
Abstract
Background Little is known about which outcome domains characterise meaningful recovery following prosthetic rehabilitation and should be measured. Our previous qualitative work developed a conceptual model of outcome domains which are meaningful to patients. This qualitative synthesis aims to develop that model by exploring views and experiences of recovery captured in the limb loss literature, and use these to produce a second iteration of the model describing outcome domains of importance following prosthetic rehabilitation from the patient’s perspective.
Methods Systematic searches were conducted using CINAHL, Psychinfo and Web of Science from 2011 to early 2023. Studies with a qualitative design focusing on views and experiences of lower limb prosthetic users were eligible for inclusion. Quality was assessed using the CASP tool. ‘Best Fit’ framework synthesis was used to synthesise the evidence and develop the conceptual model.
Results 40 studies were included, describing the experiences of 539 participants. Data supported the pre-existing conceptual model and led to development of four of the five domains. The newly named ECLIPSE model describes meaningful outcome domains as 1) Being able to participate in important activities and roles, 2) Participating in the way I want to, 3) My prosthesis works for me, 4) If I am in pain, I can manage it, and 5) I am able to accept my new normal. Studies came from 15 countries showing good coverage of high-income settings. Few participants from low-and-middle-income countries were included, it is unclear if the ECLIPSE model describes outcome domains of importance in these settings.
Conclusions This synthesis provides a rigorous foundation for understanding outcome domains of importance following lower limb prosthetic rehabilitation from the patient’s perspective. The ECLIPSE model is an accessible representation of recovery which could direct rehabilitation programmes, as well as inform the evaluation of prosthetic care through the selection of outcome measures.
Background
Outcome measurement is increasingly important in clinical practice, assisting clinicians to understand the impact of their interventions and the effectiveness of the services they provide [1]. The term outcome measurement can be better understood by breaking it down into i) the outcome domain being measured and ii) the measurement tool. An outcome domain can be defined as an element of health (i.e. pain, physical function, emotional wellbeing) that is changed by a particular intervention [2]. A measurement tool can be defined as a standardised instrument used in research and clinical practice to capture and evaluate change [3].
Despite its potential value, outcome measurement is still not routinely used in clinical practice [4]. Within prosthetic rehabilitation several clinical interest groups, such as the British Association of Physiotherapists in Limb Absence Rehabilitation (BACPAR) and the International Society of Prosthetics and Orthotics (ISPO), have attempted to increase health care professional engagement by publishing recommended outcome measures for use in clinical settings [5–8]. However, numerous outcome measures are included in the recommendations, with different measures proposed by different professional groups. The recommendations also include many outcome measures capturing the same outcome domain (i.e., mobility via measures such as the Six Minute Walk test, Timed Up and Go, or the Amputee Mobility Predictor). A recent narrative review highlighted the absence of outcome measure consensus in the field of prosthetic rehabilitation, and suggested it may be driven by a lack of understanding around which outcome domains characterise a meaningful recovery following prosthetic rehabilitation, and should therefore be measured [9].
Gaining consensus regarding outcome domains of importance is crucial to allow effective comparison of research findings and clinical data. Consensus is advocated for by organisations such as Core Outcome Measurement in Effectiveness Trials (COMET) [10], and the International Consortium of Health Outcome Measurement (ICHOM) [11], who recommend domain consensus in research and clinical settings, respectively. Both groups promote a multistakeholder approach, including patients, to ensure domains are relevant to those for whom health and rehabilitation interventions have the most impact. However, a recent review of patient participation in core outcome set development questioned how patient-centred the process is [12]. The review found health care professionals tended to dominate prioritisation exercises, and few studies employed qualitative methods that may give patients more opportunity to contribute in a meaningful way [12].
Within prosthetic rehabilitation several authors have begun to explore which outcome domains are important to people who use a prosthetic limb, using qualitative approaches. McDonald et al. and Shaffalitsky et al. [13,14] both explored outcome domains of importance following the prescription of a prosthesis, focusing on the impact of componentry rather than the wider, holistic impacts of prosthetic rehabilitation recommended by professional groups [5,15]. These authors identified domains of importance such as balance, independence and adjustment, and interestingly highlighted differences in what patients and clinicians thought was most important [14]. Another small body of work attempted to develop an International Classification of Functioning (ICF) core set which could be used to inform which outcome domains to measure [16–19]. However, the authors identified several important concepts which could not be matched to the ICF and were therefore not included, such as socket comfort and feelings of acceptance following amputation. Moreover, the deductive approach recommended for ICF core set development may have diminished the voice of the patient.
This current study follows on from our large UK qualitative study [20], which began to address the knowledge gap regarding outcome domains of importance following prosthetic rehabilitation. The study included a heterogenous sample of 37 lower limb prosthetic users and identified five key outcome domains of importance from the patient’s perspective, which were presented as a conceptual model to inform both outcome measure selection and rehabilitation priorities (Figure 1). The study included a wide range of views and experiences, but was limited by only involving individuals from the UK. Both convenience and purposive sampling were used to generate a diverse study population, however participants were identified by clinicians which may have led to a bias towards patients who had a positive experience of rehabilitation, or a more successful outcome.

Due to the limitations of a single qualitative study, further research is required to understand outcome domains of importance following prosthetic rehabilitation and continue developing the conceptual model considering the views and experiences of a larger population in different settings. Therefore, the aim of this article is twofold. Firstly, the study aims to use a systematic approach to search and synthesise published qualitative research, to explore outcome domains of importance following rehabilitation from the prosthetic user’s perspective, as captured in the current evidence base. Second, the study extends the authors’ empirical qualitative research described above [20] that underpinned the first stage of the conceptual model development, to generate a second iteration of the model informed by the wider experiences described in the limb loss literature.
Materials and methods Research design
A systematic review of the literature and ‘Best fit’ framework synthesis were undertaken to address the research aims. A comprehensive systematic approach was adopted to identify relevant publications, ensuring findings are based on a foundation of rigor and resonate with the prosthetic community which has been described as having a culture of quantitative enquiry [21]. ‘Best fit’ framework synthesis was used to analyse data and further develop the authors conceptual model of meaningful outcome domains in light of experiences described in the qualitative evidence base.
This approach was underpinned by a critical realist world view which looks to access the knowable world [22], in this case the perceptions of important outcome domains following lower limb amputation through the lens of prosthetic users. The conduct and reporting of this review adhere to the ENTREQ guidelines (Enhancing transparency in reporting the synthesis of qualitative research) [23].
Search strategy
As recommended for aggregative approaches, such as ‘best fit’ framework synthesis, a systematic search strategy was undertaken to comprehensively identify all available studies and ensure that all possible data which may contribute to the synthesis were available [24–26].
The SPIDER framework[27], adapted from the PICO framework for qualitative systematic reviews, was used to define the search terms (Table 1).
Following several scoping searches, the bibliographic databases CINAHL, Psychinfo and Web of Science were searched for relevant studies. These databases are recommended for use in qualitative syntheses as they have complete indexing for qualitative studies [24,28]. The search was limited to English language articles, published in peer reviewed journals. The Trip database was then searched to identify grey literature sources. Searches were limited to articles published in the last ten years between 2011 and early 2023, to focus on current rehabilitation services and advances in prosthetic technology, and any shifts in societal acceptance of disability. The search strategy is described in Table 2.
Screening process
Two reviewers (CO and AD) undertook study selection using Rayyan, a web application for systematic reviews (Rayyan Systems Inc.). Following the removal of duplicates, CO screened all titles and abstracts with AD screening a random sample of 13% of abstracts. Agreement between reviewers was 99.6% with a single paper requiring discussion before it was excluded. CO then undertook full text screening using the inclusion and exclusion criteria (Table 3). Studies including mixed populations, i.e., prosthetic, and non-prosthetic users, were only included if data specific to the population of interest was presented independently in the analysis to ensure the outcome domains of importance were relevant to lower limb prosthetic users. Undecided papers were reviewed by AD and MDH and agreed upon following discussion.
Critical appraisal
Critical appraisal within a qualitative synthesis is controversial [28]. Researchers dispute whether or not to undertake it, how to do it, whether to exclude studies as a result of it, and finally how to integrate critical appraisal findings into the main body of the synthesis [24,29]. Despite these questions there is a growing trend towards including critical appraisal within a qualitative synthesis, and it is recommended as part of the ‘best fit’ framework synthesis approach [25,26].
The critical appraisal process was used to give context to the findings presented in the synthesis, and comment on the quality of the overall sample [25,26]. The CASP tool [30] was used to undertake critical appraisal. Initially 10% of the papers were appraised by two reviewers (CO and MDH) to set quality expectations within each CASP question and compare and agree on the appraisal approach. CO then continued to appraise the remaining papers seeking advice and agreement from MDH where required. To summarise the findings, each quality appraisal response from the CASP tool was allocated a score from 1-3 (1=yes, 2=can’t tell and 3=no). No studies were excluded due to perceived poor quality, to ensure all possible outcomes of importance were considered at this stage, and instead they were ranked in terms of quality.
Data extraction
Data extraction was undertaken by CO in two stages. Firstly, study-related data were extracted including the aim, design, sample size, recruitment setting, data collection method and geographical location, as well as details about the included population such as time since amputation, cause of amputation, sex, level of amputation and age range. Data were extracted to describe the studies and the characteristics of the study samples.
The second phase of data extraction addressed the qualitative findings of the included studies. Data were considered as that which were presented in the results or findings sections of the papers, and included both verbatim quotations and interpretations made by the study authors which were clearly supported by the study’s data [29]. Data were imported into NVIVO software (QSR International, Melbourne, Australia) for analysis.
Stages of analysis
Stage 1. Framework development
‘Best fit’ framework synthesis [25] uses an ‘a priori’ framework based on an existing conceptual model to synthesise study data and examine and develop new iterations of the model based on findings from the wider literature. An initial conceptual model of outcome domains of importance was developed by these authors using a primary qualitative approach to explore the lived experience of prosthetic users. This first stage model acted as the pre-existing conceptual model underpinning the ‘a priori’ framework, and for clarity will now be referred to as the pre-existing model.
An ‘a priori’ framework was developed (table 4) based on the pre-existing model. Domains were described using first person statements to ensure that the voice of the prosthetic user was not lost during the synthesis process. Each framework domain was also accompanied by an in-depth description to aid consistency of coding [25,26].
Stage 2: Analysis
Data describing the included studies and their samples were analysed using descriptive statistics to give context about the qualitative approaches taken and the overall review population.
Data synthesis from the ‘findings’ sections of the included articles was undertaken in two steps. Step one involved open line by line coding of the data, codes were then mapped onto the domains and subthemes described in the ‘a priori’ framework (Table 4).
Codes that did not fit easily into the framework were collated separately in NVIVO and analysed in a second step, independent of the framework synthesis, using thematic analysis as described by Braun and Clarke [31–33]. This dual approach using inductive thematic analysis in addition to the more deductive framework synthesis (Table 5) allowed previously unidentified concepts related to outcome domains of importance to arise from the data.
Stage 3: Conceptual model development
The findings from the framework synthesis were reviewed by the research team to understand where the review data supported pre-existing domains and where they did not. Newly identified themes were reviewed against the pre-existing conceptual model and through discussion and reflection, were added or used to refine the model until consensus was reached on a second iteration.
Results
Summary of included studies
Searches identified 2709 records, which were filtered down to 101 potentially relevant articles following removal of duplicates and screening of titles and abstracts. Thirty-nine of these studies met the inclusion criteria, with an additional study identified via citation chaining (figure 2).

The studies identified explored the experiences of 539 participants, 193 of whom were female (35.8%). Demographic data regarding cause of amputation were available from 31 studies representing 444 participants (82.3%). Across all studies, the causes of amputation were trauma (n=206, 46.4%), diabetic dysvascularity (n=130, 29.3%), cancer (n=44, 10%), infection (n=37, 8.3%) and congenital aetiologies (n=6, 1.4%). Demographic data describing level of amputation were available from 34 studies (n= 499, 92.6%). The levels of amputation were transtibial level (n=286, 57.3%), transfemoral (n=128, 25.7%), ankle (n=13, 2.6%), knee (n=22, 4.4%) and hip (n=6, 1.2%) disarticulation amputations. Forty three participants experienced bilateral limb loss (8.6%). The age of participants ranged between 18-81 years. The study aims and sample characteristics are described in table 6.
The studies were undertaken in 15 different countries (Figure 3), with 486 (90.2%) participants living in high-income countries, according to the World Bank definition [73]. Eleven (2%) participants lived in upper middle-income countries, 36 (5.7%) in lower middle-income countries and 6 were not stated (2.1%). No participants were included from low-income countries.

Methodological quality of included studies
The quality of papers included varied considerably. Overall, there was a little consideration of the relationship between the researcher and the participants, which was only adequately discussed in 12 of the 40 studies. Critical examination of the potential influence the researcher may have is important to provide insight into how their assumptions may have impacted or introduced bias to the results [74].
The other notable quality concern was recruitment of participants. Only 23 of the studies adequately described why participants selected for the study were appropriate to answer the research question. Many studies used convenience sampling approaches which may have led to samples with little variation, which do not represent the characteristics of target population [34,42,69,72,48,50,52–54,58,65,67]. CASP scores (out of 27, higher indicating poorer quality) ranged from 9-22. It is important to note that the findings described in this paper are supported by articles scoring across this range. The results of the critical appraisal process are summarised in Table 7.
Best Fit Framework Synthesis
The ‘best fit’ framework synthesis illustrated that the experiences discussed within the included papers, undertaken in a variety of contexts, fit well into the pre-existing conceptual model. All of the model’s domains were supported by the qualitative data (Table 8).
Additional thematic analysis
Although additional data were identified which did not fit easily into the framework, following thematic analysis it became clear that they expanded the existing outcome domains of importance, rather than describing new ones. The next sections illustrate how each domain has been re-specified or developed, and provide additional context from the synthesis with relevant quotations. Domain changes are identified in bold underlined text within the following tables.
Domain 1 - I am able to participate in my important activities and roles
The first domain ‘I am able to participate in my important activities’, set out in table 9, was expanded to include an additional subtheme describing the importance of returning to valued roles.
Subtheme 1.4 - Fulfilment of roles
The subtheme of role fulfilment is linked to ‘participation in important activities’, and was discussed in 13 papers [13,34,39,40,42,43,45,48,61,65,66,70,71]. Fulfilment of a role such as a parent, spouse or valued member of the community, was described as an important outcome following lower limb amputation. Role fulfilment was described alongside valued activities, but additional meaning was apparent when participation in the activity enabled previously valued self-identities, for example, holding a partner’s hand when out for a walk, or being able to go to the park and play with their children.“And if we go for a walk, I’m able to hold my wife’s hand. I haven’t been able to do that for eight to ten years. Some people might think that isn’t a big deal, but to me it means a lot.” (Jon) (Hansen et al., 2019)
About 4 months later after my amputation we actually went to the park and slid down the slide with her, swung on the swing, and ran around the park. I don’t even want to think about my life without doing that.” (Crawford et al., 2016)
Fulfilling previous roles appeared to create a sense of normality for participants as well as promoting adjustment by building confidence and self-worth.feeling responsible for the household allowed her amputation not to matter, allowing her to go on with life despite her altered body. (Ward Khan et al., 2021)
Being mobile in their communities enabled participants to actively participate in society: … I am the secretary of the ward committee. I meet in disability forums and write minutes … I go on my own. (Ennion and Manig, 2019)
Domain 2 - I can participate in my important activities in the way I want to
A subtheme of the second domain describing how people with limb loss want to participate was modified to reflect being able to do activities well, in addition to doing them easily (Table 10).
Subtheme 2.2 - Doing my activities easily and well
Data describing participation in sport [13,36,63] raised the issue of doing an activity well. Participants described the need to perform well during sport to be competitive, not performing well could lead to reduced participation.Now, if I swim, the speed is gone and you always have a disadvantage… swimming is not what it used to be, all elderly swim faster than me……I stopped with it…’’ (Bragaru et al., 2013)
Domain 3 – My prosthesis works for me
Originally domain three described the need for a prosthesis that is comfortable and easy to use. This domain was well supported by the data (table 8); however additional data also described the importance of prosthesis functionality, i.e., knees and feet, in enabling valued activities. This led to the domain being restructured into three subthemes (table 11). The first two subthemes describe the original domain of ‘comfort and ease of use’. An additional third subtheme now describes the importance of a prosthesis which enables participation.
Subtheme 3.3 - My prosthesis enables me to participate
The function of prosthetic components and how they enable people to participate was described in 18 studies [13,35,60–63,65,66,71,72,36,41–43,48,52,55,57]. Participants described wanting a leg that was waterproof so they could go fishing, or a flexible ankle so they could lift objects at work. A limb that did not enable function could prevent participation or make it more challenging [35,36,72,41,48,55,57,61,65,66,71].
Like the last time when I went to the Amputee Clinic, I said, ‘I like to go fishing and I would like to go canoeing a little bit and stuff, but I can’t get this prosthesis wet, is there a type of prosthesis I can get wet? (Lehavot et al., 2022)
There’s a lot of lifting in my job and fitting and stretching, not having one of the ankles, you lose a lot of balance and so you do tend to use your back like a crane a lot more than that I did when I had two legs, just ‘cause it doesn’t, you haven’t got the balance so you just, you find yourself by necessity bending when I know I should be bending from the knees but I can’t get the lift off a prosthesis in the same way (Mitchell, FG3) (Devan et al., 2015)
Trust in the prosthesis not to give way underneath them or break also appeared to be an important factor [35,36,72,41,48,55,57,61,65,66,71].
“It takes me a little bit to trust my leg that when I take a step, it is going to be there. I have had it break on me too. I have had to gain that trust with my leg then lost it, then gained it, then lost it. So over time it has been hard for me to really trust it. That when I take a step it’s going to be there for me. It’s not going to break. It’s not going to send me flying” (Morgan et al., 2020)
participants identified the pervasive fear of falling as the major issue, as they did not trust the knee unit to appropriately respond and provide stability. This affected mood and willingness to engage in daily activities (Young et al., 2021)
Insufficient trust in the prosthesis was shown to prevent participation in important activities or require adaptation. Conversely trust appeared to inspire confidence in the limb, as well as individual capabilities.
If I feel like I can trust the leg or socket, then as far as being mobile, I feel like I can do… anything.” (Hafner et al., 2016)
Domain 4 – If I have pain, I can manage it
The analysis did not reveal any new information relevant to this domain.
Domain 5 – I am able to accept my new normal
Large amounts of the data from the included studies were mapped onto this domain which has been expanded and renamed in parts (Table 12). The subtheme ‘Chasing normality’ was renamed to
‘Feeling a sense of normality’ to better capture the domain as described by people with limb loss. The subtheme ‘adjusting to limb loss’ was expanded and is now presented in two subthemes highlighting the importance of ‘adapting and accepting my limitations’ and ‘accepting my appearance’. An additional fifth subtheme was also identified describing lifelong health and wellbeing.
Subtheme 5.2 - Adapting and accepting my limitations
Data from 14 studies supported this subtheme [35,37,65,68–70,42,46,47,50,57,59,61,64]. Participants discussed the need to adjust to the changes they had experienced by adapting how they did their daily tasks.
For example, a participant stated he could not squat or be down on one knee to change a car tire and, “That’s a limitation that I’ve adapted to. So, I just put a stool down and then sit on the stool, and then do what I gotta do. So, you just have to take the limitations, and then adapt to do things that way,” (69 years old; 2.5 years post-TTA). (Miller et al., 2020)
Some participants described these adaptations as frustrating and indicative of the lives they had lost.
It’s hard I guess you have to think about things a little bit differently. How you do things, takes a bit longer to do… and that sort of thing which is a bit frustrating… you knew what you could do before and you’re never going to achieve that again now. (Male, Transfemoral, 35-50 yrs old) (Keeves et al., 2022)
However, participants appeared to view success as accepting what they could no longer do and focusing on what they could do. This seemed to be enabled by a problem-solving attitude and engendered a sense of pride in achievements.
There are just so many more possibilities than you ever thought there would be. I can’t do this, I can’t do that. You spent so much time trying to get back to who you were, and this event says, you may be not be able to get back to who you were but look at all these amazing things you can do and can go on to achieve. It opens the gate to any other ideas you had in mind that you thought you couldn’t do; it’s just amazing. You realise that you are capable of so much more than you thought you were. (Wadey and Day, 2018)
Subtheme 5.3 - Accepting my appearance
Data from 23 of the studies focused on the importance of adjusting to an altered appearance following amputation [34,35,56,57,59–61,63–66,69,36,70,71,38,40,48–50,52,55], both in terms of how participants saw themselves, and how they perceived others saw them.“I admit that I wanted to quit studying at the university many times due to that feeling I had. Even if I tried to convince myself to live with my new different look peacefully and accept my new self…I am in a constant battle from the inside.” (female, 26 years). (Abouammoh et al., 2021)
This was often described in scenarios where staring or comments from others may have reinforced a negative self-image [36,71]. However, interaction with others was also described positively in accounts of acceptance from others leading to greater self-acceptance [40,56,64,69].
Witnessing someone else’s acceptance of the prosthesis that they themselves had sometimes struggled with helped them to feel understood and accepted for who they were (Mathias and Harcourt, 2014)
This interaction was also described in reverse with greater self-acceptance appearing to result in improved interactions with others [40,56].Samantha reflects on how her own growing sense of comfort about the prosthesis had had a positive impact on the reactions of others, which in turn had increased her sense of confidence further: Once I was comfortable with it, everyone around seemed to be (Samantha) (Mathias and Harcourt, 2014)
Ultimately these experiences of acceptance were viewed positively and indicate the importance of being able to address issues of appearance during rehabilitation and recovery. Some participants described using clothing for concealment purposes to manage concerns about appearance. However, clothing also appeared to contribute to concerns, especially in certain social situations [46,61,62,75,77].I suppose it’s a female thing but if you are invited somewhere and it’s a posh do and you’re getting dressed up and then you look down at your shoes. And then it’s like bloody hell, from here [head] to here [knee] I look ok, and then I have a pair of trainers on my feet. (Carly) (Day et al., 2019)
Other facilitators of acceptance, concerning both appearance and function, were described as a positive problem-solving attitude [13,41,49,53,55,56,58,62,63,65,66,70,74], being able to participate in important activities and roles [42,44–46,51,64,70,71,76], time since amputation [62], spirituality [40,53,63,71] and peer support [13,40–42,44–46,50,54,58,67,76,77].‘‘It doesn’t matter how you do it because everybody [peers] has something, then you feel more at home and less stared at …… you feel less different….and then you accept it (Bragaru et al., 2013)
Subtheme 5.5 - Lifelong health and wellbeing
Participants in 9 of the included studies highlighted concerns about the impact amputation and prosthesis use would have on their health and wellbeing throughout their life course [36,39,41,44,56,60,61,70,71]. Participants described concerns about the impact of amputation on their remaining joints [61], the need to remain physically active to avoid health issues later in life, and to manage weight gain [36,39,56].I think just talking about hopping. I have an example of what happens to you 20 years later. I had really bad arthritis in my knee. I have torn my ACL and if I had not [hopped on one leg] growing up, it probably would be better. (Morgan et al., 2020)
For the ones who stated that they cannot live without it, ‘‘sport is more a necessity’’ and, even if it was ‘‘not perceived as a fun activity’’, the individual still participated in sports because otherwise he or she had the feeling that it would have negative consequences for his or her health. (Bragaru et al., 2013)
Interconnected nature of outcome domains
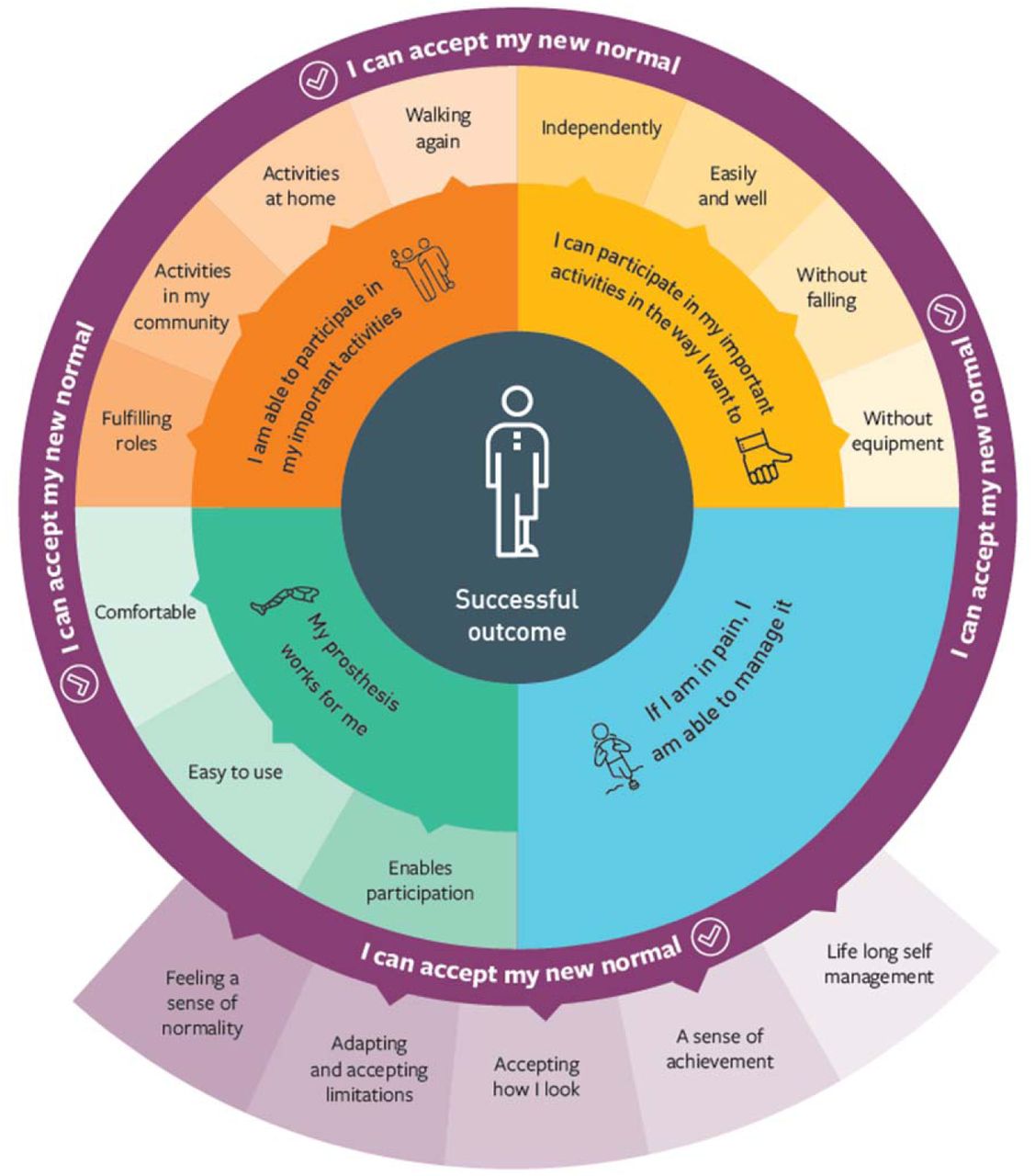
Data from the qualitative synthesis demonstrated that outcome domains of importance are interconnected, which was first introduced in our qualitative paper developing the original conceptual model [20]. Many examples were presented of how the different domains interacted, for example, how socket comfort issues prevented participation which in turn impacted adjustment and mental wellbeing, or how a lack of trust in the prosthesis caused a fear of falling, which led to reduced community participation. This analysis concurs that a successful outcome appears to be multi-faceted and requires a multi-domain measurement approach, if the outcome of prosthetic rehabilitation is to be captured in a holistic, meaningful way. Figure 4 visualises the expanded ‘ECLIPSE’ model, and the interconnected nature of the domains of importance.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
This review presents a modified and enhanced conceptual model of outcome domains of importance following lower limb prosthetic rehabilitation from the perspective of people with limb loss. Having been initially developed during a primary qualitative inquiry with 37 prosthetic users [20], it has now been rigorously examined in this systematic review using data from 40 papers describing the experiences of 539 lower limb prosthetic users from a variety of settings. The application of ‘best fit’ framework synthesis allowed us to re-examine and review domains of importance in the context of the lower limb loss literature and produce a second iteration, now named the ECLIPSE model, which more comprehensively describes this phenomenon.
The systematic review demonstrated that many of the original domains in the pre-existing model were supported by data from the literature. Thus, the model illustrates the importance of domains such as being able to participate in meaningful activities in a way individuals are happy with, having a comfortable and easy to use prosthesis, being able to manage pain, and acceptance of the new normal. However, our understanding of these concepts has been deepened during this synthesis and has led to several of the domains being expanded and re-specified.
The first domain of the ECLIPSE model described the ability to participate in important activities following prosthetic rehabilitation. Data from the review identified that following limb loss people also valued being able to return to important roles. Role fulfilment was often described alongside valued activities, with the valued activity appearing to gain additional meaning when participation enabled a return to previously valued roles. This phenomenon has also been described following traumatic brain injury [76], stroke [77] and during older persons rehabilitation [78]. A meta synthesis of studies exploring experiences of recovery following traumatic brain injury reported that returning to valued roles had a significant impact on individuals’ self-worth and that without access to these roles people struggled to define their sense of self-identity [76]. Participation in valued roles following limb loss has been described as contributing to an individual’s sense of self-identity, which can be significantly disrupted by the amputation [79,80]. However, a previous review of psychosocial adjustment to amputation suggested that successful recovery involves individuals adapting to changes in roles, alongside functioning and body image, and incorporating these changes into a new self-identity [80].
This review also demonstrated the importance of the right prosthetic componentry as an outcome domain of importance and led to re-specification of domain three (My Prosthesis works for me). What appeared to define ‘the right’ componentry (i.e., prosthetic knee, foot, suspension system etc.) was its ability to enable participation in important activities and roles, i.e., waterproofing to enable fishing, or a stable ‘trusted’ knee for walking on uneven ground. This has been reported in qualitative studies by Liu et al. [81] and Murray [82] who describe the prosthesis as key to enabling valued activities. Many different prosthetic components, designed to meet the varied functional needs of limb wearers are currently available [83], nonetheless, it may be challenging to identify a product that enables all the different activities people engage in. Having multiple prostheses for different activities could be a solution, i.e., a cycling leg or special occasion leg. However, this may be limited by financial constraints or prosthetic service provision, and may not reflect the way people often transition seamlessly between activities throughout the day. The importance of prosthesis functionality, as well as the addition of role fulfilment to domain one (I am able to participate in my important activities and roles), highlights the need for considered discussion between patients and healthcare professionals to clearly define what activities and roles are most important, and how these can be enabled through prosthetic prescription and rehabilitation. It may also be important to discuss what functionality might be lost as prescriptions change across the life course, and how this affects participation. This patient-centred approach emphasises the need for multidisciplinary input, especially considering the role of the Occupational Therapist, both during rehabilitation and lifelong prosthetic care, in order adopt an ongoing focus on participation. This focus may also challenge the current approach to outcome measurement, where tools identify the activities included in the assessment, such as walking in a crowded shopping centre or visiting a friend’s house. Meaningful outcome measurement may require tools that allow patients to define what activities are most important to them as an individual, and therefore should be captured as a measure of success.
Domain five of the ECLIPSE model, ‘I am able to accept my new normal’, was revised most significantly during this review, with three new subthemes created. This may be due to the nature of qualitative research which focuses on views and experiences and is often used to explore adjustment following amputation. The first new subtheme, ‘being able to adapt to and accept my limitations’ appears to be a common theme described in the rehabilitation literature characterising recovery from trauma or the management of long term conditions, i.e., anterior cruciate reconstruction [84], Parkinson’s Disease [85] and traumatic brain injury [86]. A study by Rosengren et al., [85] exploring the experiences of patients with Parkinson’s disease found that greater life satisfaction is achievable as people adapt to their new life situation, which involves a process of transition often based on acceptance.
This review also highlighted the need to adjust to an altered appearance following amputation. The wealth of literature describing this outcome led to its creation as a new subtheme and appeared to suggest that individuals need to adjust to how they see themselves, as well as their perception of how others see them, and that these experiences are intricately linked. This is supported by Cooley’s ‘Looking-Glass self’ theory [87] which describes how individuals base their sense of self on how they perceive others view them. The importance of adjusting to an altered appearance following limb loss is described in several studies included in a qualitative meta synthesis by Murray and Forshaw [88]. They describe the importance of using the prosthesis to moderate the reaction of others and conceal limb loss. They also highlight that adjustment to changes in self-image appear to occur over extended periods of time as people learn to accept the limitations of the prosthesis.
Both of the subthemes, ‘adjusting and accepting my limitations’ and ‘accepting my appearance’, as well as the final subtheme describing lifelong health and wellbeing, indicate the importance of both physical and psychosocial recovery following lower limb amputation. Rehabilitation programmes need to address both aspects in an integrated way to provide holistic patient-centred care. However, it is clear interventions may not only be required in the immediate post amputation period, and that ongoing physical and psychosocial support may be crucial to address changing lifelong needs.
The interconnected nature of outcome domains of importance, first documented in the authors’ primary qualitative work [20] and supported by this review, suggests the need for a multidomain approach to outcome measurement in prosthetic rehabilitation. Many examples of how domains may influence each other were described in this analysis, for example socket comfort issues leading to reduced participation in important activities. Although the findings presented here, and visualised in the ECLIPSE model (figure 4), recognise the interconnected nature of domains of importance and the need to measure them in a holistic way to capture meaningful success, further research is needed to understand the nature of the relationships between domains.
The ECLIPSE model presents a patient-centred representation of outcome domains of importance following lower limb prosthetic rehabilitation. The model could be used to direct the course of rehabilitation and highlights the need for physical and psychosocial interventions. Although several professional networks have published prosthetic rehabilitation guidelines [5,15,89,90], none include the views of patients, and no guidance is available to inform psychosocial management. Despite many papers describing the psychosocial impact of amputation [88], little research has been undertaken to evidence treatment options. Future work is needed to understand how the domain of ‘accepting my new normal’ can be addressed during prosthetic rehabilitation.
The ECLIPSE model also provides guidance for which domains are most important to measure following prosthetic rehabilitation, or in research, and could underpin a future Core Outcome Set. However, given the previously described challenges of meaningful patient involvement in COS development [12], care needs to be taken that the contribution of wider stakeholders in the COS process does not diminish the voice of prosthetic users themselves. The OMERACT initiative [91] which develop COS’ for Rheumatoid arthritis have acknowledged this concern and developed a patient COS which explicitly acknowledges that what is important to patients may be different and in need of specific consideration [92]. The ECLISPSE model could represent a patient Core Outcome Set, informing measurement in both research and clinical practice, and ensuring a person-centred focus. Future work is required to identify outcome measurement tools which capture these domains.
The design and quality of studies included in this review varied considerably. Combined, they capture the experiences of a large sample (n=539) of lower limb prosthetic users living in 15 different countries. Views and experiences from participants with different levels of amputation, a variety of causes and a wide age range were included, representing a varied sample capturing many different voices. However, despite the range of study settings, 90.2% of participants live in high-income countries. Far fewer qualitative studies have been undertaken exploring the lived experiences of lower limb prosthetic users living in low- and middle-income countries (LMICs). Due to limited representation of these individuals, it is unclear whether the ECLIPSE model describes outcome domains of importance with a prosthesis in LMICs. Further research is required to identify and understand important domains in different social and culture settings, as well as exploring how they vary between countries. This is of particular importance as it is estimated that 80% of the world’s population living with a disability live in LMICs [93], and the Global Burden of Disease study 2019 indicates an increasing international amputation prevalence of 176 million [94]. Previous outcome measure consensus work in prosthetics, undertaken by ISPO, also highlighted that many of the measurement tools for use following amputation have been developed in high income countries and call for development of measures suited to LMICs [8]. However, without first understanding which domains are most important to measure in these settings, outcome measure developers may struggle to capture what is meaningful to patients.
Limitations
When considering the findings of this review it is important to understand that the domains identified in the analysis have been generated from studies with a range of quality scores. Due to previously described issues with critical appraisal as part of systematic reviews of qualitative literature [24,28,29,95], no studies were excluded but were scored and ranked. Although this a common approach used in qualitative syntheses, it is not how the CASP tool was intended for use and should be viewed with caution.
A further limitation of the review is the potential for confirmation bias within the analysis as the authors pre-existing conceptual model was used to inform the ‘a priori’ framework. Steps were taken to minimise the risk of shoehorning data into the framework by carrying out open line by line coding as the first step in the analysis process and undertaking a separate thematic analysis on data which did not fit easily into the framework, which was then used to further develop the model. A reflexive journal was also kept throughout by the lead author to critically consider methodological and analytical decisions.
The inclusion of only peer reviewed publications written in English led to a single relevant paper being excluded which may have contributed to the findings. The decision was taken not to use translation software as this may have altered the meaning of quotations. The review also took a broad approach to the search strategy, identifying studies which explored the experiences of lower limb prosthetic users, as few studies were available describing outcome domains of importance. Although this wide focus ensured comprehensive inclusion of the available evidence, the studies did not set out to explore meaningful recovery requiring researcher judgement to identify data relevant to the research question. This also required researchers to view the data through a different lens than was originally intended, potentially reinterpreting its meaning.
Conclusion
This synthesis of qualitative findings from 40 studies representing the views of nearly 600 people provides a rigorous foundation for understanding outcome domains of importance following lower limb prosthetic rehabilitation. Our focus on the patient’s perspective ensures that the ECLIPSE conceptual model describes a meaningful recovery in the lives of those with limb loss, particularly in high income settings.
The ECLIPSE model is an accessible patient-centred representation of recovery and could be used by clinicians to shape and direct the focus of rehabilitation programmes and inform goal setting, as well as direct the evaluation of their impact through the selection of appropriate outcome measures. The interconnected nature of outcome domains of importance also highlights the need for a holistic approach to outcome measurement, capturing success in all aspects of the patient’s life.
The domains which comprise the ECLIPSE model could also inform the selection of outcomes within research. They could underpin a future core outcome set (COS) or represent a standalone patient COS, which may be more appropriate for rehabilitation settings where the aim is to enable return to previous lives. Future work is needed to understand how well current outcome measures capture the domains described in the model and whether new measures need to be developed.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.
- 18.
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵



