
Abstract
Background Both dengue and chikungunya are transmitted by Aedes aegypti and have many similarities in epidemiology and clinical manifestations. These two viruses are known to cause asymptomatic infection, however, studies to assess the seroprevalence in healthy individuals are limited. Our objective is to estimate the asymptomatic seroconversion status of both these infections Sri Lanka where dengue has been endemic and the last notable outbreak of chikungunya occurred in 2007.
Methods The study was performed using venous blood samples of 454 healthy individuals (age range 11-78) in Kandy district, who had no known history of dengue or chikungunya infections in the past or present. Samples were tested for dengue NS1 antigen, dengue IgM, dengue IgG, Chikungunya IgM and Chikungunya IgG by using commercially available ELISA kits. Statistical data analysis was performed using SPSS software version 16.0 (SPSS, Inc., Chicago, IL, USA). P value <0.05 was considered statistically significant.
Results Of the 454 healthy individuals, 287 (63.2%) were positive for dengue IgG indicating a past infection and 18 (4%) were positive for dengue-specific IgM. Of the same total, 82 (18.1%) were positive chikungunya chikungunya-specific IgM and only 6 (1.3%) were positive for chikungunya-specific IgM. The number of individuals positive for both dengue IgG and Chikungunya IgG, indicating dual antibody prevalence or exposure to both diseases asymptomatically was 61(13.43%). For dengue specific IgG, the highest sero-conversion rate (80.4%) was observed in 51-60 year age group whilst the lowest (50%) in the age group 11-20. Out of the MOH areas, the highest prevalence (71.4%) of positives were observed in Bambaradeniya and the lowest prevalence (53.1%) in Yatinuwara suburbs in Kandy. The highest percentage of dengue IgM prevalence (6.3%) was observed in the age group 21-30 years and the lowest percentage (1.5%) was observed in the age group 11-20.
Conclusions An asymptomatic seroconversion rate was observed in both dengue and Chikungunya infections. Dengue records a high rate due to its endemicity and periodic outbreaks. It is interesting to note the low-grade prevalence of Chikungunya infection contrary to the belief itsnon-existence in the island currently.
1. Introduction
Sri Lanka is a tropical country having favorable environmental conditions for vector-borne infections. Dengue and chikungunya are two such infections in Sri Lanka. Both these diseases share many similarities in terms of epidemiology and clinical manifestations (Furuya-Kanamori et al., 2016). Dengue is endemic on the island where the last two decades witnessed increased disease burden and severity leading to significant morbidity and mortality (Senaratne and Noordeen, 2014). However, the last outbreak of chikungunya occurred in 2006-07 without apperen endemicity (Wijesinghe et al., 2009).
Dengue
Dengue is a single-stranded icosahedral-enveloped RNA virus belonging to the Flaviviridae family and genus Flavivirus. It exists as four closely related antigenically distinct serotypes - DENV-1, DENV-2, DENV-3, and DENV-4 (Balmaseda et al., 2006). The infection is transmitted by infected female Aedes mosquitos. Abrupt onset of high fever, headache, myalgia and backache are the common symptoms (Kalayanarooj, 2011). Most of the patients have uncomplicated clinical course categorized as dengue fever (DF), but some patients develop dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) characterized by increased vascular permeability, plasma leakage, hemorrhage, and multiple organ dysfunction. Pathogenesis of DHF is due to the loss of capillary endothelial integrity as a result of an abnormal immune response and a disturbance in immune regulation (Wagenaar, Mairuhu and van Gorp, 2004). Thrombocytopenia and leucopenia are characteristic haematological manifestations in dengue infection (De Azeredo, Monteiro and De-Oliveira Pinto, 2015). The prediction of progression to DHF is difficult but factors such as serotype/ genotype of the virus, previous exposure to dengue virus, and the age of the patient are postulated (Tissera et al., 2016). The diagnosis of dengue infection is best done by detection of viral nucleic acid with real time quantitative reverse transcriptase PCR, virus isolation in cell culture, NS1 antigen detection, and/ or detection of virus-specific antibodies in paired sera like IgM, IgG detection through ELISA and neutralization tests (Ku et al., 2016).
There is a global increase of the incidence of dengue over the last decades. A recent estimate indicated about 390 million dengue infections occurring annually in the world with 96 million clinical cases (Who.int, 2018). A systematic review covering 1990-2015 showed that the outbreaks virtually occurring in tropical and subtropical regions in particular India, China, and Brazil (Zhou et al., 2017). In Sri Lanka, dengue had been reported since 1960 and ensuing years showed regular incidence of DF/DHF throughout the year with outbreaks during the rainy seasons (Kularatne, Gawarammana and Kumarasiri, 2005,P.D.N.N. Sirisena and Noordeen, 2014, Wijewickrama et al., 2018). Sri Lanka had experienced a major outbreak in 2017 due to the shift of DENV serotype 1 to serotype 2, with 186101 hospitalized cases (Wijewickrama et al., 2018).
Chikungunya
Chikungunya is an alphavirus of the family Toga viridae which contains single-stranded RNA and is transmitted by the female Aedes mosquito. Clinical manifestations of the disease includes sudden onset of fever with chills, headache, vomiting, malaise, myalgia, arthralgia or arthritis (Razmy, 2014a). Ocular manifestations such as anterior uveitis and retinitis were reported (Mahendradas, 2016). Most of the clinical and laboratory investigations of chikungunya infection are similar to dengue infection and arthritis is characteristic (Kularatne et al., 2009). It has been identified that the life cycle of this virus belongs to two primary transmission cycles. In Asia, it is mainly the mosquito-human-mosquito with Aedes aegypti being the primary transmission vector whereas in Africa, it is mainly the sylvatic cycle including non-human primates (Pulmanausahakul et al., 2011). For diagnosis, virus detection, serological tests and molecular techniques are used (Mahendradas, Avadhani and Shetty, 2013). During the initial viremic phase, virus isolation and the real time polymerase chain reaction (RT-PCR) are useful in identification of the illness. During the later phase of the disease detection of antibodies through serological assays would be useful (Mahendradas, 2016).
According to the geographical distribution over the years, there are 3 distinct Chikungunya virus genotypes recognised-West African, East Central South African and Asian. In 1958, the Asian strain was identified in Thailand transmitted by the suspected vector (Mowatt and Jackson, 2014). Since then Chikungunya had been circulating sporadically in South East Asian countries and transmission to humans by A. aegypti was documented in 2006 during the outbreak in Malaysia (Mowatt and Jackson, 2014). Massive outbreaks of Chikungunya had been reported in India in 2005 and the re-emergence of this virus was confirmed in 2006 after four decades of absence (Hapuarachchi et al., 2010). In Sri Lanka an outbreak of this disease was recognized in 2006 in parallel with Malaysia, Andaman and Nicobar Islands. During 2006-2007, more than 100 000 cases had been reported in Sri Lanka (Razmy, 2014b).
Since both these pathogens are transmitted by Aedes mosquito, it is reasonable to expect similarities of epidemiology of two diseases (Furuya-Kanamori et al., 2016). Due to overlap of clinical picture of both infection, misdiagnosis can lead unexpected outcomes (Furuya-Kanamori et al., 2016). Apart from clinical infection, asymptomatic seroconversion is known to occur in these infections in endemic situations. However, there is paucity of literature on asymptomatic seroconversion and thus seroprevalence. Such knowledge is important to predict epidemics and the disease severity. The aim of this study is to estimates the asymptomatic seroconversion rates of these two infections during years of dengue outbreak.
2. Materials and Methods
Sample selection
In this study venous blood samples were collected from 454 healthy individuals of age ranging from 11 to 78 years from Kandy District, Sri Lanka where 2017 experienced major outbreak of dengue, between the period of 14th January, 2018 to 17th June, 2018. It was confirmed that the study subjects did not have any known history of dengue or Chikungunya fever in the past history through an interviewer-based questionnaire. Investigators perused all medical records of the subjects and encouraged them to recall call febrile illness in the past.
Sample collection
4mL of venous blood was collected from healthy participants into K2EDTA tubes. Samples were transported from the site of collection to the laboratory in a cool box maintaining the cold temperature. Then the total WBC count, differential WBC count (WBC/DC), PCV, estimated hemoglobin and total plasma protein were measured from whole blood before centrifugation. Samples were then centrifuged at 1500 rpm for 5 minutes at 5°C. The separated plasma was then stored at −20°C until the serological tests were performed.
Ethics statement
Ethical clearance for this project was obtained from the Institutional Ethical Review Committee, Faculty of Medicine, University of Peradeniya. Written consent was obtained from each participant before obtaining the blood samples along with a questionnaire. Age, gender, residence and records of past infection with dengue or Chikungunya were taken into consideration for this study.
Blood parameters
Whole blood was diluted 1: 20 in WBC diluting fluid and the WBC counts were taken by using the hemocytometer according to the standard protocols. Differential count of WBC was done manually by a Leishmann’s stained blood smear. The PCV was calculated by hematocrit method. Estimated hemoglobin concentration was obtained by using the hematocrit value. Total plasma protein was measured by using refractometer.
Serological tests
The pre-separated plasma samples were tested for Dengue NS1 antigen, Dengue IgM, Dengue IgG, Chikungunya IgM and Chikungunya IgG by using commercially available EUROIMMUN Medizinische Labor diagnostika AG ELISA kit for Dengue NS1 antigen, Dengue IgM, Dengue IgG, ChikungunyaIgM and Chikungunya IgG.
Data Analysis
Statistical Analysis of data was performed by using SPSS software version 16.0 (SPSS, Inc., Chicago, IL, USA). P value <0.05 was considered statistically significant.
3. Results
Demographic data
Among the 454 healthy subjects, 267 (58.8%) were males and 187 (41.2%) were females. Of them, 68 (15%) belonged to the age group of 11-20, 127 (28%) in 21-30, 115 (25.3%) in 31-40, 70 (15.4%) in 41-50, 51 (11.2%), and 23 (5.1%) in the age group of more than 61 years. The Medical Officer of Health (MOH) divisions of Kandy district where they resided were 35 (7.7%)-Bambaradeniya, 129 (28.4%)-Gangawatakorale, 82 (18.1%)-Udunuwara, 38 (8.4%)-Werellagama, 111 (24.4%)-Yatinuwara and the rest 59 (13%) belonged into other MOH areas including Akurana, Doluwa, Galagedara, Galaha, Gampola, Hatharaliyadda, Kundasale, Menikhinna, and Waththegama.
Blood Parameters
To assess the general heath of the subjects WBC/DC, total plasma protein, PCV and haemoglobin were tested for all the participants and also to exclude any infection at the time when the samples collection. Accordingly, the mean values of these blood parameters were calculated. The results indicated that the mean values are within the normal range in every parameter checked (Table 1).
Dengue Specific IgG results
Among the 454 healthy individuals, 287 (63.2%) were positive for Dengue IgG indicating the past infection and 12 (2.6%) showed borderline results as per manufacturer’s instructions. Table 2 shows the prevalence of Dengue IgG among gender groups, age categories and the MOH areas of Kandy district. In the age groups, the highest sero-conversion rate (80.4%) was observed in 51-60 year whilst lowest (50%) in the age group 11-20. Out of the MOH areas, highest prevalence (71.4%) of positives were observed in Bambaradeniya and the lowest prevalence (53.1%) in Yatinuwara. There was no much difference observed between the males and females. (Males: 62.9% and females: 63.6%).

The bar chart indicates the positive percentages (y-axis) relative to the Dengue serological parameters; Dengue NS1 antigen, Dengue IgM antibody and Dengue IgG antibody (x-axis).

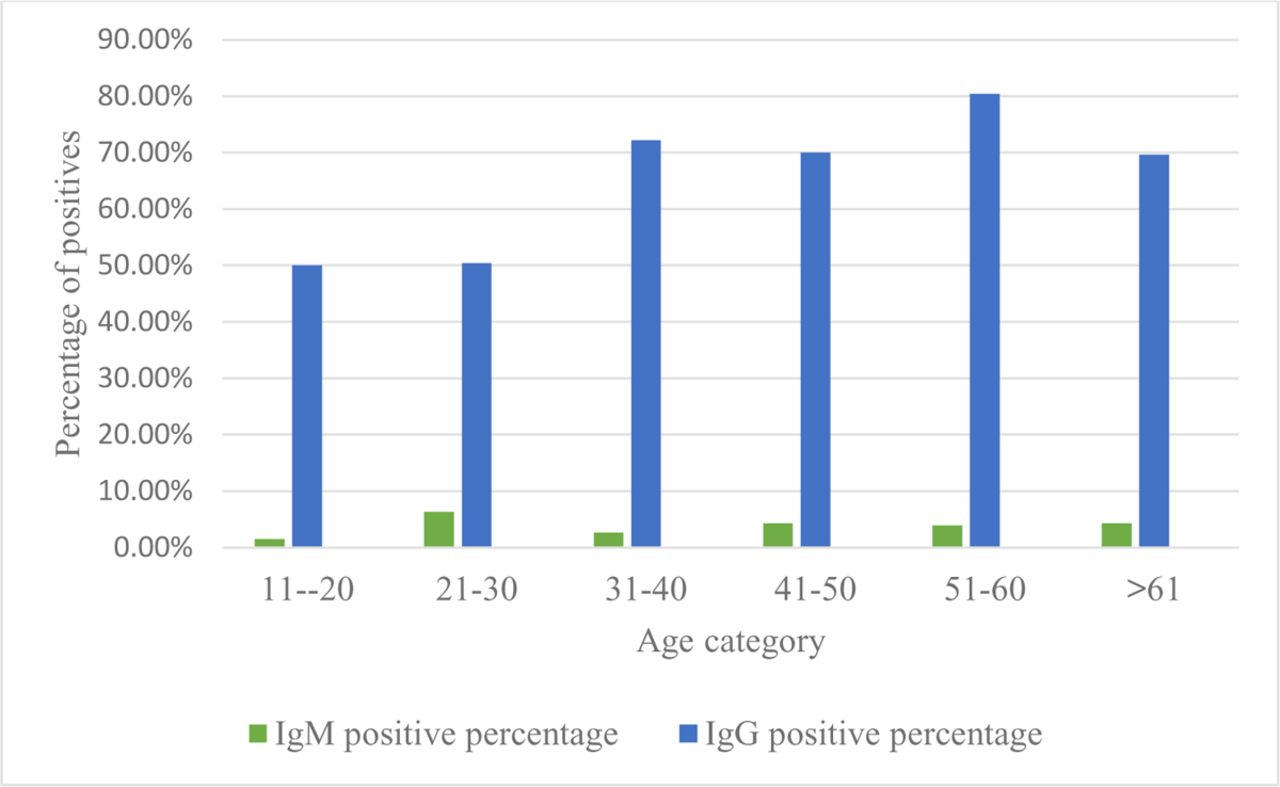
The bar chart represents the positive percentages (y-axis) of Dengue IgM and Dengue IgG antibodies relative to the age categories (x-axis).

The bar chart represents the positive percentages of Dengue IgM and IgG antibodies (y-axis) relative to the MOH areas in Kandy district (x-axis)
Dengue Specific IgM results
Out of the 454 individuals, 18 (4%) were positive for Dengue specific IgM and 19 (4.2%) indicated borderline results as per manufacturer’s instructions. According to the age categories the highest percentage of Dengue IgM prevalence (6.3%) was observed in the age group 21-30 and the lowest percentage (1.5%) was observed in the age group 11-20. The highest percentage of IgM prevalence was observed in Werellagama (7.9%) and no one was positive for Dengue IgM in Bambaradeniya. As observed in Dengue IgG prevalence, there was no significant difference of Dengue IgM prevalence with gender (Females: 5.3% and Males 3.0%). The percentages of Dengue IgM categorized according to gender, age groups and MOH areas in Kandy district are indicated in Table 2.
Chikungunya Specific IgG results
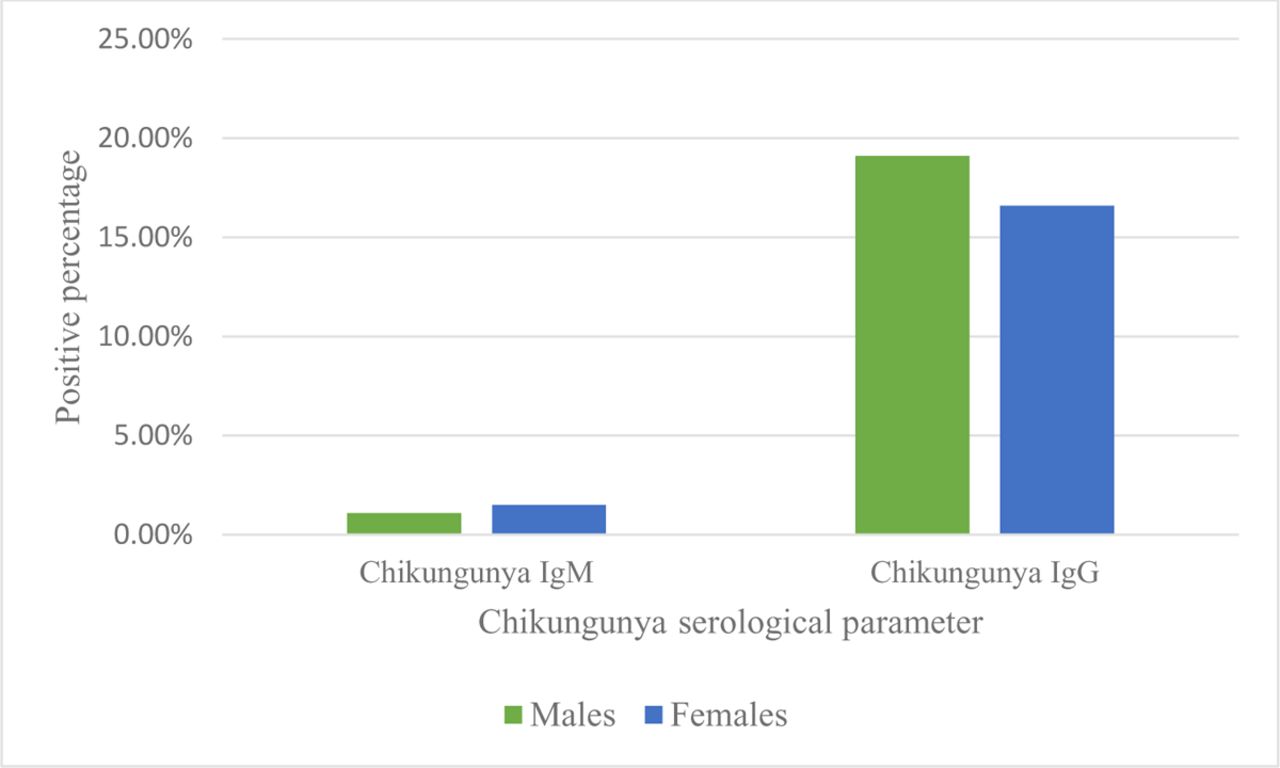
Out of the 454 individuals, 82 (18.1%) were positive and 12 (2.6%) participants showed borderline results. When considering the age categories, the highest positive percentage was shown in the age group >60 which was 26.1%. The lowest percentage was in the age group 51-60 and it was 5.9%. Gangawatakorale MOH area showed the highest percentage (24%) of Chikungunya IgG prevalence and Udunuwara had the lowest exposure (12.2%). There was no significant difference between males and females in IgG prevalence (Females: 16.6% and Males: 19.1%) The percentages of Chikungunya IgG with respect to gender, age and the MOH areas of Kandy district are indicated in Table 3.

The bar chart indicates the positive percentages of males and females (y-axis) relative to Chikungunya IgM and IgG antibodies (x-axis).

The bar chart indicates the positive percentages of Chikungunya IgM and IgG antibodies (Y-axis), relative to the age categories (x-axis).

The bar chart represents the positive percentages of Chikungunya IgM and IgG antibodies (y-axis) related to the MOH areas in Kandy (x-axis).
Chikungunya Specific IgM results
In the ELISA performed for the detection of Chikungunya IgM for the participants of this study 6 indicated positive and 10 indicated the borderline results (Table 1.2). The positives of this test were in between the age range of 11-40 and the highest number of them (4/6) were from Gangawatakorale MOH area. Table 3 indicates this data in detail.
Prevalence of anti-CHIKV and anti-DENV antibodies together
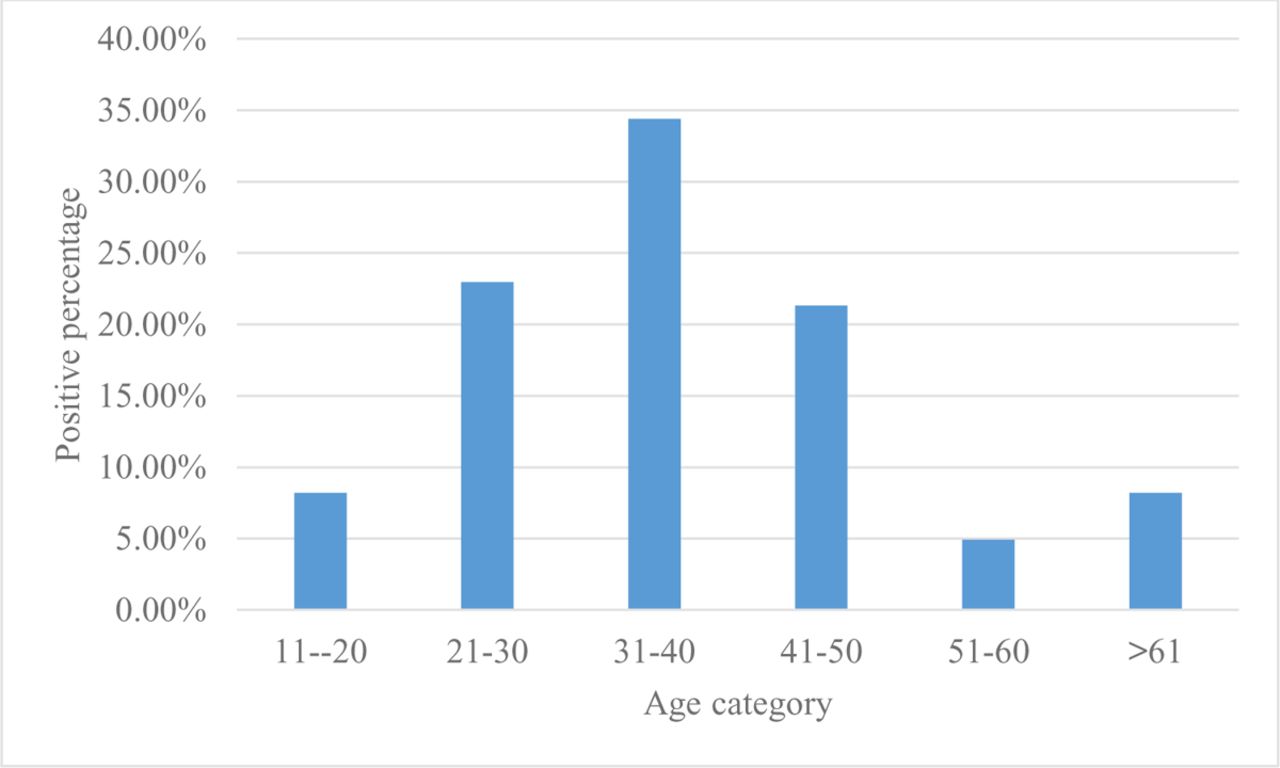
From the data obtained on the prevalence of Dengue and Chikungunya antibodies, percentages of dual antibody prevalence were calculated in order to determine the exposure to both diseases. None of the participants were positive for IgM antibodies together. However, of the 454 individuals, 61(13.43%) were positive for both Dengue IgG and Chikungunya IgG. The highest percentage of this dual positiveness in IgG was observed in the age group 31-40 which is 34.42% (21/61) and the lowest percentage was in the two ends of the age categorization which are 11-20 and >61 age groups (8.19%). When considering the MOH areas, Gangawatakorale showed the highest percentage (36.06%). Among the 287 Dengue IgG positive individuals, 21.25% were positive to Chikungunya (61/287) and in contrast, from the 82 individuals who were positive to Chikungunya, 74.39% were positive to Dengue (61/82). Table 4 indicates further details on evidence of dual anti-DENV and anti-CHIKV antibody prevalence according to gender, age group and MOH areas in Kandy district.

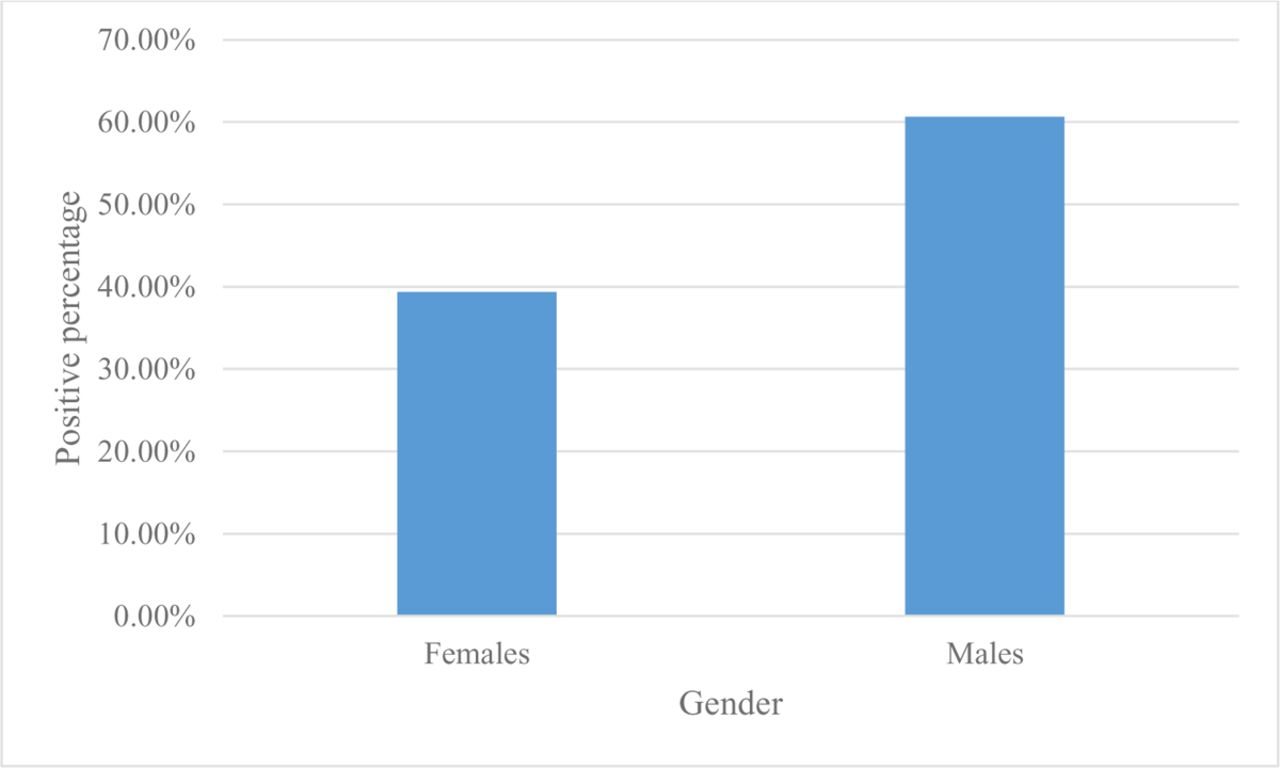
The bar chart represents the positive percentages of both the Chikungunya and Dengue IgG antibodies (y-axis) relative to the gender (x-axis).

The bar chart represents the positive percentages of both the Chikungunya and Dengue IgG antibodies (y-axis) relative to the age categories (x-axis).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The bar chart represents the positive percentages of both the Chikungunya and Dengue IgG antibodies (y-axis) relative to the MOH areas in Kandy district (x-axis).
4. Discussion
We recruited 454 healthy individuals of Kandy district, Sri Lanka who did not have any history of hospitalization due to dengue and Chikungunya or any other infection before our study. We found 63.2% of the healthy individuals were seropositive for dengue IgG which indicates past asymptomatic exposure to dengue virus and 4.0% were seropositive for dengue IgM antibodies indicating recent asymptomatic exposure. Similarly, it was revealed that among the participants 18.1% were positive for Chikungunya IgG indicating the past exposure to the virus and only 1.3% were positive for Chikungunya IgM indicating recent exposure.
Dengue and Chikungunya have caused a significant public heath impact globally, including Sri Lanka. When considering the environment associated risk factors for occurrence of these two diseases, presence of suitable breeding sites for the primary vector, Aedes aegypti, within perimeters of residential areas had an association with dengue seropositivity. High vegetation density, elevation above sea level and presence of animals have been associated with Chikungunya seropositivity (Kajeguka et al., 2017). Sri Lanka being a tropical country, has a favorable environment for both these diseases. In order to predict the disease severity and the future outbreaks, seroprevalence studies are important. Although there is adequate information about the patients who had been hospitalized due to dengue and Chikungunya infections, limited amount of data is available on the seroprevalence of these diseases in the healthy individuals. It would be useful in planning the control strategies in advance.
All four serotypes of dengue have been circulating in Sri Lanka for several decades. In 2006, 2009 and 2010 dengue serotype 1 had been responsible for outbreaks of DF/DHF in Sri Lanka (P. D.N.N. Sirisena and Noordeen, 2014). But in 2017 a huge outbreak of Dengue occurred in Sri Lanka due to shifting serotype of the dengue virus from serotype 1 to 2 (Dengue et al., 2018). Since the samples for our study were collected in 2018, after the outbreak of 2017, there is a possibility that active transmission of serotype 2 as suggested by positives Dengue IgM. However negative Dengue NS1 in all sample exclude active disease. A study done in Colombo district in Sri Lanka in a randomly selected children of less than 12 years revealed that 52% of the study cohort was positive for Dengue IgG (Tissera et al., 2010). This result is comparable our finding that 50% of the individuals were in the age group of 11-20 years. The seroconversion rate of 80.4% is highest in the age group of 51-60 having high risk of secondary dengue infection, however, does it happen clinically is doubtful. In secondary dengue infection the virus bound immune complexes are recognized by the Fcɣ receptors which facilitate the virus entry and replication in the target immune cells (Katzelnick et al., 2017). Among the MOH areas of Kandy district, Bambaradeniya MOH area had the highest percentage of Dengue IgG prevalence. But in contrast this area did not have anyone positive for Dengue IgM probably due to cessation of active transmission.
Compared to Dengue IgG prevalence, Chikungunya IgG prevalence is significantly low. Similar pattern is observed in between the IgM antibodies of both the diseases as well. Unlike Dengue, in Chikungunya reinfection is unlikely due to lifelong immunity (LAOPRASOPWATTANA et al., 2016). A previous study in Sri Lanka to study prevalence of Chikungunya during a Dengue outbreak in 2006 revealed absence of Chikungunya antibodies in Kandy district (Wijesinghe et al., 2009). However, we found seroconversion against Chikungunya with IgM and IgG antibodies highest in Gangawatakorale MOH area. This area is more urban and suggests presence of high density of infected mosquitos. After the outbreak of Chikungunya in the Central province of Sri Lanka in 2006, a study had been conducted in a hamlet belonging to Kandy district of the same province. During this study it had been revealed that 51% of the people had symptomatic Chikungunya and the peak incidence observed in the age group 40-50 years (Abeyrathna et al., 2012).
Several seroprevalence studies of both infections had been done in many countries in healthy individuals. However, comparison is difficult due to the differences of the age groups, study population, method of antibody detection and many other reasons. However, in Singapore, among the residents of age 18-79 years, the seroprevalence rate of Chikungunya antibodies were 1.9% which is much less than that of the current study which indicated 18.1% positivity for Chikungunya IgG antibodies. In the same study highest seroprevalence was observed in the elderly of age group between 70-79 years and significant difference had been observed in between males and females (Ang et al., 2017). In Thailand, among the individuals of age ranging from 6 months to 60 years, 26.8% were seropositive for CHIKV, 79.2% were seropositive for DENV and 24.4% had shown dual positivity to both antibodies. In the same study, seroprevalence of DENV antibodies were three times that of Chikungunya which agrees with the current study (Vongpunsawad et al., 2017). In Pakistan (District Lahore), 2012, seroprevalence of Dengue in healthy individuals of age above 15 years was 67.2% in 2012 (Hafeez et al., 2017). A study done using the residents of Qatar, it had been revealing that Asian Nationals had higher adjusted odds of being seropositive for anti-DENV and anti-CHIKV antibodies compared to nationals of Middle East, North Africa and Qatar. This study has also shown that anti-DENV antibody seropositive rate was higher among the anti-CHIKV antibody seropositive individuals comparable with the present study in Sri Lanka, suggesting co-circulation of these viruses (Humphrey et al., 2019).
Including Sri Lanka (Kularatne, 2009), evidence of dengue and Chikungunya co-infection have been found in many countries like Angola, Gabon, India, Madagascar, Malaysia, Myanmar, Nigeria, Saint Martin, Singapore, Tanzania, Thailand and Yemen (Furuya-Kanamori et al., 2016). In Sri Lanka, the first case report of both Dengue and Chikungunya co-infection confirmed with molecular assays was reported in 2006 and during 2006-2007, 3 cases had been reported in Kandy-Sri Lanka.(Hapaurachchi et al., 2008)(Kularatne et al 2009). When considering globally, data on co-infection of these diseases is relatively low. However according to some comparative studies performed to check biological and clinical symptoms between mono infected and dual infected patients, no severe manifestations had been observed in mixed infections (Kularatne, 2009). This suggests that the two viruses do not exert additive effects (Hapaurachchi et al., 2008). In the current study, seroprevalence of dual antibodies for anti-DENV and anti-CHIKV was calculated. The calculated percentage of the dual antibody prevalence was less than that of a similar study performed in Thailand (Vongpunsawad et al., 2017). The current study also has revealed that 21.25% of the Dengue IgG positive healthy individuals are positive for Chikungunya IgG and 74.39% of Chikungunya IgG positive healthy individuals were positive for Dengue IgG. According to these results, it can be expected that there can be a relationship between Chikungunya and Dengue virus antibodies where exposure to Chikungunya makes it more vulnerable to Dengue but the vice versa is not.
Having accurate and reliable seroprevalence data would be much useful in predicting the disease burden and for the public health implications. In case of Dengue, it is much complicated due to four serotypes and reinfection involving different serotype cause DHF due to Antibody Dependent Enhancement (ADE)” (Flipse et al., 2016). Therefore, the current study is much useful in assessing the risk of severe dengue outbreak. On the contrary Chikungunya has one serotype giving immunity against future infections. However, renewing the population with added new generations, outbreak can be predicted due to its asymptomatic endemicity.
Data Availability
All data produced in the present work are contained in the manuscript
Abbreviations
- K2EDTA-Di
- Potassium Ethylene Diammine Tetra Aciticacid.
- DF
- Dengue fever
- DSS
- Dengue Shock Syndrome
- DHF
- Dengue Hemorrhagic fever
- WBC
- White Blood Cells
- PCV
- Packed Cell Volume
- PCR
- Polymerase Chain Reaction
- WBC
- White Blood Cells
- DC
- Differential Count
- RT-PCR
- Real time polymerase chain reaction
- CHIKV
- Chikungunya virus
- DENV
- Dengue virus
- MOH
- medical Officer of Health Author contribution
RPVJR and SAMK did conceptualization and LEADAE and TNAM collected data. LEADAE,SAMK and SAMDA analyzed the data and drafted the paper. All authors did intellectual contribution and involved in final version of the manuscript.
References



