
ABSTRACT
Background The association between preoperative wearable device step counts and surgical outcomes has not been examined using commercial devices linked to electronic health records (EHR). This study measured the association between daily preoperative step counts and postoperative complications.
Study Design Data was obtained using the All of Us (AOU) Research program, a nationwide initiative to collect EHR and health-related data from the population. Included were patients who underwent a surgical procedure included in the National Surgical Quality Improvement Program (NSQIP) targeted procedures dataset. Excluded were patients who did not have available physical activity FitBit data. Primary outcome was the development of a postoperative complication. All analyses were performed in the AOU researcher workbench.
Results Of 27,150 patients who underwent a surgical procedure, 475 participants with preoperative wearable data were included. 74.7% were female and 85.2% were White. The average age was 57.2 years. The overall rate of postoperative complications was 12.6%. Patients averaging fewer than 7,500 daily steps were at increased odds for developing a postoperative complication (OR 1.83, 95% CI [1.01, 3.31]). Following adjustment for age, sex, race, comorbid disease, body mass index (BMI), and relative procedure risk, patients with a baseline average steps/day < 7,500 were at increased odds for postoperative complication (aOR = 2.06, 95% CI [1.05, 4.06]).
Conclusions This study found an increase in overall postoperative complication rate in patients recording lower average preoperative step counts. Patients with a baseline of less than 7,500 steps per day had increased odds of postoperative complications in this cohort. This data supports the use of wearable devices for surgical risk stratification and suggests step count may measure preoperative fitness.
INTRODUCTION
Risk stratification is a critical part of successful perioperative care and guides efforts for optimization when preparing a patient for surgery.1, 2 In recent years, preoperative fitness assessment has gained increasing recognition as a tool for surgical risk stratification. Cardio-pulmonary exercise testing (CPET) can be used to test patient fitness and plan postoperative care based on individual risk.3 Some have also worked to implement subjective, self-reported measures to more easily estimate functional capacity prior to surgery.4
Beyond planning postoperative care, recent data demonstrates a benefit for prehabilitation, which focuses on improving patient fitness prior to surgery by targeting modifiable lifestyle factors such as diet, exercise, smoking, and mental health.5 Interventional studies targeting physical activity in the preoperative period have demonstrated the ability to improve functional capacity and postoperative outcomes.6–8 Tracking patient fitness and physical activity in the preoperative period may facilitate the identification of modifiable targets to improve surgical outcomes.
Despite these advances, challenges remain in the clinical implementation of these approaches. Traditional methods of functional capacity assessment have depended on CPET or subjective/self-reported measures. While CPET offers a robust measure of fitness and can inform perioperative care, it requires an investment of substantial resources.9 It is unclear how accurately subjective assessment portrays patient fitness.10, 11 Wearable devices, such as Fitbits, provide a wealth of objective physical activity data and could offer a convenient, cost-effective, and accessible way to inform clinicians about patients’ overall fitness over an extended period. Recently, several studies have examined the association of preoperative step counts recorded by wearable pedometer devices with postoperative outcomes.12–15 However, prior work has typically been confined to small prospective cohorts undergoing a single type of procedure. In addition, no study utilizing a large-scale EHR dataset has measured the association between step counts and postoperative outcomes across procedures of varying organ sites and complexity.
The All of Us (AOU) Research Program is a National Institutes of Health (NIH)-funded effort to collect EHR, health questionnaire, genetic, and digital health technology data from over 1 million people in the United States.16 Participants have the opportunity to share wearable device data, providing physical activity data that can be linked to their EHR data. The primary aim of this study was to investigate the association between preoperative daily step counts and postoperative adverse outcomes in AOU participants who have undergone elective surgical procedures.
METHODS
Study Participants
This was a retrospective cohort study using the All of Us Research Program Controlled Tier version 7 data set and included participants who contributed wearable device physical activity data along with EHR data. Participants 18 and older can be enrolled in the AOU Research Program after an informed consent process at an AOU-associated clinic. The AOU Research Program was approved by the AOU Institutional Review Board, and additional IRB approval is not required for studies using AOU data through the Researcher Workbench, a secure cloud-based platform. Deidentified data was accessed and analyzed within the AOU Researcher Workbench by authors who had completed AOU Responsible Conduct of Research training. Included were patients who underwent an elective surgical procedure defined using linked participant EHR data and source provided Current Procedural Terminology (CPT) codes. The selection of CPT codes for study inclusion was based on the same criteria used by the National Surgery Quality Improvement (NSQIP) program’s Procedure Targeted dataset (Supplementary Table 1). NSQIP data is not available in AOU. For patients who underwent multiple procedures, only the most recent was included for analysis. Participants with no available physical activity data prior to surgery were excluded.
Independent Variables
Age, sex, and race were obtained from AOU participant surveys. The most recent body mass index (BMI) measurement before the procedure was obtained from participant EHR. For participants without a BMI measurement (missingness 37.6%), the median was imputed. A sensitivity analysis was performed without BMI, BMI included without imputation, and median imputation, and no difference was noted based on approach. The BMI data showed a non-normal distribution, making the median a more robust measure than the mean. Additionally, the missing data were missing at random, supporting the use of a simple imputation method. Procedure risk was determined using the median length of stay (LOS) by CPT code. Procedures with median LOS of 0-1 days were deemed low-risk, 2-4 days medium-risk, and 5+ days high-risk. Comorbid disease was defined using ICD codes in participant EHR prior to surgery, indicating any condition defined under the Elixhauser comorbidity index. Physical activity was measured by calculating the mean daily steps for participants who had any preoperative physical activity data. Fitbit devices are not provided to AOU participants. Instead, participants who already own Fitbits can share their data with AOU. Fitbits have been utilized in many studies aimed at tracking patient activity, and prior studies have shown they provide reliable step counts.17, 18 While there is likely some inherent error in device recording, these devices have been proven to be effective and reliable for research purposes, particularly in their measurement of steps. The mean steps/day was chosen for analysis as this is what is typically provided by digital health applications to consumers, thus making results more applicable to users.
Development of Postoperative Complications
The primary outcome of the study was the development of any adverse event within 90 days of surgery. Adverse events included pneumonia, respiratory failure, pulmonary embolism, sepsis, cardiac arrhythmia, renal failure, urinary tract infection, and deep vein thrombosis. Systemized Nomenclature of Medicine (SNOMED) concepts were used for defining postoperative adverse events (Supplementary Table 2). This composite outcome was selected based on prior studies using similar large, EHR-based datasets to investigate surgical outcomes.19 Mortality was not included as a primary outcome as there were no deaths that occurred during the postoperative period in this cohort.
Statistical Analysis
Descriptive statistics summarizing participant demographic and other clinically relevant variables were represented by median and IQR for continuous variables and frequency for categorical variables. Two-sample t-tests and chi-squared tests were performed for normally distributed continuous and categorical variables, respectively, to compare demographic and clinically relevant data between participants in stratified groups. Adjusted analyses were conducted with multivariable logistic regression. All analyses were conducted in the AOU Researcher Workbench using Jupyter Notebook software version 6.4.8. The following packages were used for analysis: pandas, os, statsmodels, numpy, matplotlib, scipy, seaborn, and datetime. Participant counts of less than 20 are not reported to comply with the AOU Data and Statistics Dissemination Policy.
RESULTS
Descriptive Statistics
475 patients met our inclusion criteria. Demographic and clinical information about the cohort is provided in Table 1. Of the included participants, 60 (12.6%) experienced an adverse event within 90 days following their procedure. Patients who experienced an adverse event were more likely to be male (43.3% vs. 19.8%; P < 0.001), have 4+ comorbid conditions (76.7% vs. 11.6%; P < 0.001), and underwent a medium-or high-risk procedure (41.7% vs. 21.9%; P < 0.001).
Exploratory analysis to determine step threshold
Several step thresholds (average steps/day) were tested to determine observed differences in the rate of postoperative events. At increments of 500 steps, patients were stratified into two groups: active and inactive. For each threshold, the adverse event rate was calculated for those above (i.e. active) and below (i.e. inactive) the average daily step count (Figure 1). Further, univariable logistic regression models were performed to examine the relationship between step counts and odds of postoperative complication (Figure 2). Based on this, a preoperative activity level of 7,500 steps/day was used for further analyses. This point was chosen as it displayed a strong association with the primary outcome and because prior studies have shown step counts of 7000-8000 steps/day to be indicative of moderate to vigorous physical activity and are associated with reduced mortality. Additionally, dividing the cohort at 7500 steps achieved a balanced sample size between the two groups, and thus represents a realistic and pragmatic activity goal that could set for patients in a real clinical setting.20, 21 Baseline characteristics of participants in the active vs. inactive group are shown in Supplementary Table 3.

Average complication rate (any adverse event) above and below daily step count threshold, in 500 step increments.

Association between average daily steps (< y-axis) and development of a postoperative complication based on unadjusted logistic regression model. Based on these findings, a threshold of 7500 steps was utilized for further analyses.
Preoperative step count and 90-day postoperative adverse outcomes
On unadjusted analysis, the rate of 90-day postoperative adverse events was greater in patients who had recorded fewer than 7,500 daily steps prior to their procedure than those who averaged 7,500 or more steps a day (OR 1.83 [1.01, 3.31]). Given the relatively low event rate, there was insufficient evidence to conclude that individual complications were associated with the 7,500-step threshold. For example, amongst those in the inactive group, the odds of deep vein thrombosis were 2.03 [0.21, 19.65], surgical site infection 1.69 [0.33, 8.82], respiratory failure 2.03 [0.21, 19.65], urinary tract infection 1.88 [0.59, 6.01], cardiac arrhythmia 1.45 [0.66, 3.14], renal failure 1.12 [0.27, 4.76], sepsis 0.67 [0.09, 4.80], pulmonary embolism 2.03 [0.21, 19.65], and pneumonia 0.22 [0.02, 2.14] compared to the active group (Supplementary Figure 1).
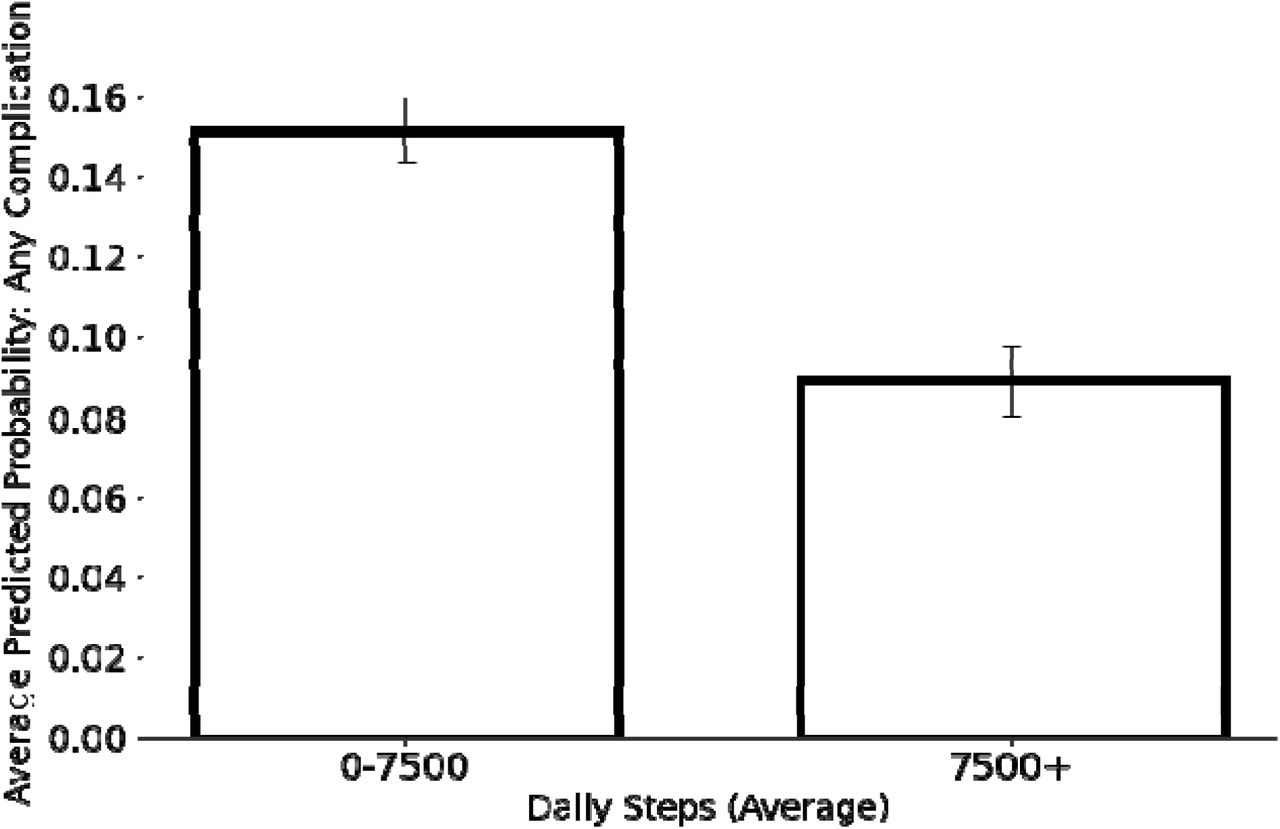
Following adjustment for age, sex, race, comorbid disease, body mass index (BMI), and relative procedure risk, patients with less than 7,500 average daily preoperative steps had increased odds of 90-day postoperative complications (aOR 2.06 [1.05, 4.06]; Figure 3). A final fitted model was used to calculate individual-level probability of developing a postoperative complication. A higher average probability of postoperative complications was observed for those taking <7,500 steps/day (15.1% vs. 8.9%; P < 0.001; Figure 4).

Association between average daily steps (<7,500) and development of adverse postoperative outcome based on multivariable logistic regression adjusting for clinical and demographic characteristics. Model diagnostics were performed with a C-index of 0.78, AIC of 320, and BIC of 362. BMI: body mass index.

Predicted probability of any adverse event based on estimates from fitted logistic regression model (including procedural risk, age, sex, race, comorbid disease) in participants above and below 7,500-step threshold. Error bars denote standard error.
DISCUSSION
In this retrospective observational cohort study of participants in the AOU Research Program, we found that preoperative daily step counts taken from EHR-linked wearable device data were an independent predictor for the development of adverse postoperative outcomes across a range of surgical procedures. After adjusting for patient demographic, clinical, and surgical factors, individuals who had an average daily step count of less than 7,500 steps prior to their procedure were at increased odds of developing adverse outcomes in the 90 days after surgery.
The results in this study are consistent with past studies that have examined postoperative outcomes in patients taking more or less than a set number of steps in the preoperative period.13, 14 The work reported here expands the scope of preoperative fitness assessment using wearable devices by utilizing a large and diverse surgical cohort, including several procedures of varying risk. The potential for using wearable devices to improve clinical care is supported by several prior studies in addition to ours. For example, after several surgical procedures, a higher step count on postoperative day one was associated with a decreased probability of a prolonged length of stay.22 In peritoneal cancer, a higher mean daily step count during the inpatient period predicted a lower risk of hospital readmission following resection.23 Others have shown that activity monitoring in the postoperative setting can help increase patient activity levels and ultimately improve outcomes.24, 25 In each of these studies, the use of wearable devices provided data to guide treatment that otherwise would not have been available through other monitoring tools.
Wearable devices can provide a more objective measure of preoperative fitness than patient-reported activity levels and a more cost-effective, efficient option than CPET. Wearable devices have previously been tested in the immediate preoperative period to provide similar information to CPET tests, such as 6-minute walking time.26 To translate wearable devices into clinical practice, a more rigorous selection of important features, their relative weights in determining surgical outcomes, and their interactions with other important clinical covariates should be further studied. For example, Cos et al. developed machine learning models that incorporated multiple domains of wearable device data to predict surgical outcomes in a cohort of pancreatectomy patients.27 Najafi et al. found a strong association between scores on a wrist-worn frailty-meter and major adverse events following lower extremity revascularization.28 Activity measured by wearable devices has also been shown to be associated with a shorter length of stay following major surgery.22
The growing body of work surrounding wearable devices has highlighted several areas in which they can improve care by replacing, adding to, and refining current measures of risk stratification. Additionally, several recent studies have shown patient fitness can be improved in the preoperative period through prehabilitation programs.29, 30 These programs can even be delivered through digital and virtual tools, such as smartwatches and mobile applications, making them accessible and easier to use for many patients.31 This suggests that wearable devices can not only be used for preoperative risk stratification, but also can be a mechanism to help improve postoperative outcomes.
Notable to this study was the use of the AOU Research Program to assess the association between preoperative step counts and surgical outcomes. The AOU Research Program presents a unique data source for conducting observational surgical research. Relative to other programs that have collected longitudinal health data, AOU has prioritized the recruitment of groups traditionally underrepresented in biomedical research to better reflect the diversity of the United States and make findings more generalizable to the population.16 Additionally, the AOU Research Program integrates data sources not typically available in other large datasets intended for biomedical research, such as wearable device, genetic, and participant-reported surveys.
In the context of the AOU Research Program and the integration of new technologies like wearable devices in healthcare, the importance of health equity cannot be overstated.32 Our findings underscore the necessity of making these technological advancements accessible and beneficial to the entire population, especially groups traditionally underrepresented in biomedical research. Future research should focus on understanding participants’ technological literacy, a crucial element for effectively using and interpreting wearable device data.33 Ensuring patients’ comfort and proficiency with these technologies is essential for enhancing their engagement and utilization. Additionally, preparing health providers to integrate this technology into their clinical practice, including the incorporation of wearable device data into EHR, is crucial. Exploring other implementation challenges and facilitators, such as addressing data privacy and managing cost considerations is also critical.34 Assessing the feasibility of implementing wearable technology in various healthcare settings will be key in identifying gaps and opportunities for ensuring equitable access and use of these technologies across diverse healthcare environments.35
The findings of this study must be considered in the context of the limitations. First, the step counts used as a preoperative measure did not reflect the immediate timeframe before surgery. Instead, all wearable device data that was generated by a patient prior to their surgery was factored into the average preoperative step count. As a result, the reported step count reflects chronic activity level and specific conclusions about how acute changes in step count leading up to surgery cannot be commented on based on the data available. Second, while AOU has focused on recruiting historically underrepresented groups in biomedical research, the included participants all had wearable device data from a personal Fitbit, and the study cohort may not be representative of a broader population. Third, there was heterogeneity among surgical procedures included in the study that included surgeries which may have treated conditions that could directly impact daily step counts (i.e., orthopedic procedures). However, the approach to include longer-term step count data allows an assessment of chronic activity that is less sensitive to the condition-specific changes that occurred closer to the time of surgery. For example, the average number of days of step data included was 851 (Q1: 240; Q3: 1343) per patient. Lastly, while AOU has sought to enroll a diverse group of participants, with many participants belonging to groups traditionally underrepresented in biomedical research, it relies on a bring-your-own-device (BYOD) model for collecting Fitbit data. BYOD programs have traditionally suffered from a lack of diversity, and this is evidenced by the study cohort being comprised of largely white, female, non-Hispanic or Latino participants.(31)
In conclusion, average daily steps are associated with elective surgical outcomes across a range of common procedures and the relationship is independent of several clinically relevant factors including comorbid conditions and type of surgery. The results of this study support the use of wearable device data and a step threshold of 7,500 steps as a guide to preoperative risk stratification and optimization programs prior to elective surgery.
Data Availability
All data produced in the present work are contained in the manuscript.
SUPPLEMENTARY DATA

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Unadjusted analysis was performed on all postoperative adverse events and each individual event between active and inactive groups (odds ratios showing inactive relative to active). Any codes indicating chronic conditions were excluded.
ACKNOWLEDGEMENTS
The All of Us Research Program is supported by the National Institutes of Health, Office of the Director: Regional Medical Centers: 1 OT2 OD026549; 1 OT2 OD026554; 1 OT2 OD026557; 1 OT2 OD026556; 1 OT2 OD026550; 1 OT2 OD 026552; 1 OT2 OD026553; 1 OT2 OD026548; 1 OT2 OD026551; 1 OT2 OD026555; IAA #: AOD 16037; Federally Qualified Health Centers: HHSN 263201600085U; Data and Research Center: 5 U2C OD023196; Biobank: 1 U24 OD023121; The Participant Center: U24 OD023176; Participant Technology Systems Center: 1 U24 OD023163; Communications and Engagement: 3 OT2 OD023205; 3 OT2 OD023206; and Community Partners: 1 OT2 OD025277; 3 OT2 OD025315; 1 OT2 OD025337; 1 OT2 OD025276. In addition, the All of Us Research Program would not be possible without the partnership of its participants.
Footnotes
Meeting Presentation: American College of Surgeons (ACS) Clinical Congress, Boston, MA, October 2023
Title update; Figure 2 added to clarify selection of step threshold
REFERENCES



