
Abstract
Background Tixagevimab and cilgavimab (AZD7442) are two monoclonal antibodies developed by AstraZeneca for the pre-exposure prophylaxis and treatment of patients infected by SARS-CoV-2. Its effectiveness and safety in patients hospitalized with COVID-19 was not known at the outset of this trial.
Methods DisCoVeRy is a phase 3, adaptive, multicentre, randomized, controlled trial conducted in 63 sites in Europe. Participants were randomly assigned (1:1) to receive placebo or tixagevimab-cilgavimab in addition to standard of care. The primary outcome was the clinical status at day 15 measured by the WHO seven-point ordinal scale. Several clinical, virological, immunological and safety endpoints were also assessed.
Findings Due to slow enrolment, recruitment was stopped on July 1st, 2022. The antigen positive modified intention-to-treat population (mITT) was composed of 173 participants randomized to tixagevimab-cilgavimab (N = 91) or placebo (N = 82), 91.9% (159/173) with supplementary oxygen, and 47.4% (82/173) previously vaccinated at inclusion. There was no significant difference in the distribution of the WHO ordinal scale at day 15 between the two groups (odds ratio (OR) 0.93, 95%CI [0.54-1.61]; p = 0.81) nor in any clinical, virological or safety secondary endpoints. In the global mITT (N = 226), neutralization antibody titers were significantly higher in the tixagevimab-cilgavimab group/patients compared to placebo at day 3 (Least-squares mean differences (LSMD) 1.44, 95% Confidence interval (CI) [1.20-1.68]; p < 10−23) and day 8 (LSMD 0.91, 95%CI [0.64-1.18]; p < 10−8) and it was most important for patients infected with a pre-omicron variant, both at day 3 (LSMD 1.94, 95% CI [1.67-2.20], p < 10−25) and day 8 (LSMD 1.17, 95% CI [0.87-1.47], p < 10−9), with a significant interaction (p < 10−7 and p = 0.01 at days 3 and 8, respectively).
Interpretation There were no significant differences between tixagevimab-cilgavimab and placebo in clinical endpoints, however the trial lacked power compared to prespecified calculations. Tixagevimab-cilgavimab was well tolerated, with low rates of treatment related events.
Funding Trial registration: ClinicalTrials.gov NCT04315948. Registered on 13 March 2020 updated on 22 April 2021.
Introduction
Even though COVID-19 is no longer a public health emergency,1 SARS-CoV-2 continues to circulate worldwide, and therefore individuals unable to mount an adequate immune response (e.g. the elderly and the immunocompromised), or unvaccinated/disease naïve individuals at risk for severe COVID-19, remain vulnerable. Although immunomodulatory agents (corticosteroids, interleukin-1 and 6 inhibitors, JAK inhibitors) and direct-acting antiviral remdesivir have been identified as effective treatments to decrease mortality in sub-groups of patients hospitalized with COVID-19,2–6 antibody-mediated SARS-CoV-2 neutralization may be another treatment option in vulnerable patient groups.
Indeed, in the ambulatory setting, the administration of monoclonal antibodies (mAbs) directed against SARS-CoV2 (intravenous sotrovimab or intramuscular tixagevimab-cilgavimab), significantly reduced the risk of hospitalization and death in patients at risk for disease progression, compared to placebo.7,8 In the hospital setting, several trials on mAbs for COVID-19 were terminated early for futility (bamlavinimab in 314 patients, and sotrovimab or BRII-196/BRII-198 in 546 patients).9,10 Several other trials showed a potential therapeutic benefit of mAbs in this setting. The open-label RECOVERY platform trial was the first to demonstrate a 28-day mortality benefit in seronegative patients at baseline for SARS-CoV-2 infection in patients who received casirivimab-imdevimab plus standard of care (SoC) compared to SoC alone.11 The company-sponsored double-blinded, placebo-controlled trial also showed that casirivimab-imdevimab treatment was associated with a significant reduction in 28-day mortality for seronegative patients, but not for seropositive ones.12 The mAb cocktail with an extended half-life, tixagevimab-cilgavimab (AZD7442), was also evaluated as an intravenous formulation in association with SoC (which included remdesivir) in the double-blinded, placebo-controlled ACTIV-3-TICO trial in 1417 hospitalized patients with COVID-19.13 Although the primary outcome of time to sustained recovery was not met, treatment with tixagevimab-cilgavimab was associated with a decreased 90-day mortality.
Since these trials were completed, the virus itself has evolved, resulting in the emergence of different variants of concern (VOC) and mass vaccination campaigns against SARS-CoV-2 were ramped up worldwide.14 In this context, of an evolving pandemic, we report here the results from the DisCoVeRy platform trial that evaluated the efficacy and safety of intravenous tixagevimab-cilgavimab in SARS-CoV-2 antigenic positive patients (i.e those with a high SARS-CoV2 viral load) hospitalized with COVID-19, and followed-up to day 90.
Materials and Methods
Study design
DisCoVeRy is a phase 3, adaptive, multicentre, randomized, double-blind, superiority trial for evaluating the efficacy and safety of drugs for the treatment of adults hospitalized for COVID-19. The first four interventions evaluated (lopinavir/ritonavir, lopinavir/ritonavir plus IFN-b-1a, hydroxychloroquine, and remdesivir) have been stopped for futility and the results reported elsewhere.15–17 The present analysis is based on the protocol version 15.0 of September 20th, 2021, which evaluates the cocktail of two monoclonal antibodies (mAbs), tixagevimab and cilgavimab developed by AstraZeneca. The study was conducted across 63 sites in 13 European countries (Austria, Belgium, Czech Republic, France, Greece, Hungary, Ireland, Luxembourg, Norway, Poland, Portugal, Slovakia, and Spain). The trial was approved by the Ethics Committees in each country and is sponsored by the Institut national de la santé et de la recherche médicale (Inserm, France); it was conducted in accordance with the Declaration of Helsinki.
Participants
Eligible participants were adults (> 18 years) hospitalized with SARS-CoV-2 infection confirmed on a RT-PCR performed on a nasopharyngeal (NP) swab within the 5 days preceding randomization, and a time between onset of symptoms and randomization of less than 9 days (extended to 11 days from September 20th, 2021, protocol V15). Participants with prior receipt of investigational or licensed mAb or vaccine indicated for the prevention of SARS-CoV-2 infection or COVID-19 were excluded. From September 20th, 2021 (protocol V15), inclusion of patients with initiated (one dose) or completed (two doses) vaccination was allowed in a proportion of 20% of enrolled participants, provided they would not receive an additional dose in the 30 days following hospital discharge. Full inclusion and exclusion criteria are detailed in the appendix. Written informed consent was obtained from all participants or their legal representative.
Randomization and masking
Participants were randomly assigned in a 1:1 ratio to receive tixagevimab-cilgavimab or placebo in addition to standard of care (SoC). The randomization was stratified by region, by antigenic status obtained from the result of a rapid antigen test on a NP swab at enrolment, and with protocol V15, by vaccination status. Randomization was performed via an electronic Case Report Form and used computer-generated blocks of various sizes. The allocation of tixagevimab-cilgavimab was double-blinded.
Procedures
The participants received a single intravenous infusion of tixagevimab-cilgavimab (600 mg at a maximum infusion rate of 50 mg/minute) or placebo (a 0.9% saline solution) within 24 hours following randomization. Participants could not be treated with other monoclonal or polyclonal antibodies directly targeting SARS-CoV-2 during the study. The SoC could include corticosteroids, remdesivir, and other immunomodulatory agents at the discretion of the physician.
Participants were assessed daily while hospitalized. The evaluation of the primary endpoint was at day 15, and participants were contacted by phone to collect the data if they had already been discharged from the hospital. Follow-up assessments were scheduled at days 29, 90, 180, 365 and 456. For all participants discharged from the hospital, assessments at days 29 and 90 were organized as outpatient consultations. Assessments at days 180 and 365 were also organized as outpatient consultations, but only for a subset of 25% of patients enrolled in centers with available resources, selected at day 90, the others were contacted by phone. For the final assessment at day 456, all patients were contacted by phone.
NP swabs or lower respiratory tract samples were obtained at baseline (day 1 pre-treatment) and days 3, 8, 15 (while hospitalized) and 29. Blood samples were obtained at baseline, at days 3, 8, 15 (while hospitalized), and at days 29, 90, 180 and 365 (for the subset of patients evaluated during a medical consultation at these times).
The blood samples included samples for safety laboratory tests, serum samples for serology, drug concentration and anti-drug antibodies measurements, and serum and plasma samples for exploratory objectives.
Outcomes
The primary endpoint was the clinical status at day 15 measured on the 7-point ordinal scale of the WHO Master Protocol (v3.0, March 3, 2020). The key secondary endpoint was the time from randomization to sustained recovery, defined as being discharged from the index hospitalization, followed by being alive and at home for 14 consecutive days prior to day 90 (details in the appendix). Other secondary efficacy endpoints included: clinical status on the ordinal scale at days 29, 90, 180, and 365; change of the National Early Warning Score 2 (NEWS-2) from baseline to days 3, 8, 15 (if hospitalized), and 29; oxygenation and ventilator-free days from baseline to day 29; time to new oxygen use, non-invasive ventilation or high flow oxygen devices during the first 29 days; time to new invasive mechanical ventilation use during the first 29 days; new need for mechanical ventilation or death by day 15; time to hospital discharge; in-hospital mortality and/or at days 29, 90, 180, 365, or 456; occurrence of new hospitalization between discharge from index hospitalization and days 90, 180 and 365; occurrence of confirmed re-infection with SARS-CoV-2 between discharge and Days 90, 180 and 365.
Safety endpoints included: cumulative incidence of serious adverse events (SAEs), grade 3 and 4 adverse events (AEs), grade 1-2 hypersensitivity-related and infusion-related AEs until day 29, or AE of special interest (AESI); the discontinuation of investigational product for any reason.
Virological endpoints included the measures at baseline, days 3, 8, 15 (while hospitalized) and 29 of: the proportion of participants with detectable SARS-CoV-2 in NP or LRT samples; the normalized quantitative viral load in NP or LRT samples; and their respective change from baseline. They also included the time to first undetectable normalized quantitative viral load in NP swabs.
The pre-specified exploratory analysis of neutralizing activity of patients’ serum samples against their variant of infection, or against delta for pre-omicron variants of infection, was performed. The endpoints related to this analysis included: the neutralizing antibody titers at day 3 and day 8; the change of titers from baseline to days 3 and 8; and the proportion of patients with neutralizing antibody titers below the limit of detection (LOD).
Details on the outcomes are in appendix.
Statistical analysis
Sample size
The study was powered to detect an odds ratio (OR) of 1.5 (an OR greater than 1 indicates superiority of the experimental treatment over the control for each ordinal scale category), with a 90% power and a two-sided type I error of 0.05, for the primary endpoint. We determined that 413 evaluable, antigen positive patients were needed in each arm. Since antigen negative patients can represent as much as 30% of patients, 590 participants (antigen positive or negative) were needed in each arm. Accounting for 5% of non-evaluable patients, we needed to include a total of 620 patients per arm (details in appendix).
Populations
The intention-to-treat (ITT) population included all randomized participants analyzed in their assigned randomization group. The modified intention-to-treat (mITT) population included participants from the ITT population for whom the infusion of the allocated treatment was truly initiated. The safety population included all randomized participants, analyzed in their actual treatment group. Each population set was further categorized according to the antigenic status, thereby defining « Antigen positive » ITT and mITT. The set of all patients (i.e. antigenic positive and negative) in ITT, mITT, and safety populations are referred to as the « Global » ITT, mITT, and safety populations.
The efficacy analyses were conducted on the antigen positive mITT population, as it is hypothesized that tixagevimab-cilgavimab may be most effective in antigen positive patients. Efficacy analyses were also conducted on the global mITT population as a sensitivity analysis. Safety analyses were performed on the global safety population. The analyses were stratified by vaccination status, but not by region due to the low number of inclusions in some regions. For global populations, analyses were also stratified by antigenic status. The analyzes of the neutralizing activity of serum samples were performed on patients from the global mITT population with known or imputed variants of infection (details in appendix). Variants of infections were grouped in three categories: (a) pre-omicron (alpha, beta, gamma, delta, other), (b) omicron BA.1, (c) omicron BA.2/5 (omicron BA.2 or BA.5).
The analyses reported here were performed on the pre-specified primary database lock with all endpoints collected until day 90.
Statistical tests
The primary endpoint, clinical status at day 15 measured on the 7-point ordinal scale, was analyzed with a proportional odds model. For the key secondary endpoint, time to sustained recovery, cumulative incidence functions were estimated for each group using the Aalen-Johansen estimator, and the recovery rate ratio (RRR) for sustained recovery were estimated using the Fine and Gray method. For virological endpoints, the proportion of subjects with detectable viral loads in NP swabs were compared between groups using a stratified Cochran– Mantel–Haenszel (CMH) test. Time to first undetectable viral load through day 29 was analyzed with the same approach as for the time to sustained recovery. The log10 normalized quantitative SARS-CoV-2 viral load in NP swabs were compared between groups using linear mixed models with repeated measures for each patient, with the treatment arm as the main exposure variable, and the time of measurement, time by treatment interaction, and stratification variables as covariates. Patient effect was accounted for as random intercept (log10 copies/10 000 cells) and slope (log10 copies/10 000 cells per day). The differences in the viral loads, and in the change from baseline of the viral loads between treatment groups were estimated as differences of slopes using the linear mixed effects model.
Analyzes of neutralizing antibody titers were performed on the global mITT population, stratified by vaccination status and by variant of infection (pre-omicron; omicron BA.1; omicron BA.2/5). The log10 titers at day 3 and day 8, and the change of titers from baseline to days 3 and 8 were compared between the two arms using an ANCOVA model and results reported as least-square mean differences (LSMD). The proportion of subjects with undetectable neutralizing antibody titers at days 3 and 8 were compared between groups using a stratified CMH test. Details on the statistical tests and handling of missing data are in the appendix. All analyses were done using SAS 9.4.
Subgroup analyses
Prespecified subgroup analyses for the primary outcome, the key secondary outcome, and the differences of slopes of normalized viral loads were performed across the following subgroups: vaccination status (yes / no), clinical status at inclusion (ordinal scale 3-4 / ordinal scale 5), duration of symptoms prior to randomization (less than 5 days / 5 days or more), age (less than 65 years / 65 years or more), SARS-CoV-2 serology at inclusion (negative / positive), SARS-CoV-2 variant of infection (pre-omicron / omicron BA.1 / omicron BA.2/5), sex (female / male), and for analyses on the global mITT population, the antigenic status at inclusion (positive / negative). Prespecified subgroup analyses for the serum neutralization outcomes were performed on the following subgroups: vaccination status, SARS-CoV-2 serology at inclusion, and variant of infection. Interactions between the treatment and the subgroup variables were tested and the p-values are reported. Post-hoc subgroup analyses for the cumulative incidence of SAEs, the first safety endpoint, was also performed on the same subgroups in the safety population.
Trial safety and monitoring
There was no pre-planned interim analysis for efficacy nor futility, and none were performed. An independent data safety and monitoring board (DSMB) externally reviewed the trial data on two scheduled occasions, as pre-specified in the protocol. The trial was registered on ClinicalTrials.gov (NCT04315948) on 13 March 2020, updated on 22 April 2021. The full protocol and statistical analysis plans are available as supplementary material.
Role of the funding sources
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
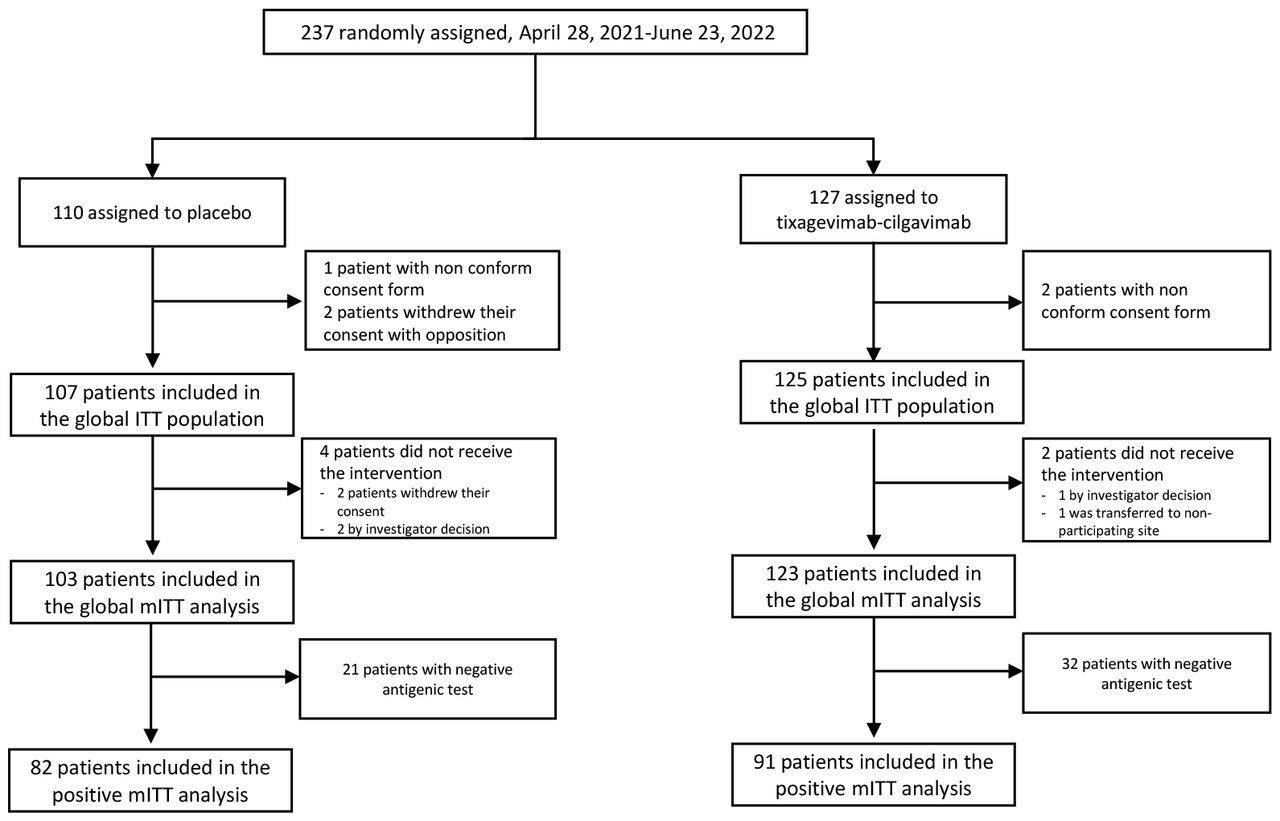
Due to slow enrolments and in-vitro data showing decreased activity of tixagevimab-cilgavimab against the omicron circulating variants,18,19 the study steering committee decided to stop the inclusions on July 1st 2022, in all participating sites, before having reached the targeted sample size. Between April 28th 2021, and June 23rd 2022, 237 participants were randomized across 34 sites in 6 European countries (France, n=206 ; Belgium, n=15 ; Norway, n=6 ; Luxembourg, n=5 ; Greece, n=4 ; Portugal, n=1). Five participants were excluded from the ITT population (no valid informed consent form, n=3; withdrawal of consent, n=2) and six excluded from the mITT population (withdrawal of consent, n=2; investigator decision, n=3; transfer to non-participating study site, n=1). Fifty-three participants had a negative antigenic status at inclusion; they were excluded from the antigenic-positive mITT population (figure 1).

Participants’ baseline characteristics are presented in table 1, without notable imbalance between arms. Among the 226 participants in the global mITT population set, 173 (76.5%) had a positive antigen test at baseline and vaccination was initiated or completed for 45.1% (102/226) of participants. In the global mITT population, the median age was 66 years (IQR 53 – 76) and 68.6% (155/226) were male. The median time from symptom onset to randomization was 7 days (IQR 6 – 9). Overall, 77% (174/226) of participants had at least one comorbid condition. Most participants were infected with one of the variants circulating before omicron (58.8%, 133/226); others were infected with omicron BA.1 (23.5%, 53/226), or omicron BA.2 or BA.5 (9.7%, 22/226). Data on the variant of infection was missing for 8.0% (18/226) of participants (no sequencing available and not imputed).
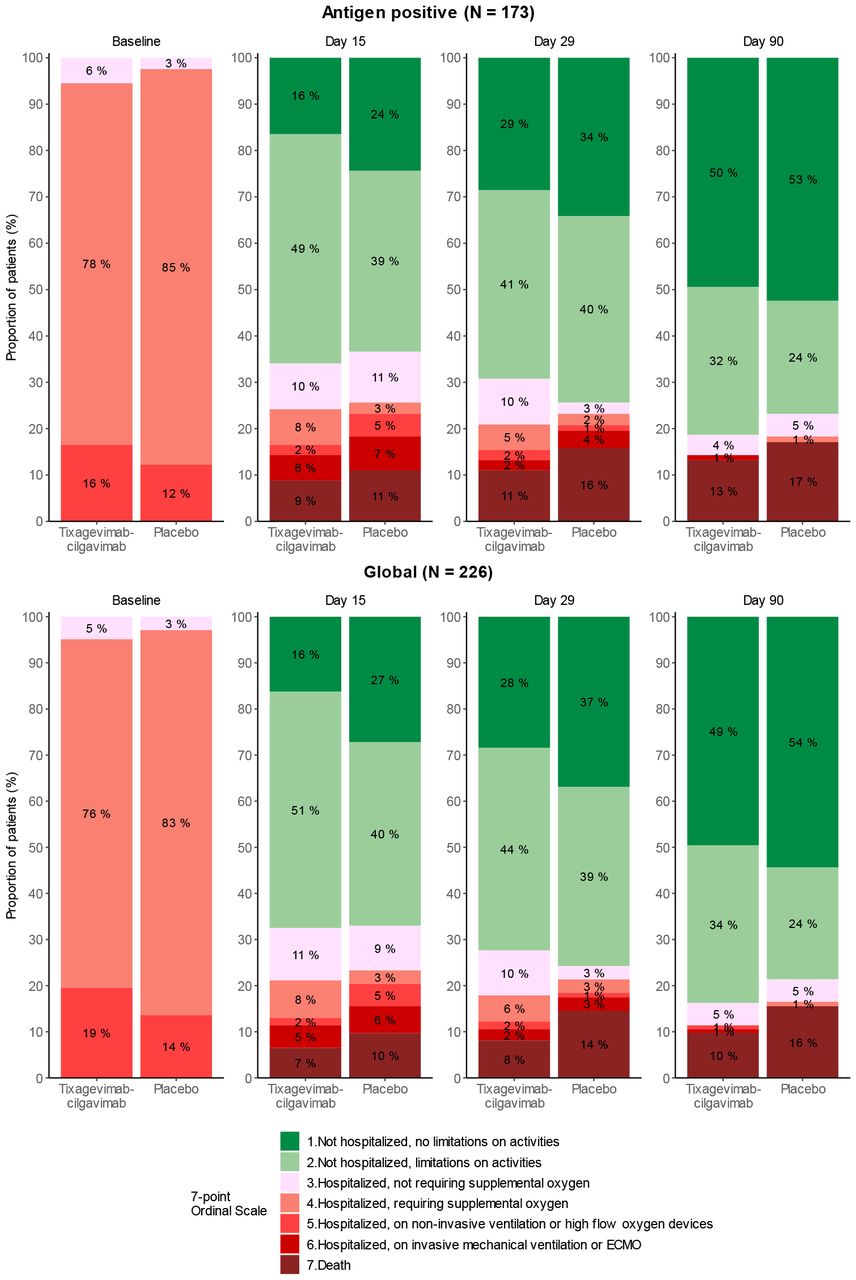
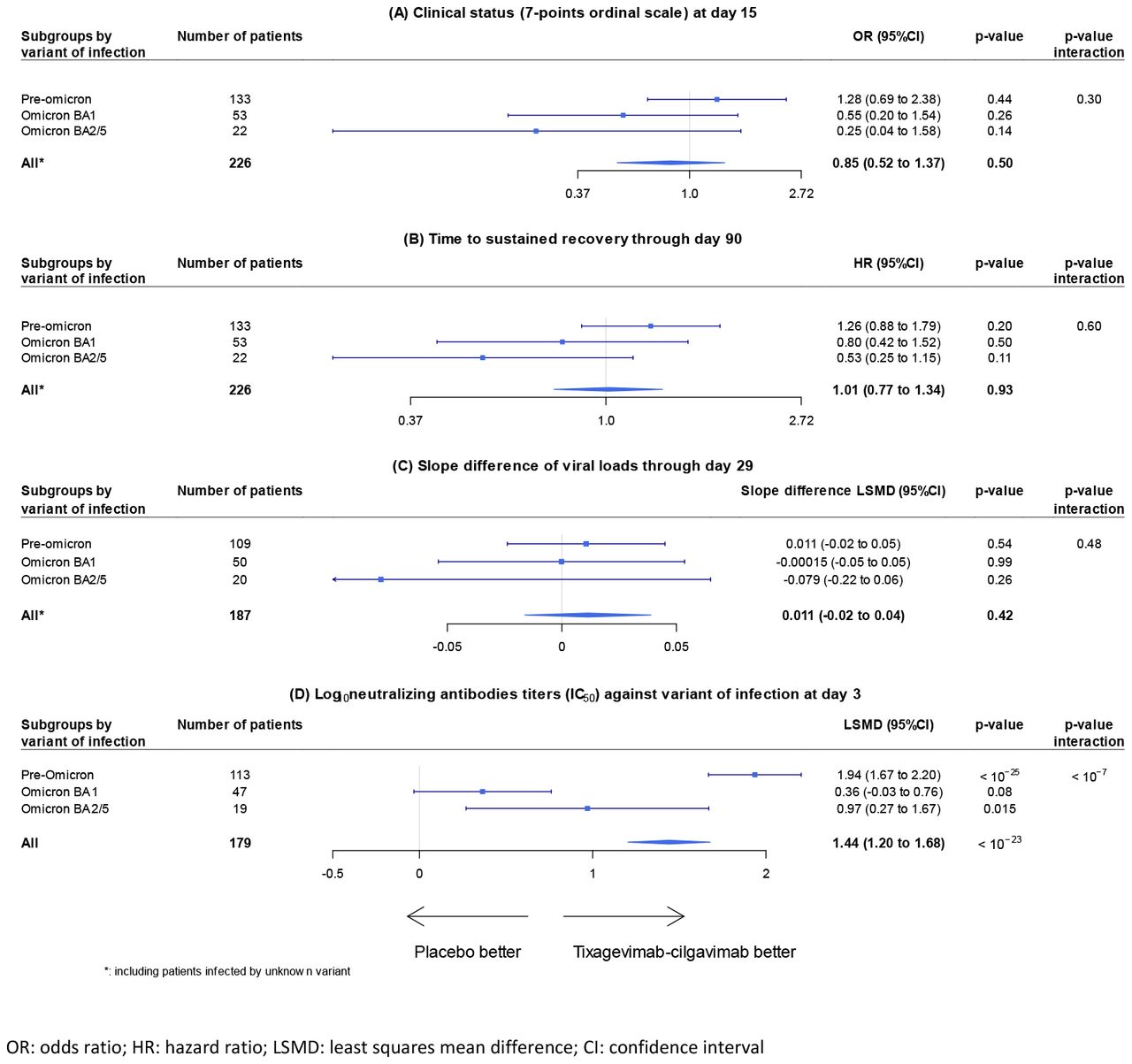
Table 2 shows the clinical status of patients in the tixagevimab-cilgavimab and placebo groups according to the WHO ordinal scale, at day 15, day 29, and day 90, for the antigen positive and global mITT populations. There was no significant difference in the distribution of the seven-point ordinal scale at day 15 between the tixagevimab-cilgavimab and control groups (figure 2; table 2). At day 15, 64.7% (112/173) of antigen positive participants were no longer hospitalized (65.9%, 60/91 for tixagevimab-cilgavimab vs. 63.4%, 52/82 for placebo), and 9.8% (17/173) had died (8.8%, 8/91 for tixagevimab-cilgavimab vs. 11.0%, 9/82 for placebo). There was no significant difference in all subgroup analyses according to vaccination status, clinical status at inclusion, variant of infection, duration of symptoms prior to randomization, antigenic status (for the global population), age, sex, or serology (figure S1, appendix). Likewise, there was no significant difference in the distribution of the seven-point ordinal scale at day 29 and at day 90 (figure 2; table 2). The median time to sustained recovery through day 90 was not significantly different between the tixagevimab-cilgavimab and placebo groups, in both the antigen positive and global populations, as well as for any of the subgroup analyses (table 2; figures S2 and S4, appendix). There was no significant interaction between the treatment and the subgroup variables exept for sex, with a greater effect of tixagevimab-cilgavimab for males in both the antigen positive and the global populations (p=0.02 and p=0.04). No significant difference was observed for any other clinical secondary endpoints (table 2; table S2; figure S3, appendix). Analysis of change from baseline in the NEWS-2 score was limited to day 3, due to an important amount of missing data at days 8, 15, and 29.

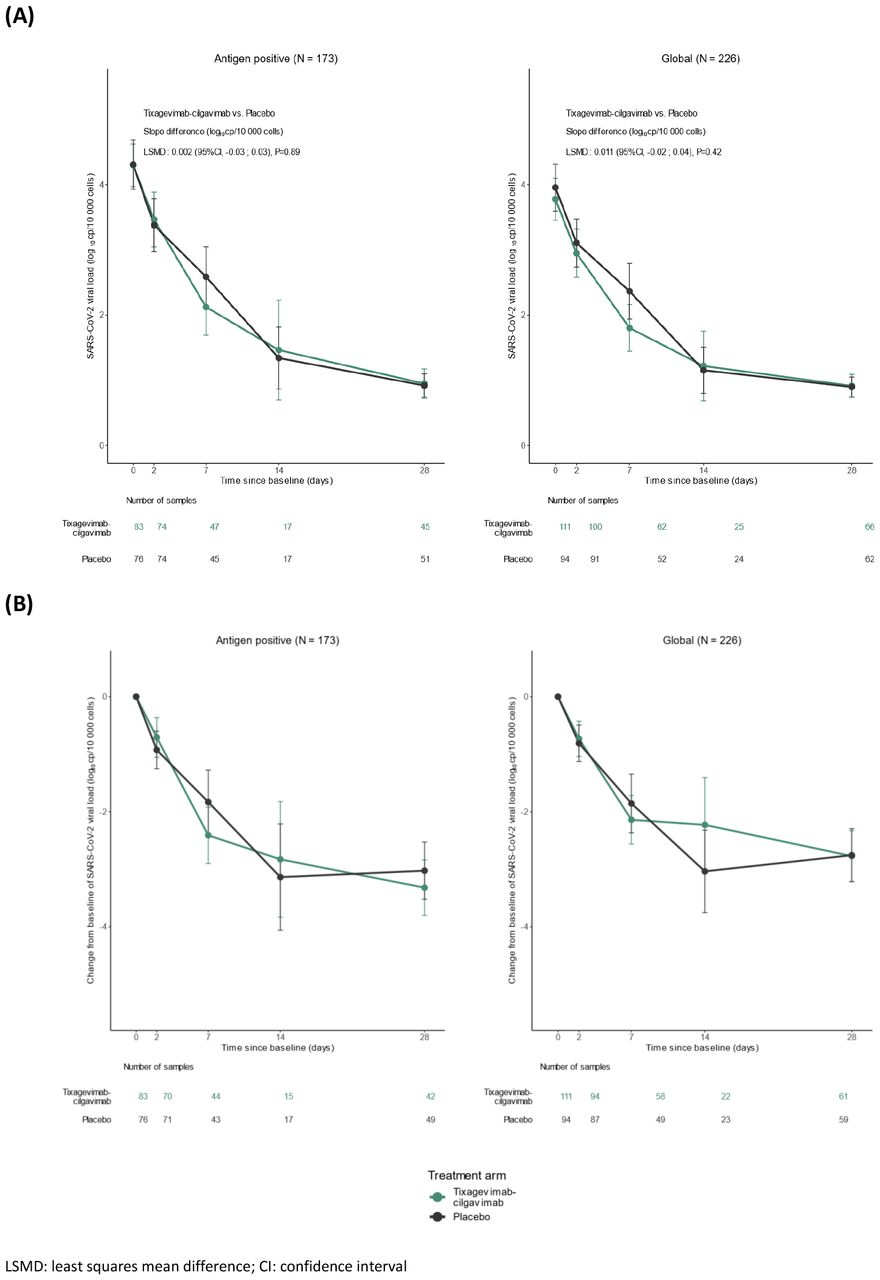
Normalized SARS-CoV-2 viral load, measured in NP swabs, were available for 205 (91%) patients at baseline, for 191 (85%) patients at day 3, for 114 (50%) patients at day 8, for 49 (22%) patients at day 15, and for 128 (57%) patients at day 29. There was no significant difference in viral kinetics from baseline to day 29 between the tixagevimab-cilgavimab and control groups, in both the antigen positive and global mITT populations. Accordingly, there was no significant difference between the two groups in the proportion of participants with detectable viral load at each time point, or in the time to first undetectable quantitative viral load through day 29 (figure 3; figure S5; tables S2 and S3, appendix).

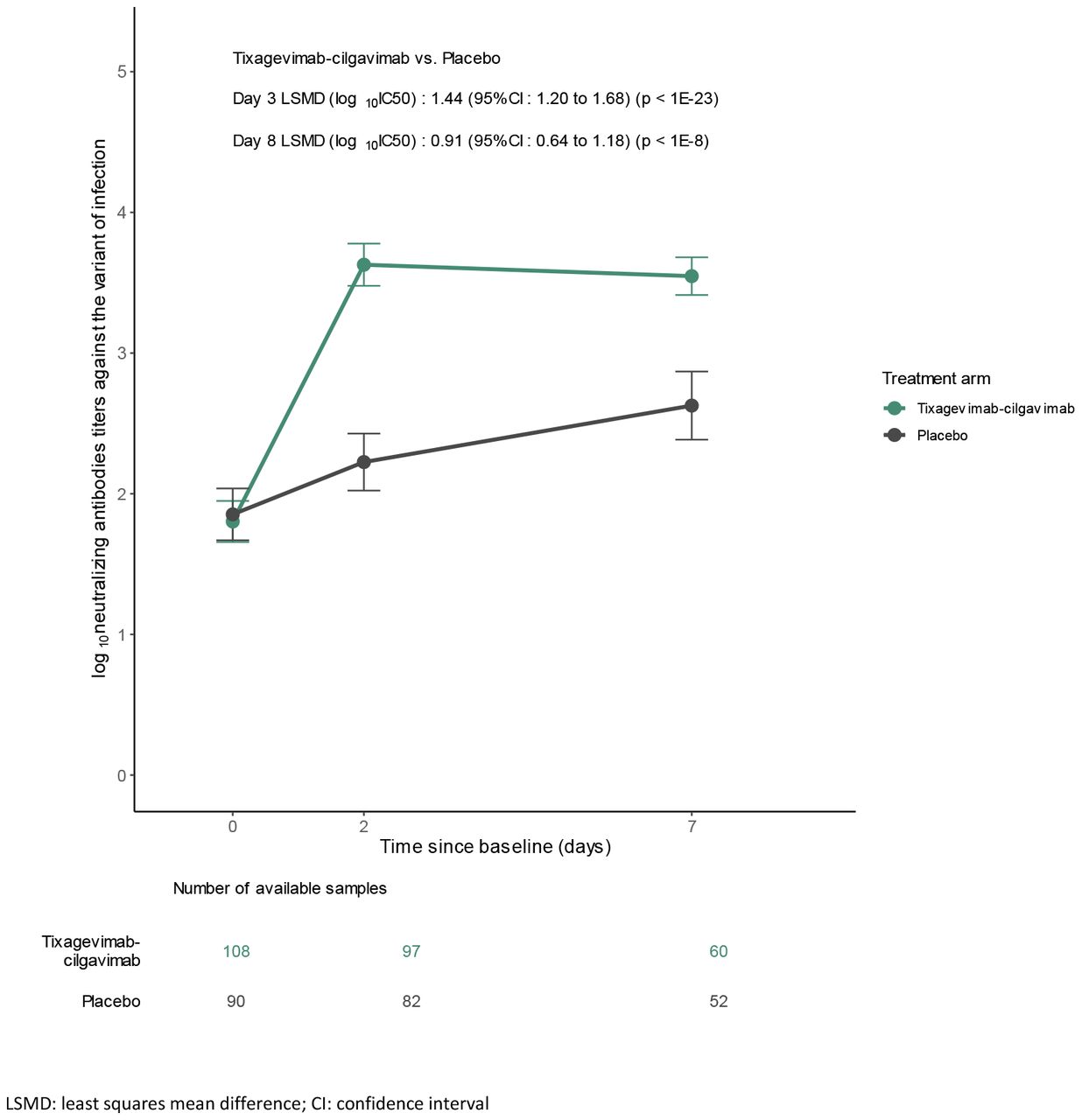
Neutralizing antibody titers were available for 198/226 (87.6%) patients at baseline, 179/226 (79.2%) at day 3, and 112/226 (49.5%) at day 8 (table S4, appendix). The proportion of subjects with undetectable neutralizing antibodies in the tixagevimab-cilgavimab arm dropped from 51.9% (56/108) at baseline, to 1% (1/97) at day 3, and 0% (0/60) at day 8, whereas in the placebo arm it dropped from 54.4% (49/90) to 30.5% (25/82) at day 3, and 13.5% (7/52) at day 8 (p < 10−9 at day 3 and p = 0.006 at day 8). Figure 4 shows the evolution of the log10 neutralizing antibody titers from baseline to day 8. There was a significantly greater increase in neutralizing antibodies in the tixagevimab-cilgavimab group compared to the placebo group both at day 3 (LSMD: 1.44, 95% CI [1.20 - 1.68], p < 10−23) and day 8 (LSMD: 0.91, 95% CI [0.64 - 1.18], p < 10−8).

Subgroup analyses showed that the difference in the increase of neutralizing antibodies was most important for patients infected with a pre-omicron variant, both at day 3 (LSMD: 1.94, 95% CI [1.67 - 2.20], p < 10−25) and day 8 (LSMD: 1.17, 95% CI [0.87 - 1.47], p < 10−9), whereas it was not significant for patients infected with omicron BA.1, and reduced for patients infected with BA.2/5. The interactions between the effects of the treatment and the variant at inclusion were significant at days 3 and 8 (p < 10−7 and p=0.01, respectively). The interactions with the vaccination status or the serology were also both significant at day 3 (p = 0.006 and p = 0.004), but not at day 8 (figure 5; figure S7, appendix). All prespecified subgroup analyses, and post-hoc analyses of clinical and virological endpoints in the subgroup of patients infected with pre-omicron are presented in the appendix.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Safety outcomes are shown in table 3. A total of 178 adverse events (AEs), including 90 serious AEs (SAEs) were reported, of which 28 (31.1%) were considered related to the investigational medicinal product. No grade 1-2 hypersensitivity-related and infusion-related AE until day 29 was reported, and one adverse event of special interest (AESI) was observed in the tixagevimab-cilgavimab group (anaphylactic shock), but considered not linked to the investigational product. In the tixagevimab-cilgavimab group, 51/123 (41.5%) patients had at least one AE, against 45/103 (43.7%) in the control group (p = 0.70); 30 (24.4%) patients in the tixagevimab-cilgavimab group had at least one grade 3 or 4 AE, against 33 (32.0%) in the control group (p = 0.18); 28 (22.8%) patients in the tixagevimab-cilgavimab group had at least one SAE, against 32 (31.1%) in the control group, although the difference was not statistically significant (p = 0.13). Among 19 fatal SAEs overall, none were of cardiac origin. The post-hoc subgroup analyses of SAEs suggested that tixagevimab-cilgavimab was safe regardless of serostatus or vaccination. It also showed, for patients infected with a pre-omicron variant, a statistically significant lower number of patients with at least one SAE in the tixagevimab-cilgavimab group, 10/70 (14.3%) against 22/63 (34.92%) in the control group (p = 0.01; figure S11, appendix).
Some patients had more than one adverse event (AE) or serious adverse event (SAE). As per protocol, AEs and SAEs do not include disease-related events (DRE).
Discussion
Here we report the results of the DisCoVeRy multicentric, platform trial comparing intravenous tixagevimab-cilgavimab plus SoC to placebo plus SoC in hospitalized patients with COVID-19, mostly infected with pre-omicron SARS-CoV-2 variants. The trial was terminated early, after only 237 of the 1240 intended inclusions, due to novel in-vitro evidence showing loss of significant neutralization activity against omicron circulating variants.18,19 Tixagevimab-cilgavimab administration was well tolerated but was neither associated with a better clinical outcome at day 15, nor with improved sustained recovery up to day 90, nor with faster viral clearance, despite a significant increase in neutralizing antibodies against the SARS-CoV-2 variants infecting individuals at days 3 and 8 in patients who received tixagevimab-cilgavimab compared to placebo.
Our results differ from those of the ACTIV-3-TICO trial, the only other randomized controlled trial that has evaluated tixagevimab-cilgavimab in hospitalized patients with COVID-19.13 The trial found a 30% relative risk 90-day reduction in mortality (9% vs. 12%; hazard ratio [HR] 0.70 [95%CI 0.50-0.97]; p=0.032). Differences in outcome results may be due to the underpowered nature of the DisCoVeRy trial, but also due to differences in patient populations, their management, and the infecting SARS-CoV-2 variants. Patients, in the DisCoVery trial, were older (median age of 66 vs. 55), and more often male (69% vs. 58%), immunocompromised (20% vs. 9%), with at least one comorbidity (78% vs. 61%), more often vaccinated against COVID-19 (47% vs. 26%), and with a higher seroprevalence for SARS-CoV-2 at baseline (60% vs. 53%) than in the ACTIV-3-TICO trial. Patients in the DisCoVery trial were more severely ill at baseline, with only 4% of patients not requiring supplemental oxygen compared to 23% in the ACTIV-3-TICO trial, with an observed overall greater mortality up until day 90 of 15% compared to 10%, respectively. When considering SoC, 61% of patients in the ACTIV-3-TICO trial received concomitant remdesivir compared to none in the DisCoVeRy trial as remdesivir was not yet considered SoC in Europe at the time of enrolment. Results of the individual patient data meta-analysis of randomized controlled trials on remdesivir later offered more conclusive evidence of remdesivir efficacy in hospitalized patients with COVID-19 not needing mechanical ventilation.6 Although the delta variant was the predominant one in both trials, the DisCoVeRy trial enrolled 40% of patients infected with the omicron variant compared to none in the ACTIV-3-TICO trial.13 The SARS-CoV-2 omicron variant has been associated with the spread of multiple sub-lineages. They harbor different spike mutations that make them more evasive to vaccine or infection-induced antibodies including therapeutic mAbs. Nevertheless, although infections due to the omicron variant have overall proven to be less virulent than prior variants including delta,20 many patients who did require hospitalization were still at risk of dying, as illustrated by the mortality rate of 15% at day 90. A significant neutralizing activity against SARS-CoV-2 was measured in serum taken on days 3 and 8 from patients infected with pre-omicron variants that received tixagevimab-cilgavimab, but was not the case for those infected by omicron variants. This is consistent with in-vitro live-virus neutralization assays showing enhanced neutralization escape to tixagevimab-cilgavimab by SARS-CoV-2 serial omicron sub-lineages in comparison to the ancestral strain or delta variant.18,19
Results of this trial concerning safety of tixagevimab-cilgavimab should also be considered in-light of other randomized trials and reports of real-life experience. A warning was issued following the post-hoc analyses of the PROVENT pre-exposure prevention trial for SARS-CoV-2; a higher proportion of cardiovascular SAEs (myocardial infarction, cardiac arrhythmia or cardiac failure) were observed in individuals with cardiac risk factors who had received tixagevimab-cilgavimab compared to placebo.21,22 Nevertheless, no significant differences in any SAEs, nor in cardiac SAEs between patients who received tixagevimab-cilgavimab (32/123 ; 26% and 5/123 ; 4%, respectively) and those who received placebo (35/103 ; 34% and 4 /123 ; 4%, respectively) were observed in the DisCoVeRy trial. Furthermore, in the post-hoc subgroup analyses of cumulative incidence of SAEs, two times fewer SAEs were observed in the tixagevimab-cilgavimab group compared to the placebo group in patients infected with a pre-omicron variant. These observations are in line with safety results from the ACTIV-3-TICO trial13 as well as a population-based propensity-matched cohort study including aggregated healthcare records from 78 million patients in the USA.23
The randomized placebo-controlled design, the inclusion of patients vaccinated against SARS-CoV-2, and those infected by other than pre-omicron SARS-CoV-2 variants, the collection of data on normalized viral loads, and on neutralizing antibody titers are strengths of our study. Nevertheless, the final trial size was underpowered to compare safety, clinical efficacy, and virological effects of tixagevimab-cilgavimab to placebo. The early termination of this trial, with only 19% of the planned enrolment, reflects the difficulties to evaluate mAbs in the ever-changing landscape of a pandemic due to a virus with evolving genomics.24,25 Already by mid-2022, mAbs previously approved by the US Food and Drug Administration and the European Medicines Agency for clinical use were no longer recommended. Thus, clinical investigators were wary of including patients in our trial when new in-vitro evidence showed decreased neutralizing effects against emerging variants.19 Further reflections are needed on how best to evaluate mAbs in the clinical setting during a pandemic to rapidly bring new therapeutic options to patients, while preserving patients’ safety. Novel approaches for evaluating mAbs could be considered, such as immuno-bridging trials where correlates of protection such as humoral/ and or cellular immune parameters are evaluated in a controlled trial to establish whether an intervention is effective,26 and the adoption of a global surveillance system with criteria for in-vitro evaluation of antiviral susceptibility correlated to clinical data.27 Modeling antiviral effects while taking into account vaccination status, SARS-CoV2 antibody levels, infecting viral strains, and other parameters, may also provide better insight into viral efficacy of mAbs, as we have previously shown with remdesivir.28 It remains to better determine which patients would best benefit clinically from an active antiviral therapy in the hospital setting: is it the NP viral load, the time to symptoms onset, the SARS-CoV2 serological status of the patient, the presence of an immunodeficiency, or other factors that should guide clinicians?29
Data Availability
With publication, deidentified, individual participant data that underlie this Article, along with a data dictionary describing variables in the dataset, will be made available to researchers whose proposed purpose of use is approved by the DisCoVeRy Steering Committee. To request the dataset, please address directly to the corresponding author (florence.ader{at}chu-lyon.fr) or to the sponsor's representative (helene.esperou{at}inserm.fr) to obtain a data access form. All requests will be evaluated by the Trial Management Team and the DisCoVeRy Steering Committee. For accepted requests, data will be shared after signing a data transfer agreement with the study sponsor. Data will be shared directly or through access on the INSERM repository. Related documents, such as the study protocol, statistical analysis plan, and informed consent form, will be made available (with publication) on request to the corresponding author or to the sponsor's representative. The data will be open access for the informed consent form, protocol, and statistical analysis plan.
Contributors
FA, MH, CD, NPS, MBD, DC, YY, CB, CM, and FM were involved in the design, establishment, and day-to-day management and implementation of the trial. FA, MH, CD, DC, YY and FM obtained funding for the trial. MH, SJ, FG, FD, JR, NdC, DG, ELL, KL, VT, EF, DM, TS, JC, FCR, AMDR, PL, GMB, CR, KA, VLM, LP, PS, XL, MT, PC, OD, SG, MG, PL, FVB, CV, LB, EBN, AC, AK, FL, ERN, SS, GT, NPS, FA included participants in the trial. MBD, AG, MAT, GD and LJ were responsible for the virological analyses. PP and GC were responsible for the immunological analyses ; IB and SDD were involved in the seroneutralization analyses. ADi, NM, VT were responsible of the safety monitoring and analyses. SCD, ADe, CD, HE, CFL, SlM, AM, and MN were in charge of trial promotion and data monitoring. ST, OK, NB, and BL were responsible for the biobanking. MH, JE, RG, EH, MHa, JAP, AP, JRB, TS, KT, MT, ST, SU, GC, ADi, MBD, HE, DC, YY, FM, and FA were voting members of the trial steering committee. THLH, CM, NB, DB, JG, and FM were involved in the statistical analyses. CM, FM, MH, and FA wrote the original draft of the manuscript, which was reviewed and edited by NPS, NM, AG, PP, GC, JG, and DC. MH, CM, DB, NB, THLH, CD, CFL, ADe, and AM had full access to the blinded data. NB had full access to unblinded data. All authors contributed to refinement of and approved this manuscript. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication
Data sharing
With publication, deidentified, individual participant data that underlie this Article, along with a data dictionary describing variables in the dataset, will be made available to researchers whose proposed purpose of use is approved by the DisCoVeRy Steering Committee. To request the dataset, please address directly to the corresponding author (florence.ader{at}chu-lyon.fr) or to the sponsor’s representative (helene.esperou{at}inserm.fr) to obtain a data access form. All requests will be evaluated by the Trial Management Team and the DisCoVeRy Steering Committee. For accepted requests, data will be shared after signing a data transfer agreement with the study sponsor. Data will be shared directly or through access on the INSERM repository. Related documents, such as the study protocol, statistical analysis plan, and informed consent form, will be made available (with publication) on request to the corresponding author or to the sponsor’s representative. The data will be open access for the informed consent form, protocol, and statistical analysis plan.
Declaration of interests
MH reports grants from The Belgian Center for Knowledge (KCE), the Fonds Erasme-COVID-Université Libre de Bruxelles and the EU-Horizon programme, for the submitted work; and has received support for attending meetings from Pfizer; support for participation on an advisory board for therapeutics on COVID-19; and support for leadership for the Belgian guidelines on therapeutics for COVID-19 and acting as a treasurer for the Belgian Society of Clinical Microbiology and Infectious Diseases. RG reports consulting fees from Celgene, Novartis, Roche, Bristol Myers Squibb, Takeda, Abbvie, AstraZeneca, Janssen, Merck Sharp & Dohme, Merck, Gilead, and Daiichi Sankvo; lecture fees from Celgene, Roche, Merck, Takeda, AstraZeneca, Novartis, Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Sandoz, Abbvie, Gilead, and Daiichi Sankvo; support for attending meetings from Roche, Amgen, Janssen, AstraZeneca, Novartis, Merck Sharp & Dohme, Celgene, Gilead, Bristol Myers Squibb, Abbvie, and Daiichi Sankvo; participation in a Data Safety and Monitoring Board for Celgene, Novartis, Roche, Bristol Myers Squibb, Takeda, Abbvie, AstraZeneca, Janssen, Merck Sharp & Dohme, Merck, Gilead, and Daiichi Sankyo; research grants from Celgene, Roche, Merck, Takeda, AstraZeneca, Novartis, Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Sandoz, Abbvie, Gilead, and Daiichi Sankyo. J-AP reports consulting fees from Pfizer, Merck Sharp & Dohme, and Janssen-Cilag; lecture fees from Pfizer; and support for attending meetings from Pfizer. DC reports grants and lecture fees from Janssen and lecture fees from Gilead, outside the submitted work. CB reports participation in a Data Safety and Monitoring Board for 4Living Biotech; and consulting fees from Da Volterra and Mylan Pharmaceuticals, outside the submitted work.FM reports grants and consulting fees from Da Volterra, grants from Sanofi, and consulting fees from Ipsen, outside the submitted work. All other authors decalre no competing interests
Acknowledgements
This work received funding from several sources: the European Commission (EU-Response, Grant 101015736), the DIM One Health Île-de-France (R20117HD) and Astra-Zeneca. We thank all participants who consented to enroll in the trial, as well as all study and site staff whose indispensable assistance made the conduct of the DisCoVeRy trial possible (all listed in the appendix, pp 27-36)
References



