, colon, endometrial, oesophageal adenocarcinoma, gastric cardia, head and neck, kidney, liver, lung, myeloid leukaemia, myeloma, and rectal).17 Cancers were obtained by the UK Biobank through the National Health Service (NHS) Digital for participants from England and Wales and the NHS Central Register for participants from Scotland (details in eTable 2).24 In secondary analyses, we assessed the risks for cancers not previously related to PA with at least 100 cases (eTable 3).
Analytic sample
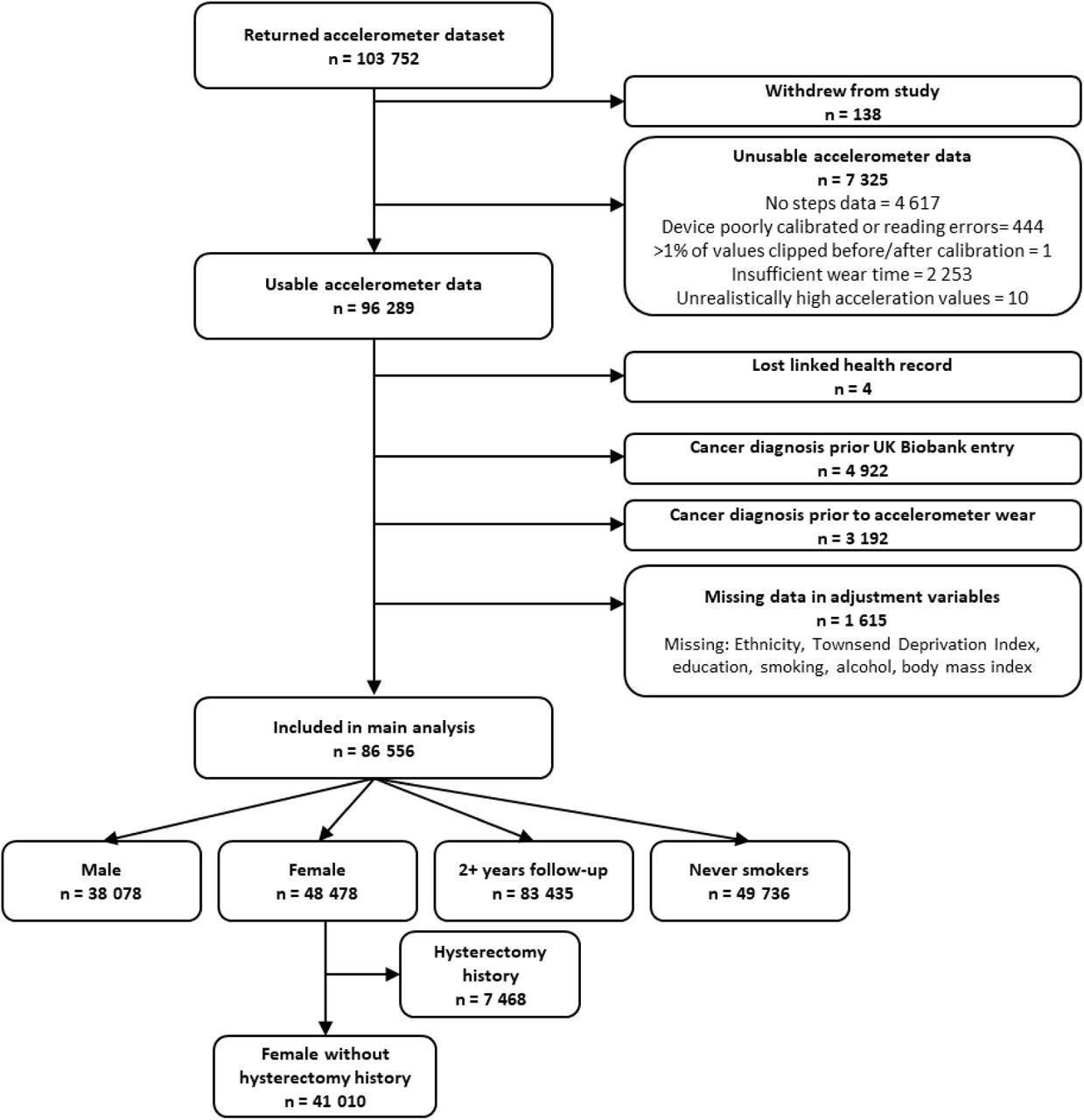
Raw accelerometer data from 103 614 participants were processed, excluding study withdrawals. We further excluded participants with device calibration or data reading errors (>1% of values outside +/-8g range), inadequate wear time (<72 hours), unreasonably high average acceleration (>100 mg), and lacking steps data.{Citation} Individuals with cancer (excluding C44: non-melanoma skin cancer) before accelerometer wear and missing healthcare linkages or covariate data, were also excluded. The final analysis included 86 556 participants (eFigure 1).

Statistical analysis
Cox proportional hazards regression models estimated adjusted Hazard ratios (HRs) with 95% confidence intervals for a one standard deviation (SD) increase in total activity and incident cancer. We also assessed risks across quintiles of physical activity.
Attained age was the underlying time scale. Individuals who were cancer-free during follow-up were censored at their date of death or at the end of the follow-up period (31 December 2020, England; 31 December 2016, Wales; 30 November 2021 Scotland).
Multivariable models adjusted for sex (male, female), ethnicity (White, non-White), smoking status (never, previous, current unknown cigarettes/day, current <15 cigarettes/day, current ≥15 cigarettes/day), alcohol consumption (never, <3 times per week, ≥3 times per week), education (school leaver, further education, higher education), and deprivation based on the Townsend Deprivation Index (TDI) (quintiles ranging from least deprived to most deprived, based on the 2011 UK census).25 Female-specific models were further adjusted for oral contraception ever use (no, yes, missing), hormone replacement therapy ever use (no, yes, missing), menopausal status (no, yes, missing/unknown), and parity (0, 1-2, 3+, missing). Covariate data were provided by participants at the UK Biobank baseline assessment and were chosen a priori based on existing studies (Details in eTable 1). No violations of the proportional hazards assumption were observed for the exposures using Schoenfeld residuals.
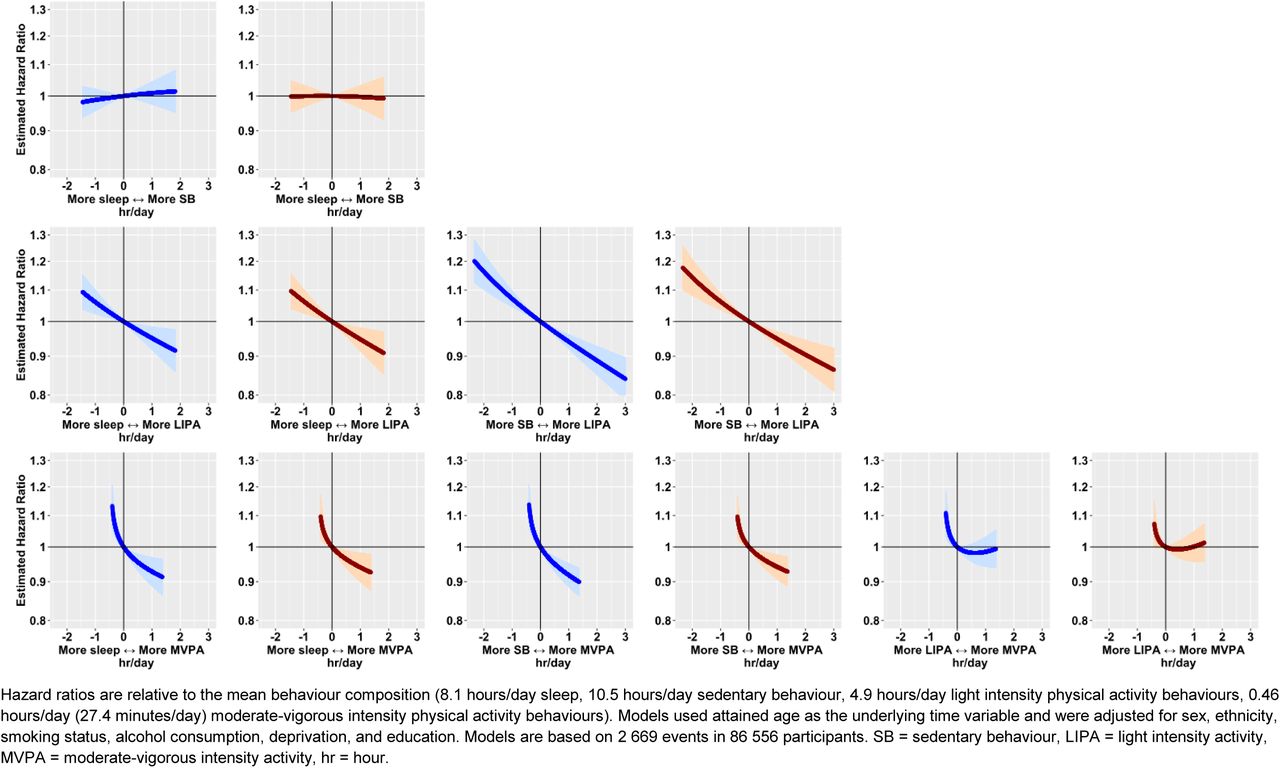
Compositional data analyses, using the "epicoda" package, modelled associations between the relative time spent in SB, LIPA, MVPA, and sleep and cancer risk.7 First, we calculated the estimated HR associated with reallocating time to one behaviour from all other proportionally (e.g., reallocating one hour/day to LIPA from all other behaviours proportionally). 7 Second, we estimated HRs for specific pairwise reallocations of time between behaviours (e.g., reallocating one hour/day from SB to LIPA, holding sleep and MVPA constant). For all compositional analyses, the estimated hazard ratios were relative to the mean behaviour composition among included participants for a hypothetical average participant.
Finally, we used restricted cubic splines to assess the relationship between step count and cancer incidence using a reference point at the 10th percentile and knots positioned at the 5th, 50th, and 90th percentiles. We employed P-values for linear trends to estimate significance of the overall association. Multivariable models were further adjusted for daily step count.
We conducted several sensitivity analyses, including adjustment for body mass index (<25, 25-30, and 30+ kilograms/meters²) as measured at the assessment centre and dietary factors (fresh fruits and vegetable consumption (<3, 3–4.9, 5–7.9, or 8+ servings/day, missing); red and processed meat consumption (<1, 1–2.9, 3–4.9, or 5+ times/week, missing)). Two subgroup analyses were conducted, one among males and females, and the other among never smokers. To assess the potential influence of reverse causality, we repeated the analyses after excluding the first two years of follow-up. Statistical analyses were performed May-November 2023 using R (v4.2.2; R Foundation for Statistical Computing). Two-sided P values of <0.05 was considered statistically significant.
Consent
Participants in the UK Biobank provided written informed consent. The study was approved by the National Information Governance Board for Health and Social Care and the National Health Service North West Multicentre Research Ethics Committee (06/MRE08/65). We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines (eTable 4).26
RESULTS
Among 86 556 participants, the mean age at accelerometer assessment was 62.0 years (SD=7.9). The majority were female (56%), identified as White (97%), and fell within the least deprived quintile of the Townsend Deprivation Index (50%) (Table 1). Throughout a mean follow-up of 5.8 years (SD=1.3; 504 557 person-years), 2 669 physical activity (PA)-related cancers accrued, with breast among females (n=995) being the most common (details in eTable 3).
Total daily PA and cancer incidence
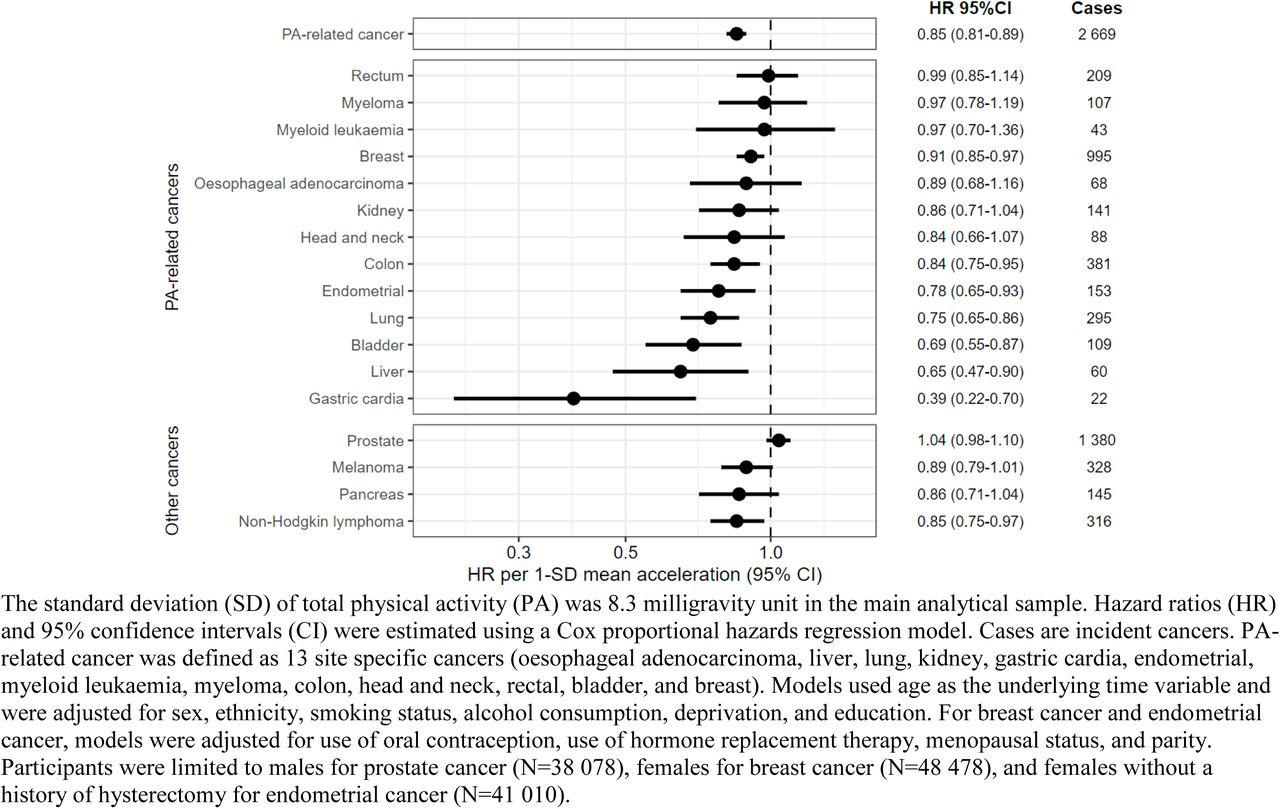
Higher total PA was associated with a lower risk of PA-related cancer (hazard ratio (HR) per 1 SD (8.3 milligravity (mg) units), 0.85 [95% confidence interval (CI) 0.81-0.89]) in the multivariable-adjusted models (Figure 1; eTable 5). Similar associations were found in models assessing quintiles of total PA (eTable 6).
To explore which cancers contributed to this result, we also examined associations for individual cancer sites (Figure 1; eTable 5). With higher daily PA, we observed a significantly lower risk for seven types; gastric cardia (HR1SD=0.39, [95% CI 0.22-0.70]), liver (HR1SD=0.65, [0.47-0.90]), bladder (HR1SD=0.69, [0.55-0.87]), lung (HR1SD=0.75, [0.65-0.86]), endometrial (HR1SD=0.78, [0.65-0.93]), colon (HR1SD=0.84, [0.75-0.95]), and breast cancers (HR1SD=0.91, [0.85-0.97]). There were also suggestive associations (HR < 0.9) for three cancers; oesophageal adenocarcinoma (HR1SD=0.89, [0.68-1.16]), kidney (HR1SD=0.86, [0.71-1.04]), and head and neck cancers (HR1SD=0.84, [0.66-1.07]). Similar associations were found in models assessing quintiles of total PA (eTable 6).
In secondary analysis of non-PA-related cancer sites, we observed no protective association with prostate cancer, an inverse association with non-Hodgkin lymphoma (HR1SD=0.85, [0.75-0.97]), and suggestive inverse associations for melanoma (HR1SD=0.89, [0.79-1.01]) and pancreatic cancers (HR1SD=0.86 [0.71-1.04]).
Compositional data analysis
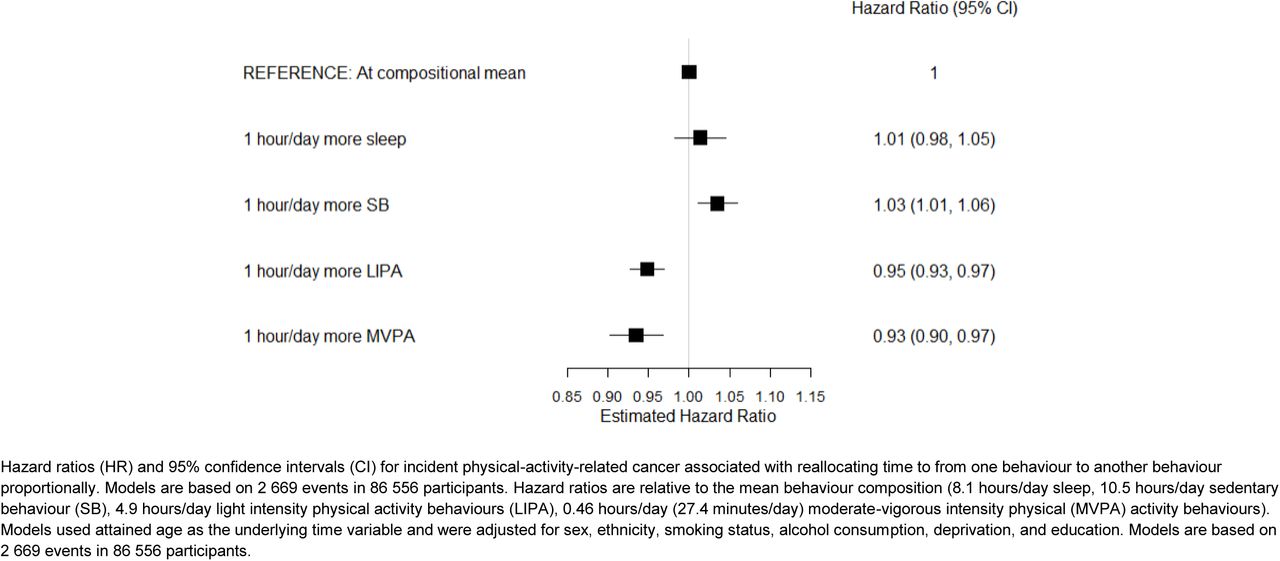
First, we estimated the risks associated with each behaviour individually by reallocating time to one behaviour from all others proportionally for an average individual (eFigure 2). Reallocating one hour/day to LIPA from all other behaviours was associated with a 5% lower risk of PA-related cancer (HR=0.95, [0.93-0.97]) in multivariable-adjusted models. Reallocating one hour/day to MVPA from other behaviours was associated with a 6% lower cancer risk (HR=0.93, [0.90-0.97]). Reallocating one hour/day to sedentary behaviour (SB) was associated with a significantly higher cancer risk (HR=1.03, [1.01-1.06]), but reallocating one hour/day to sleep was not (HR=1.01, [0.98-1.05]).

Next, we estimated the risks associated with specific pairwise reallocations of time between behaviours (Figure 2; eTable 7). For an average participant, reallocating one hour/day from SB to overall physical activity (LIPA + MVPA) was associated with a 7% lower risk (HR=0.93, [0.91-0.95]) in the multivariable-adjusted model. Reallocating one hour/day from SB to MVPA alone was associated with an 8% lower cancer risk (HR=0.92, [0.89-0.95]), and reallocating one hour/day from SB to LIPA was associated with a 6% lower risk (HR=0.94, [0.92-0.96]).
Step counts and cancer incidence
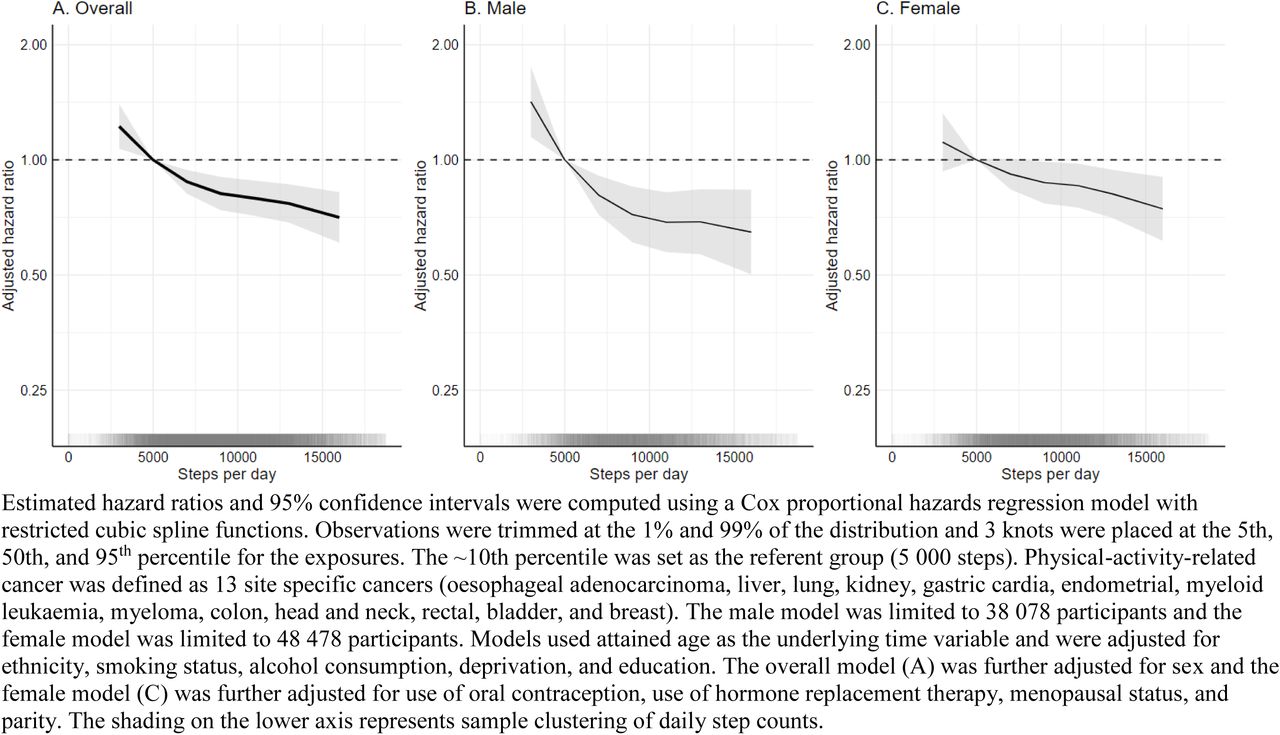
Higher daily step counts were associated with a lower risk of PA-related cancers (P for trend≤0.001) after multivariable adjustments (eTable 8; Figure 3). Compared to individuals who took 5 000 daily steps (10th percentile, reference), individuals who took 9 000 daily steps had an 18% lower risk (HR=0.82, [0.74-0.90]), while those who took 13 000 steps had a 23% lower risk (HR=0.77, [0.69-0.86]). Individuals taking fewer than 5 000 steps had a higher risk.

Higher step intensity (peak 30-minute cadence) was associated with a lower risk of PA-related cancer prior to adjustment for total step counts (Table 2). Compared to individuals who took 70 steps/minute (10th percentile, reference), individuals who took 120 steps/minute had a lower cancer risk before (HR=0.72, [0.59-0.89]), but not after adjusting for total daily steps (HR=0.88, [0.69-1.14], P for trend=0.05).
Sensitivity analyses
Associations for total PA and cancer risk were slightly attenuated after adjusting for body mass index (BMI) in models per 1-SD of total activity (eTable 5), but the direction between the quintiles was consistent (eTable 6). BMI adjustment did not substantially alter results from the compositional analyses (eFigure 3; eTable 7) or the spline models for step count (eTable 8), nor did adjusting for dietary factors (eTables 5-8, eFigure 4).
Sex-specific models of 1-SD differences in total PA showed that patterns of association for cancer risk were similar among males and females for most cancer sites (eTables 9-10), as were findings from the compositional data analysis (eFigure 5). Protective associations were observed for step count and PA-related cancer risk in sex-specific models (eTable 11; Figure 3). Analyses conducted among never smokers were similar to our primary analysis (eTable 12; eFigure 6). After removing the first two years of follow-up, higher activity quintiles demonstrated protective associations for cancer risk, but the impact was more attenuated in lower activity categories (eTable 13; eFigure 7).
DISCUSSION
In this prospective analysis, higher total daily physical activity (PA) measured by accelerometers was associated with a composite of 13 cancers previously shown to be associated with PA in studies of self-reported leisure time activity.17 We also observed lower risks for 7 of these 13 cancers. Additionally, we found protective associations for minimizing sedentary time in favour of engaging in light intensity physical activity (LIPA) or moderate-vigorous physical activity (MVPA). Compared with individuals who took 5 000 steps per day, those who took 9 000 daily steps had an 18% lower risk of incident PA-related cancer. A weaker suggestive association with higher step intensity was observed, but results were not significant after adjusting for total step count.
Results from our compositional data analysis are novel and suggest that less sedentary time in favour of LIPA or MVPA was associated with a lower risk of certain cancers. These findings align with previous studies indicating that sedentary behaviour may be associated with chronic disease risk factors and cancer development and progression.27–29 Notably, our finding that any intensity of PA was beneficial contrasts with findings from cardiovascular disease research, where intensity plays a more pivotal role in determining health benefits.7,27 A study by Stamatakis found that short bursts of vigorous intensity PA were associated with a lower risk of PA-related cancer among non-exercising adults.30 Our findings suggests that efforts to decrease sedentary behaviour in favour of engaging in LIPA or MVPA activities, such as allocating more time to casual walking, household chores, home repairs, and gardening could also support cancer prevention efforts and might be feasible to incorporate into everyday routines. Further, our study was not limited to non-exercisers, which enhances the applicability of our findings.
Walking, a highly accessible and popular form of PA, is often considered an ideal exercise intervention due to its simplicity to track and minimal adverse effects.31 Our findings show that higher steps counts were associated with a lower risk for PA-related cancers. In terms of step intensity, we found a weaker but non-significant association after adjusting for total step count. These findings align with our compositional model results for total PA, which suggested that LIPA and MVPA were beneficial for cancer risk. Together, this suggests that walking at any pace may provide health benefits with respect to cancer incidence.
Our study adds new information to a limited literature base on the association between total daily PA and incident cancers.11 Previous research in the UK Biobank cohort reported protective associations for self-reported PA and cancer, and we extend these findings for many site-specific cancers.28,32 Our findings align with other studies using accelerometer data that found physical activity may play a role in the prevention of PA-related cancers among older women33 and for incident breast cancer.15,16 In addition to finding lower risk for 7 of the 13 PA-related cancers identified by Moore and colleagues,17 we also observed a protective association between total PA and non-Hodgkin lymphoma and suggestive associations for melanoma and pancreatic cancers. This suggests potential areas for future research, especially in samples with larger case counts.
Several hypothesized mechanisms linking higher PA with a lower cancer risk have been proposed. These mechanisms encompass hormonal changes, insulin levels, inflammation, immune function, and oxidative stress.29 Some hypotheses suggest that PA may reduce cancer risk by influencing body weight, but we observed no substantial changes in model estimates after adjusting for body mass index, although measurements here were obtained several years before the accelerometer measurements, potentially introducing imprecise estimates over time.
Strengths and limitations
Our study has several strengths, including the use of accelerometer devices in a large and prospective cohort study, which reduces susceptibility to recall and reporting biases compared to most previous studies.3,4 Accelerometers captured a wide range of daily behaviours, including both sedentary and physically active activities, as well as step count. Further, we processed the accelerometer data using open-source methods.34 Our sample included a wide age-range (43-78 years at accelerometer wear) of participants, making the cohort mature for analysing more common adult-onset cancers.19,35 Our results add to the limited literature on how physical activity impacts cancer risk across different cancer sites. We also employed compositional data analyses to model associations for 24-hour behaviours, rather than just individual behaviour risks. In addition, we controlled for key cancer risk factors and conducted extensive sensitivity analysis to examine major threats to the validity of our findings.
This study also had several limitations. The UK Biobank cohort includes middle to early late-aged individuals, potentially leading to underrepresentation of cancers with onset at more advanced ages. Secondly, the study is observational, and we cannot exclude the possibility of unmeasured and residual confounding. Reverse causation is also a possibility, as certain cancers may have been undiagnosed at the time of accelerometer wear and could have reduced daily PA. Nonetheless after removing the first two years of follow-up, we observed only minor attenuations. Future UK Biobank studies with additional follow-up will be required to investigate associations for less common cancers. Furthermore, we had accelerometer data from one period during middle-age; thus, we are also unable to draw conclusions about PA earlier in the life in relation to cancer risk. Finally, the study population drawn from the UK Biobank may not be representative of wider populations.36 However, we believe that the etiological findings are still likely to have broader applicability.37
Conclusion
Results from this prospective study suggest protective associations between engaging in higher levels of overall daily PA, reducing sedentary time in favour of engaging LIPA or MVPA, and increasing daily step counts and cancer risk. These findings underscore the potential health benefits of incorporating lower intensity activities into daily life during middle age, alongside promoting higher intensity activities in public health initiatives focused on cancer prevention.
Data Availability
We do have permission to share the data. However, all bona fide researchers can apply to use the UK Biobank resource for health-related research that is in the public interest (https://www.ukbiobank.ac.uk/register-apply/).
Author Contributions
Shreves had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Shreves, Travis, Matthews, Doherty.
Acquisition, analysis, or interpretation of data: Shreves, Small, Walmsley, Saint-Maurice, Papier, Travis, Matthews, Doherty.
Drafting of the manuscript: Shreves, Travis, Matthews, Doherty.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Shreves.
Obtained funding: Shreves, Travis, Matthews, Doherty.
Administrative, technical, or material support: Shreves, Chan, Walmsley, Doherty.
Supervision: Doherty, Matthews, Travis.
Conflict of Interest Disclosures
Shreves, Moore, Gaitskell, Travis, and Matthews declare no competing interests.
Doherty is supported by Novo Nordisk. Doherty accepted consulting fees from the University of Wisconsin (NIH R01 grant) and Harvard University (NIH R01 grant). Doherty received support for presentations at the International Conference on Soft Computing in Data Science 2021, Korean Society of Cardiology 2020, and Oxford International Study Abroad programme 2023. Doherty received support to attend the 2023 CTSU Joint Annual Collaborators’ Meeting, London, 2023 Big Model AI for Drug Design workshop, Abu Dhabi, 2023 Festival of Genomics, London, 2022 Industry Symposium on Digital Biomarkers, EMBL-EBI, Cambridge, 2020 ELIXIR Bioinformatics Industry Forum, London, 2020 3rd NYU Biomedical and Biosystems Conference, Abu Dhabi, 2020 Academy of Medical Sciences, UK-Japan Symposium on Data-Driven Health. Doherty is a member of the 2021 Scientific advisory board EU IMI IDEA-FAST. Doherty received a donation from SwissRe to purchase equipment for accelerometer data collection in the China Kadoorie Biobank.
Doherty, Walmsley, and Chan have released accelerometer analysis software under an academic use license that could result in commercial entities paying license fees for their use.
Funding/Support
Shreves, Saint-Maurice, Moore, and Matthews are supported by the National Institutes of Health’s Intramural Research Program. Shreves is also supported by the National Institutes of Health’s Oxford Cambridge Scholars Program. Walmsley is supported by HDR UK, an initiative funded by UK Research and Innovation, Department of Health and Social Care (England) and the devolved administrations. Papier is supported by Cancer Research UK (grant number C16077/A29186). Chan is supported Novo Nordisk. Doherty and Small are supported by the Wellcome Trust (223100/Z/21/Z). Doherty is also supported by Novo Nordisk, Swiss Re, and the British Heart Foundation Centre of Research Excellence (grant number RE/18/3/34214). Travis is supported by Cancer Research UK (grant number C8221/A29017).
Role of the Funder/Sponsor
The funders/sponsors had no role in the design of this study, the analysis and interpretation of the results, or drafting of the manuscript.
eTABLES
eFIGURES







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ACKNOWLEDGEMENTS
REFERENCES



