
ABSTRACT
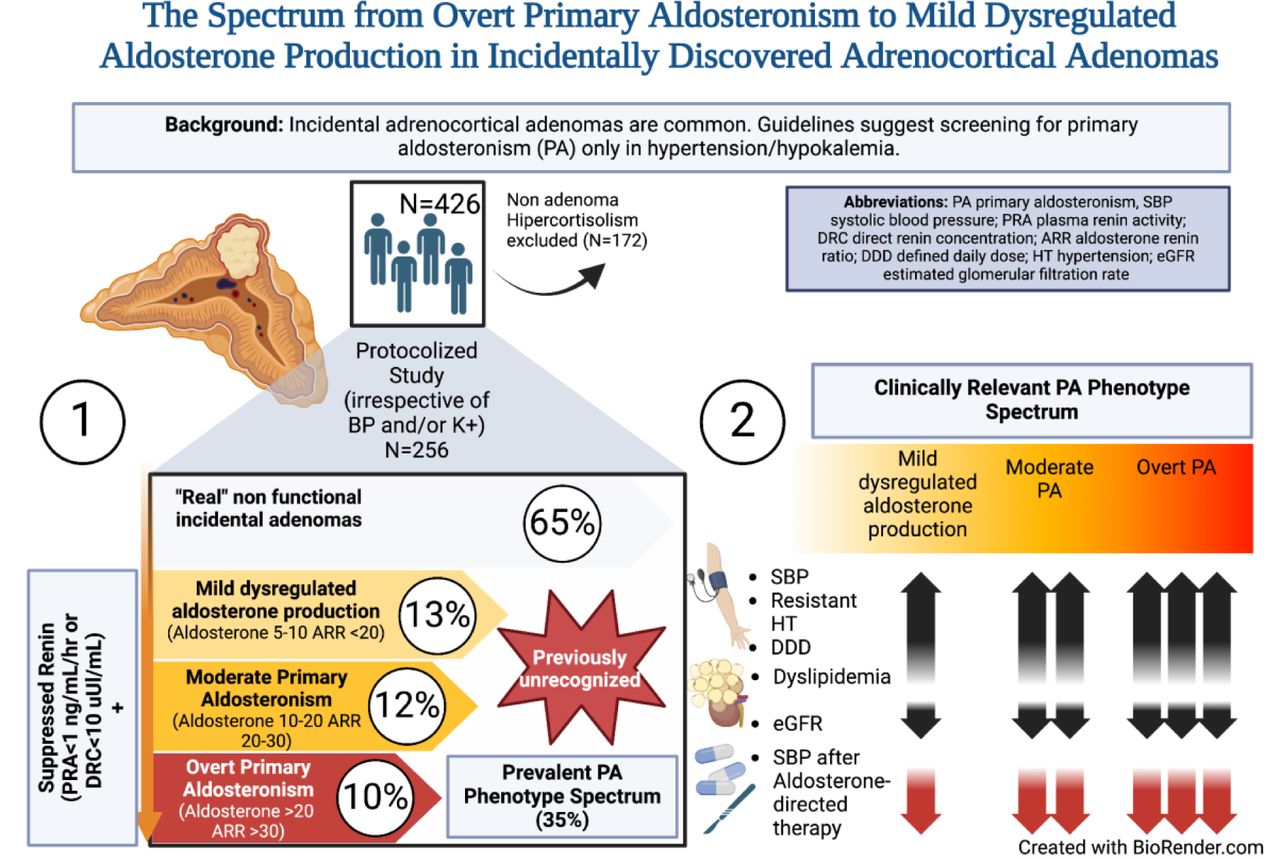
Background Incidental adrenocortical adenomas (IA) are common. Current guidelines suggest screening for primary aldosteronism (PA) only in cases of hypertension or hypokalemia. This study aimed to evaluate the spectrum from overt PA to mild dysregulated aldosterone production with a sensitive protocol irrespective of blood pressure (BP) and potassium in patients with IA.
Methods 254 consecutive patients (excluding hypercortisolism) were evaluated. The spectrum of PA was defined as a suppressed renin plus the following criteria: 1)Overt PA: aldosterone-to-renin-ratio (ARR) >30 ng/dL-to-ng/mL/hr, plasma aldosterone concentration (PAC) >15ng/dL, and/or 24h urinary aldosterone >10 ug/24h; 2)Moderate PA: ARR 20-30 ng/dL-to-ng/mL/hr, PAC 10-15 ng/dL; 3)Mild dysregulated aldosterone production: ARR <20 ng/dL-to-ng/mL/hr and PAC >5-10 ng/dL.
Results 35% (n=89/254) met criteria for PA spectrum, 20% (34/89) were initially normotensive and 94% (84/89) normokalemic. Overt, moderate, and mild groups were 10%, 12%, and 13%. There were trends across groups of clinical severity: systolic BP (153±19, 140±14, 137±14 mmHg, p-trend<0.05), resistant hypertension (50%, 23%, 7% p-trend=<0.001), daily defined dose of antihypertensives (DDD) (3.2±1.6, 1.2±1.5, 0.4±0.6 p-trend=0.001), and lower eGFR (75.5±30.8, 97.8±38.5, 101±25.5, p-trend<0.01). At follow-up (mean 28±15 months), 87% had treatment with MR antagonists or surgery with decreased systolic BP relative to clinical severity, −31.3 ±23, −12.7 ±19, and −11.4 ±19 mmHg, (p-trend<0.001). Similar trends were observed for DDD, with significant increase in renin.
Conclusions There is a prevalent spectrum of clinically-relevant PA and dysregulated aldosterone production in IA, irrespective of BP or potassium, usually undetected. Aldosterone-directed treatment improved BP and normalized renin even in milder cases.

{kind=link}
Competing Interest Statement
The authors have declared no competing interest.
Clinical Trial
We analyzed retrospectively an intervention that was not randomized and treatment decisions were autonomously determined by attending physicians without predefined outcomes as typically seen in prospective studies.
Funding Statement
T. Uslar and R. Baudrand were supported by grant 1190419 from FONDECYT and ACT210039 from Anillo ANID.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
Ethics committee from "Bioética UC" project number 180806018
I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable.
Yes
Data Availability
Data is available if requested and will be provided under restrictions to protect confidential persona information of patients.
Non-standard Abbreviations and Acronyms
- IA
- incidental adrenocortical adenomas
- PA
- primary aldosteronism
- MR
- mineralocorticoid receptor
- CT
- computed tomography
- HU
- Hounsfield units
- MRI
- Magnetic resonance imaging
- PAC
- plasma aldosterone concentration
- PRA
- plasma renin activity
- DRC
- direct renin concentration
- DST
- dexamethasone suppression test
- MACS
- mild autonomous cortisol secretion
- ARR
- aldosterone-to-renin ratio
- DDD
- defined daily dose.



