
Abstract
Background Maternal nutritional interventions aim to address nutrient deficiencies and improve maternal, fetal, and pregnancy outcomes. However, the effects of these interventions on the placenta are not well known, which is a major gap in understanding how such interventions could influence pregnancy outcomes and fetal health. We hypothesised that nutritional interventions influence placental phenotype, and that these placental changes relate to how successful, or not, the intervention is in improving pregnancy outcomes.
Methods We conducted a systematic review and followed PRISMA-2020 reporting guidelines. Articles were retrieved from PubMed, Clinicaltrials.gov, and ICTRP-WHO using pre-defined search terms and screened by two reviewers using a 3-level process. Inclusion criteria considered articles published from January 2001-September 2021 that reported on clinical trials in humans, which administered a maternal nutritional intervention during the periconceptional or pregnancy period and reported on placental phenotype (histomorphometry, function or placental disorders).
Findings Fifty-three eligible articles reported on (multiple) micronutrient- (n=33 studies), lipid- (n=11), protein- (n=2), and diet-/lifestyle-based (n=8) interventions. Of the micronutrient-based interventions, 16 (48%) associated with altered placental function, namely altered nutrient transport/metabolism (n=9). Nine (82%) of the lipid-based interventions associated with altered placental phenotype, including elevated placental fatty acid levels (n=5), altered nutrient transport/metabolism gene expression (n=4), and decreased inflammatory biomarkers (n=2). Of the protein-based interventions, two (66%) associated with altered placental phenotype, including increased cerebro-placental ratio (n=1) or decreased preeclampsia risk (n=1). Three (38%) of diet and lifestyle-based interventions associated with altered placental phenotype, namely placental gene expression (n=1) and disease (n=2). In studies with data on maternal (n=30) or offspring (n=20) outcomes, interventions that influenced placental phenotype were more likely to have also associated with improved maternal outcomes (11/16 [69%]) and offspring birth outcomes (6/11 [54%]), compared to interventions that did not associate with placental changes (2/15 [13%] and 1/9 [11%], respectively).
Conclusions Periconceptional and prenatal nutritional interventions to improve maternal/pregnancy health associate with altered placental development and function. These placental adaptations likely benefit the pregnancy and improve offspring outcomes. Understanding the placenta’s role in the success of interventions to combat nutrient deficiencies is critical for improving interventions and reducing maternal and neonatal morbidity and mortality globally.
Introduction
Maternal and child undernutrition are associated with approximately 50% of global deaths under the age of 5 [1]. Pre-existing maternal nutrient deficiencies can be amplified during pregnancy, specifically, as nutritional demands increase to support the health of the mother and the developing fetus [1, 2]. The periconceptional and perinatal periods represent critical windows of offspring development, and nutritional inadequacy or insufficiency during these periods not only associates with immediate adverse outcomes (including an increased risk of poor fetal growth, stunting, preterm birth, and mortality [2, 3]), but also programmes poorer health trajectories in offspring and increases their disease risk later in life [4]. For mothers, a suboptimal nutritional status during the periconceptional and perinatal periods can associate with an increased risk of anaemia, hypertension, miscarriage, or mortality [5]. Common nutritional interventions targeted to improve maternal nutrient status and maternal/pregnancy outcomes have included daily supplementation with folic acid [6], with and without iron, multiple micronutrients, and/or calcium supplementation [7]. However, the success of these interventions in improving pregnancy outcomes has been inconsistent [2, 8], in part because the biological mechanisms that determine an intervention’s impact are complex and remain poorly understood.
The placenta is an underappreciated mediator of a nutritional intervention’s impact on maternal, fetal, and infant health outcomes. A critical organ in pregnancy that develops alongside the embryo/fetus, the placenta plays a vital role in fetal development by facilitating nutrient (glucose, amino acids, lipids, and vitamins and minerals [9, 10]) and gas transport, waste removal, and fetal protection from xenobiotics [9]. Placental nutrient transport is influenced by nutrient availability and fetal nutrient requirements [11], among other factors, and can adapt to buffer against temporary fluctuations in maternal nutrient status (both deficiencies and oversupply) to maintain a consistent nutritional environment for the developing fetus [9]. Importantly, the placenta itself also relies on adequate nutritional resources to develop and function properly, and inadequate resources may disrupt optimal placental development and function [12]. A healthy placenta also benefits maternal health, including through the release of placental hormones, which can alter maternal physiology in preparation for pregnancy and lactation [13]. Thus, it is plausible that nutritional interventions to improve maternal and fetal health may be associated with changes in the placenta, and understanding these changes may be important for determining why a nutritional intervention is successful in achieving its intended effects in some contexts, but not others.
To-date, evidence in reviews of how nutritional interventions influence the placenta have focused on placental-related pregnancy complications (such as specific conditions like preeclampsia [14-17]), rather than evaluating the effects of interventions on overall placental phenotype. Here, we performed a systematic review to synthesise existing knowledge on how direct maternal nutritional interventions in the periconceptional or pregnancy periods impact placental phenotype. We also aimed to determine whether 1. improved maternal and offspring outcomes were more likely to occur in nutritional interventions that reported placental phenotype alterations, and 2. associations between nutritional interventions and placental phenotype differ based on placental sex or study location. We hypothesised that direct maternal nutritional interventions in the periconceptional and prenatal periods would associate with altered placental phenotype, and that nutritional interventions that improved maternal and offspring health would be more likely to associate with beneficial placental adaptations, than interventions with no improvements on maternal/offspring outcomes.
Methods
Reporting guidelines
This study adhered to current Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-2020)[18] (Figure 1) and Synthesis without meta-analysis (SWiM) [19] frameworks (Supplementary Table S1).

Inclusion and exclusion criteria
Eligible study designs included randomised and non-randomised controlled trials in human populations that administered a direct nutritional intervention to the mother during the pre-conception, periconceptional, or pregnancy periods. Inclusion criteria also required that studies were written in English and published between January 2001 and September 2021 (time of search) to increase the translatability of the review findings to the current day context.
The population of interest was pregnant people receiving a direct nutritional intervention before or during pregnancy (Supplementary Figure S1). Interventions were considered direct if they were nutrition-specific and administered directly to the mother (vs. an indirect nutritional intervention, which may seek to address the underlying drivers of undernutrition, and may target household income/food security, health services, water, sanitation, and food production) [20]. Studies were required to have included a comparison group that served as a control, and some measure of placental phenotype as an outcome (but not necessarily the primary outcome of that study; Supplementary Figure S1). Placental outcomes were categorized into the following five groups: anthropometry (any physical characteristics related to the placenta), molecular (any alterations to placental genotype and/or gene expression, or other molecular changes), pathology (any findings related to placental histopathology), placental abruption (cases of placental abruption), and placenta-related disease (any disease with placental origins, or that significantly impacts the placenta; Supplementary Table S2).
Information sources and search terms
PubMed, ClinicalTrials.gov, and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) were searched to identify peer-reviewed publications using the following search string: ((nutr* OR diet* OR supplement* OR vitamin OR folate* OR folic acid OR mineral OR (micronutri* AND (intervention OR supplement*))) AND (placenta* OR preeclampsia) AND (maternal OR pregnan* OR gravid* OR conception* OR preconceptional OR gestation*)). When searching the listed databases, the filters “Clinical Study, Clinical Trial, Comparative Study, Controlled Clinical Trial, Journal Article, Humans” were applied.
Article search, screening, and data collection
A three-level screening process was performed by two authors (VB and MW; Figure 1). A total of 5299 titles from PubMed (n=5078), ClinicalTrials.gov (n=156), and WHO ICTRP (n=65) were captured from the article search. Articles were excluded for deduplication (n=14), publication date before 2001 (n=8), and incorrect study type (n=10), leaving 5267 articles to be screened at level one (title screening). Clinical trial titles from ClinicalTrials.gov and WHO ICTRP, and article titles from PubMed search results were screened for relevance to our review objectives. In total, 4568 titles were excluded for having a topic not relevant to this review, leaving a total of 699 article abstracts and clinical trials documents to be screened at level two.
At screening level two, 699 article abstracts (PubMed: n=608) and clinical trial records (ClinicalTrials.gov: n=60, WHO ICTRP: n=31) were reviewed to determine their adherence to the inclusion criteria (Figure 1). Articles and trials were excluded for: not reporting on a direct maternal nutritional intervention (n=323), reporting on an animal study (n=12), incorrect type of article (i.e., review, study protocol, or commentary; n=169), no results posted (n=29), or not written in English (n=2), leaving 164 records (PubMed articles: n=129, ClinicalTrials.gov: n=17, WHO ICTRP: n=18) to be carried forward to level three screening.
At level three, full texts were unavailable for seven of 129 PubMed articles. The corresponding authors were contacted by email twice between December 2021 and January 2022 for each of these seven articles, but only one response was received. Publications resulting from the clinical trials retained for screening at level three were obtained from the trial webpage directly, or from searching the trial name and/or number using search browsers (e.g., Google Scholar). Ultimately, 158 full texts were reviewed to evaluate whether studies met the full inclusion criteria (from PubMed, n=123; ClinicalTrials.gov, n=17, and WHO ICTRP, n=18; Figure 1). At level three, articles were excluded for not including a placental measure (n=64; including articles reporting on relationships between a nutritional intervention and risk of preeclampsia that did not provide placenta-specific measures), not administering a direct nutritional intervention (n=9), duplicates (n=11), or other reasons (i.e., wrong study type, no trial results available or could not be found (n=21). In total, 53 articles met the full inclusion criteria.
Data were extracted from each of the 53 included articles, including population data (such as study location [which we used to identify socioeconomic status based on four World Bank classifications: low-income (LIC), low-middle income (LMIC), upper-middle income (UMIC), and high-income (HIC)] [21]), maternal clinical characteristics and demographics, type of pregnancy (singleton or twin), and nutritional intervention details (type [micronutrient, lipid, protein, and/or diet- or lifestyle-based], composition, timing, dose, and compliance data). Data on maternal comorbidities (defined in this study as conditions or states of health during pregnancy that may be harmful to the health of the mother and/or fetus) reported in the studies under review were noted and used to inform results interpretations. Reported adverse outcomes were noted and classified into two categories: adverse effects (outcomes that were suspected to be in response to the intervention [22]) and adverse events (outcomes that were not suspected to be in response to the intervention [22]). Data on associations between the nutritional intervention and 1. placental phenotype (primary outcome), and 2. placental sex, and 3. fetal/infant and maternal outcomes (secondary outcomes) were also captured.
Risk of bias assessments
The 53 articles under review were assessed for risk of bias (RoB) using the Cochrane Collaboration’s Tool for Assessing Risk of Bias [23] (Supplementary Table S3). The RoB assessment criteria were set a priori. As our outcome of interest was placental phenotype, which was often not the primary outcome of the studies under review, assessments for risk of bias due to “incomplete outcome data” considered (when applicable) how the subset of the original cohort with placental data was selected or determined. We also assessed potential bias related to compliance to the intervention, as follows: articles that clearly measured and reported participant compliance were assessed as low risk, articles that did not report clear methods to measure compliance, but had frequent follow up visits with participants, were assessed as unclear risk, and articles that did not measure compliance and had few participant follow up visits (e.g., only at intervention onset and delivery) were assessed as high risk. RoB assessments were performed independently by two authors (VB and MW). Discrepancies in RoB assessments were resolved through discussion with a third author (KLC). While RoB in interventions was not a primary outcome of this review, assessments of RoB were performed to inform results interpretations.
Data synthesis and visualisation
Graphical Overview for Evidence Reviews (GOfER [24]) figures were created for each type of nutritional intervention to visualise key study data. The GOfER included intervention composition and timing, reported alterations to placental phenotype, and reported maternal and fetal outcomes (both beneficial and adverse). A filled map was created to demonstrate the locations of the studies included (Microsoft Excel v16). Alluvial diagrams were created to visualise relationships between type of intervention, study location, and changes in placental phenotype (or no changes; RAWGraphs [25]).
Statistical analysis
Data were analysed using JMP 16.0. Relative risk (RR; 95% confidence interval) with p value from Fisher’s exact test (2-tail) was used to determine whether nutritional interventions that improved maternal or offspring outcomes were more likely to associate with placental changes than interventions that did not improve maternal or offspring outcomes.
Results
Study and cohort characteristics
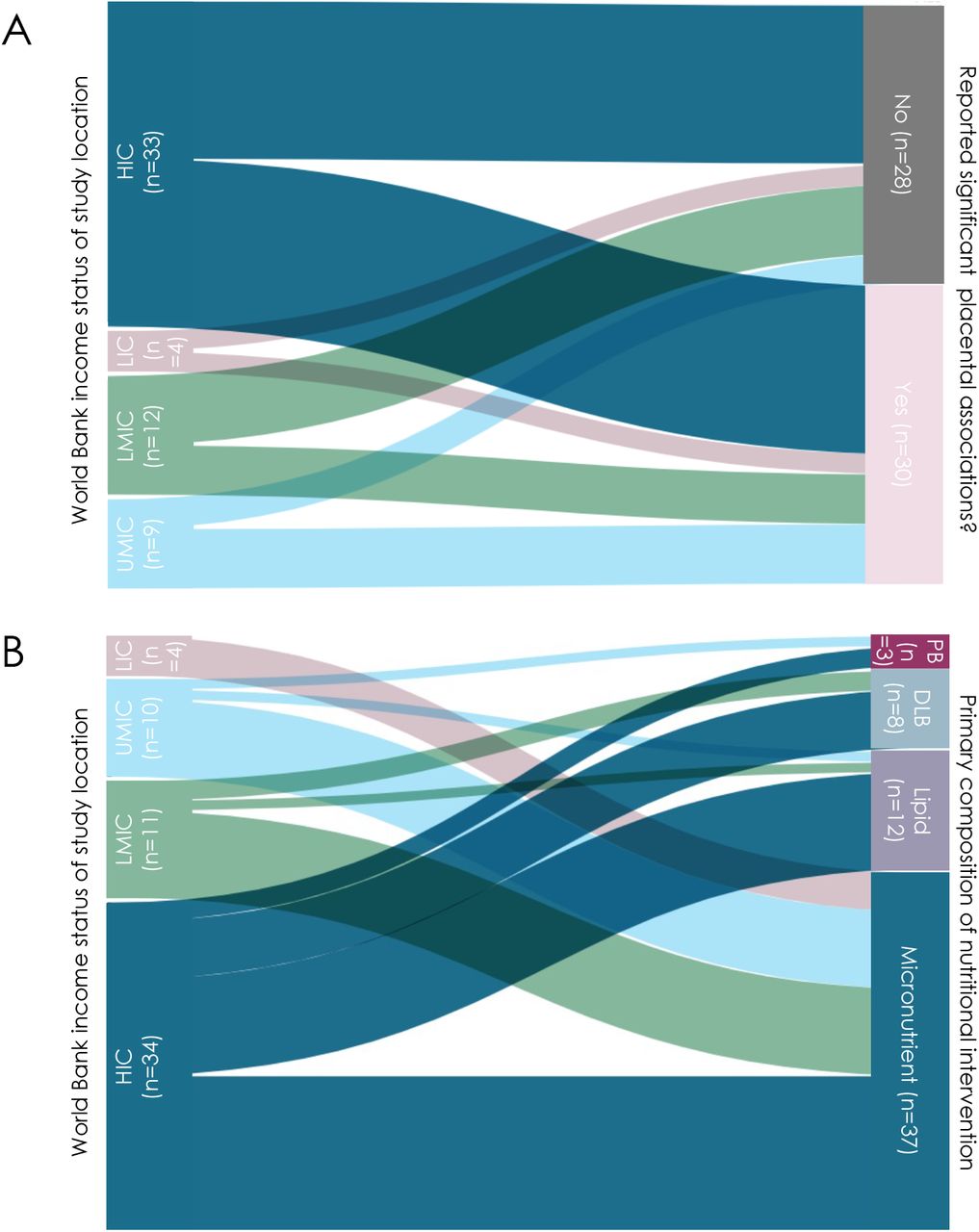
The 53 included studies were randomised controlled clinical trials (n=43 [81%]), interventional clinical trials (n=7 [13%]), controlled feeding studies (n=2 [4%]), and intention-to-treat studies (n=1 [2%]). These studies administered micronutrient- (n=33 [62%]), lipid- (n=11 [21%]), protein- (n=3 [6%]) and diet and lifestyle-based (n=8 [15%]) interventions. The included studies reported on cohorts from LICs (n=4 [7.5%]), LMICs (n=12 [23%]), UMICs (n=9 [17%]), and HICs (n=33 [62%]; Figures 2-3). Five studies reported findings from multiple cohorts, which included participants from countries with differing socioeconomic statuses.


Diagram created on app.rawgraphs.io website. LIC = low-income country. LMIC = low-middle income country. UMIC = upper-middle income country. HIC = high-income country. n = number of studies. DLB = Diet and lifestyle-based. PB = protein-based.
The majority (n=46 [87%]) of studies included only singleton pregnancies, while seven (13%) included both singleton and twin pregnancies. Maternal comorbidities were common in the studies under review (n=33 [62%]) and were either a criterion to be a participant in the nutritional intervention trial or were identified as a potential confounding variable by the original authors. The most common comorbidities included a history or diagnosis of preeclampsia (n=12 [36%]), prior or current hypertension (n=7 [21%]), overweight and/or obesity (n=7 [21%]), smoking (n=6 [18%]), and/or any type of diabetes (n=6 [18%]; Supplementary Table S4). Twenty studies excluded pregnant participants with comorbidities.
Presence of a maternal nutrient deficiency was a selection criterion for three [5.6%] of the studies. All studies reported self-administration of the intervention by the participant, and three studies also included an additional intervention administered by a research team member once weekly. Interventions began either peri- (n=3 [6%]) or post-conceptionally (n=50 [94%]; 14 beginning in the first trimester, 28 in the second trimester, and 11 in the third trimester), with the majority continuing until birth (n=52 [98%]), and one that finished after 12 weeks of administration.
Adverse effects and events were reported in five and one study, respectively, and included gastrointestinal complaints following multiple micronutrient [26] or iron [27] supplementation, an increased incidence of preterm birth following iron supplementation [28], an increased likelihood of antenatal hospital admission with hypertension following vitamin C+E supplementation (exact cause unknown to the researchers) [29], and reports of general developmental abnormalities in both the treatment vitamin C+E and placebo groups [30].
Risk of bias assessments
All 53 studies under review had low or unclear risk of selection, detection, attrition, and reporting bias (Figure 4). Risk of performance bias was assessed to be high in 5 trials (9%) where blinding was not possible given the nature of the nutritional intervention (Figure 4). Most studies (n=38 [72%]) had a low RoB related to intervention compliance, however, methods for measuring intervention compliance were unclear in over one quarter of the studies under review (n=14 [26%]), and one study was assessed to have a high RoB due to limited participant follow up and no reported compliance measures (Figure 4) [31]. Results from RoB assessments were used to inform results synthesis and interpretations if the study reported significant associations between its nutritional intervention and placental phenotype.

Nutritional interventions associated with improved maternal and infant outcomes
Forty studies in total reported maternal and/or infant outcomes, with 50% (n=20) and 25% (n=10) of studies reporting only maternal or infant outcomes, respectively, and 25% (n=10) of studies reporting both (Supplementary Tables S5 and S6). Maternal and offspring outcomes were reported as being improved following nutritional intervention in 13/30 (43%) and 7/20 (35%) of the studies, respectively, that reported these data.
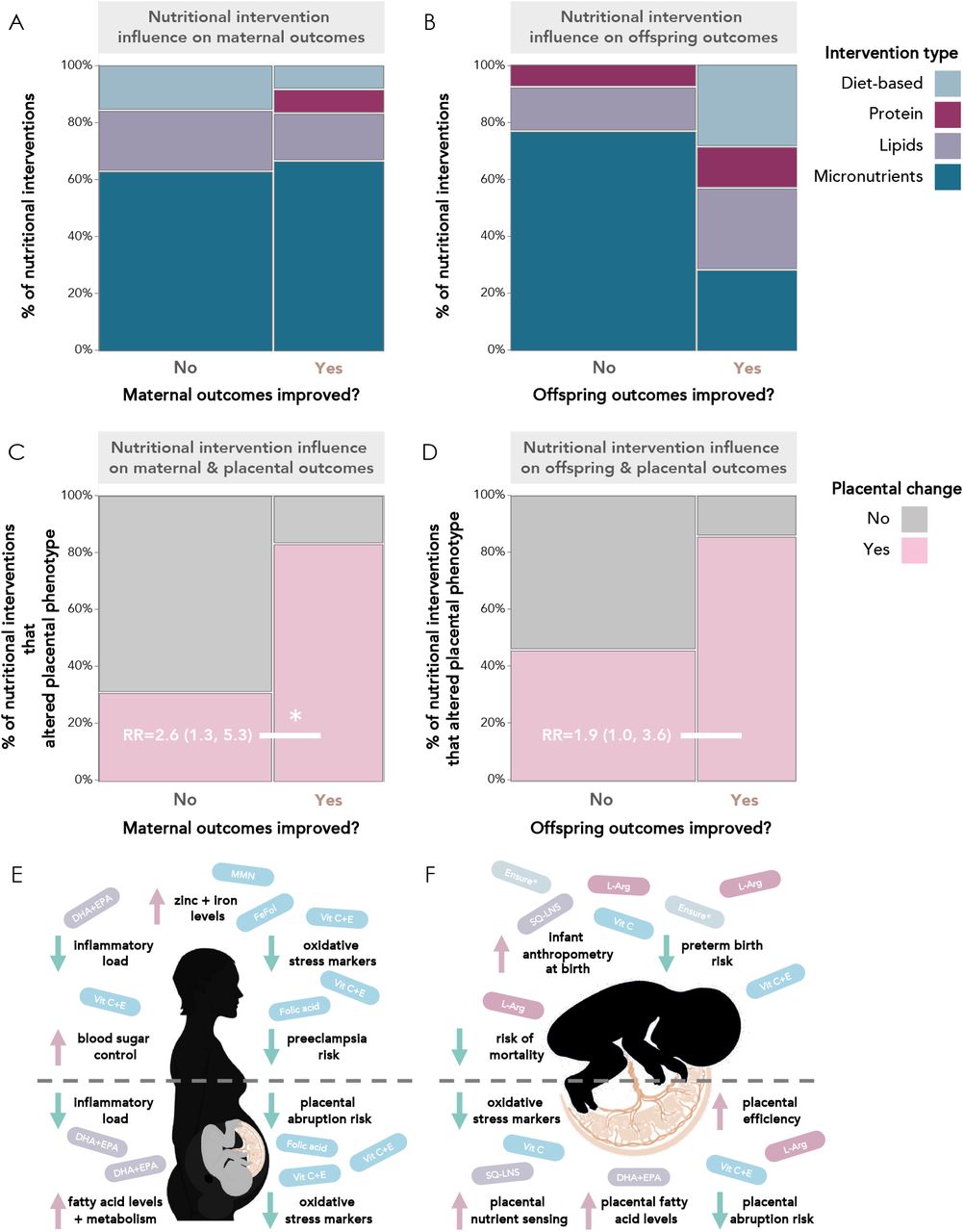
There were 12 nutritional interventions that associated with improved maternal outcomes, including one diet and lifestyle-based intervention, one protein-based intervention, two lipid-based interventions, and eight micronutrient-based interventions (Figure 5A). Improved maternal outcomes included a smaller required insulin dose in mothers with gestational diabetes (following vitamin C supplementation [32]), reduced blood levels of iron and/or zinc (following iron [33] and multiple micronutrient supplementation [34]), decreased total lipid content in placental tissue (following docosahexaenoic acid [DHA] and eicosapentaenoic acid [EPA] supplementation [35]), decreased risk of preeclampsia (following calcium [36], L-arginine and multiple micronutrient supplementation [37]), and decreased risk of placental abruption (following magnesium citrate supplementation [38]; Figure 5A).

(A) Of the 12 nutritional interventions that associated with improved maternal outcomes, one was diet and lifestyle-based (8%), one was protein-based (8%), two were lipid-based (17%), and eight were micronutrient-based (67%). (B) Of the seven nutritional interventions that associated with improved infant outcomes, two (29%) were diet and lifestyle-based, one was protein-based (14%), two (29%) were lipid-based, and two (29%) were micronutrient-based. Nutritional interventions that improved maternal (C) and offspring (D) outcomes were more likely to associate with placental changes than interventions that did not improve maternal or offspring outcomes. Visual summary of the nutritional interventions and beneficial maternal (E), offspring (F), and placental (E-F) outcomes reported in the studies under review. Mosaic plots are proportion (%) of studies reporting improvement, or no improvement, in maternal (A, C) and offspring (B, D) outcomes. Data in C and D are relative risk (95% confidence interval). *Significance = p<0.05 from Fisher’s exact test (2-tail). RR = relative risk. FeFol = iron-folic acid. Vit = vitamin. DHA = docosahexaenoic acid. EPA = eicosapentaenoic acid. SQ-LNS = small-quantity lipid-based nutrient supplements. L-Arg = L-arginine.
Of the seven nutritional interventions that associated with improved infant outcomes, two were diet and lifestyle-based, one was protein-based, two were lipid-based, and two were micronutrient-based (Figure 5B). Improved infant outcomes included improved fetal growth (following lipid supplementation [39]), increased fetal nervonic acid ratio (following EPA and DHA supplementation [40]), and a decreased risk of intrauterine growth restriction (IUGR; following L-arginine supplementation [41]), twin-to-twin transfusion syndrome incidence (TTTS [a syndrome that can occur in diamniotic monozygotic twin pregnancies that creates an imbalance in nutrient allocation between fetuses]; following Ensure® liquid supplementation [42]), and preterm birth (for infants born to mothers who smoked; following vitamins C+E (supplementation with both vitamins concurrently) [43]; Figure 5B).
Classifications of placental outcomes
Of the 53 included studies, 29 studies (51%) reported on more than one placental outcome across the five categories, for a total of 88 outcomes noted across all studies: 19 (22%) of the studies reported on placental anthropometry, 24 (27%) reported on placental molecular changes, five (6%) reported on placental pathology, 19 (22%) reported on placental abruption, and 21 (24%) reported on a placental-related disease (Supplementary Table S7).
Direct nutritional interventions associate with placental phenotype
Specific micronutrient-based interventions associate with placental phenotype
Of the 33 studies that used a micronutrient-based intervention, 16 (48%) reported associations between the nutritional intervention and placental phenotype (Figure 6). Micronutrient interventions that associated with altered placental phenotype began during the first (n=3), second (n=9), and third trimesters (n=4; Figure 6).


Income status of study location obtained from World Development Indicators by The World Bank Database. LIC = Low-income country. LMIC = Low- to middle-income country, UMIC = Upper-middle-income country, HIC = High-income country. Sm = Smoker. NSm = Non-smoker. N = Number of participants. Pre = Pre-conception. PEB = Protein-Energy Ball. MMN = Multiple Micronutrient. GDM = Gestational diabetes mellitus. Anth = Anthropometry. Molec = Molecular Alterations. Patho = Pathology. PA = Placental abruption. PD = Placenta-related disease. A dash (-) under “Details” indicates no significant placental phenotype alterations. Circles for this review’s secondary outcomes were only placed if the study reported fetal/infant or maternal outcomes as a primary outcome of their study. aVadillo-Ortega, 2011, and Larqué, 2006 appear as duplicates on 2 separate pages between figures 6-8 due to their crossover between intervention categories. Income status of study location obtained from World Development Indicators by The World Bank Database. LIC = Low-income country. LMIC = Low- to middle-income country, UMIC = Upper-middle-income country, HIC = High-income country. N = Number of participants. Pre = Pre-conception. L-arg = L-arginine. MTHF = 5-methyl-tetrahydrofolic acid. Anth = Anthropometry. Molec = Molecular Alterations. Patho = Pathology. PA = Placental abruption. PD = Placenta-related disease. A dash (-) under “Details” indicates no significant placental phenotype alterations. Circles for this review’s secondary outcomes were only placed if the study reported fetal/infant or maternal outcomes as a primary outcome of their study. aVadillo-Ortega, 2011, and Larqué, 2006 appear as duplicates on 2 separate pages between figures 6-8 due to their crossover between intervention categories.
Associations between micronutrient-based nutritional interventions and placental anthropometry were reported in two studies, including increased placental weight at term (following daily vitamin C and zinc supplementation initiated during the first trimester in a population at high risk for malaria and low birthweight [44]), and increased chorionic villi density (following vitamin D supplementation that began in the late first or early second trimester in mothers at high risk of having offspring with asthma [45]; Figure 6).
One study reported associations between micronutrient-based interventions and placental pathology [28], where daily iron supplementation initiated periconceptionally was associated with a decreased risk of chorioamnionitis (a maternal inflammatory response leading to the infiltration of neutrophils into the placenta) in a population at high risk for malaria and chorioamnionitis [28] (Figure 6).
Half (n=8) of these 16 micronutrient-based intervention studies reported differences in placental molecular changes between the control and intervention groups. Placental molecular changes included increased expression or activity of the following: placental superoxide dismutase (an antioxidant enzyme [46]; following daily vitamin C supplementation initiated upon gestational diabetes diagnosis [32]), transferrin receptor 1 mRNA (involved in placental iron uptake [34, 47]; following a daily multiple micronutrient intervention that began in the second trimester [34]), genes involved in vitamin D metabolism (after daily vitamin D supplementation that started in the third trimester[48]), soluble fms-like tyrosine kinase-1 (SFLT-1; following daily vitamin D plus 5-methyl-tetrahydrofolic acid [MTHF] supplementation that started in the second semester[49]), and placental phospholipid DHA (after daily 5-MTHF and DHA supplementation that began in the second trimester [50]). Molecular changes also included modified expression of five genes in placental tissue (increased expression of metastasis associated in colon cancer-1 [MACC1], integrator complex subunit 9 [INST9], Von Willebrand factor [vWF], and age-related maculopathy susceptibility 2 [ARMS2]; and decreased expression of contactin 5 [CNTN5]; following daily vitamin D supplementation initiated in the second trimester [45]). In two studies from a single trial of daily maternal choline supplementation initiated during the third trimester [51], increased methylation of multiple cortisol-regulating genes and dysregulation of 197 different placental biological processes was reported [52, 53].
Placental abruption risk following nutritional intervention was assessed in 16 studies, where two interventions, which supplemented either daily vitamin C+E [43] (initiated during the first trimester) or magnesium citrate [38] (initiated during the second trimester) were associated with decreased abruption risk (Figure 6). In contrast, two studies from the Diabetes and Preeclampsia Intervention Trial (DAPIT) [54], which supplemented daily vitamin C+E (that began in the first trimester) in mothers with diabetes to lessen preeclampsia risk, reported no differences in placental abruption risk in the full cohort [54] or in follow-up studies with a cohort subset [55]. Two studies from the Combined Antioxidant and Preeclampsia Prediction Studies (CAPPS) trial reported that placental abruption risk was decreased in mothers who smoked [43], but not the intervention group overall [56], following daily vitamin C+E supplementation that started in the first trimester.
Placental-related disease risk was decreased in 5 (33%) of the 15 studies that evaluated placental-related disease occurrence following nutritional intervention. These findings included a decreased risk of premature rupture of membranes (PROM; following daily vitamin C+E supplementation initiated in the second trimester [30]), histopathological-positive placental malaria risk (following daily vitamin A and zinc supplementation that started in the third trimester [44]), and preeclampsia (following daily interventions with either folic acid [57] that began pre-conceptionally, or calcium [36] initiated in the second trimester; Figure 6). In the CAPPS trial [58], no changes in the risk of preeclampsia [43, 56], or amnio-choriodecidua [59], were reported following daily vitamin C+E supplementation initiated in the first trimester.
For the remaining 17/33 studies that used a micronutrient-based intervention, there were no reported associations between micronutrient interventions and placental anthropometry (n=5 [30%]) [26, 33, 60, 61], pathology (n=1 [6%]) [33], molecular changes (n=5 [30%]) [26, 27, 59, 60, 62], abruption risk (n=8 [47%]) [29, 54-56, 63-66], or placental-related disease (n=8 [47%]) [29, 33, 54, 56, 63, 64, 67, 68].
Specific macronutrient-based interventions influence placental phenotype
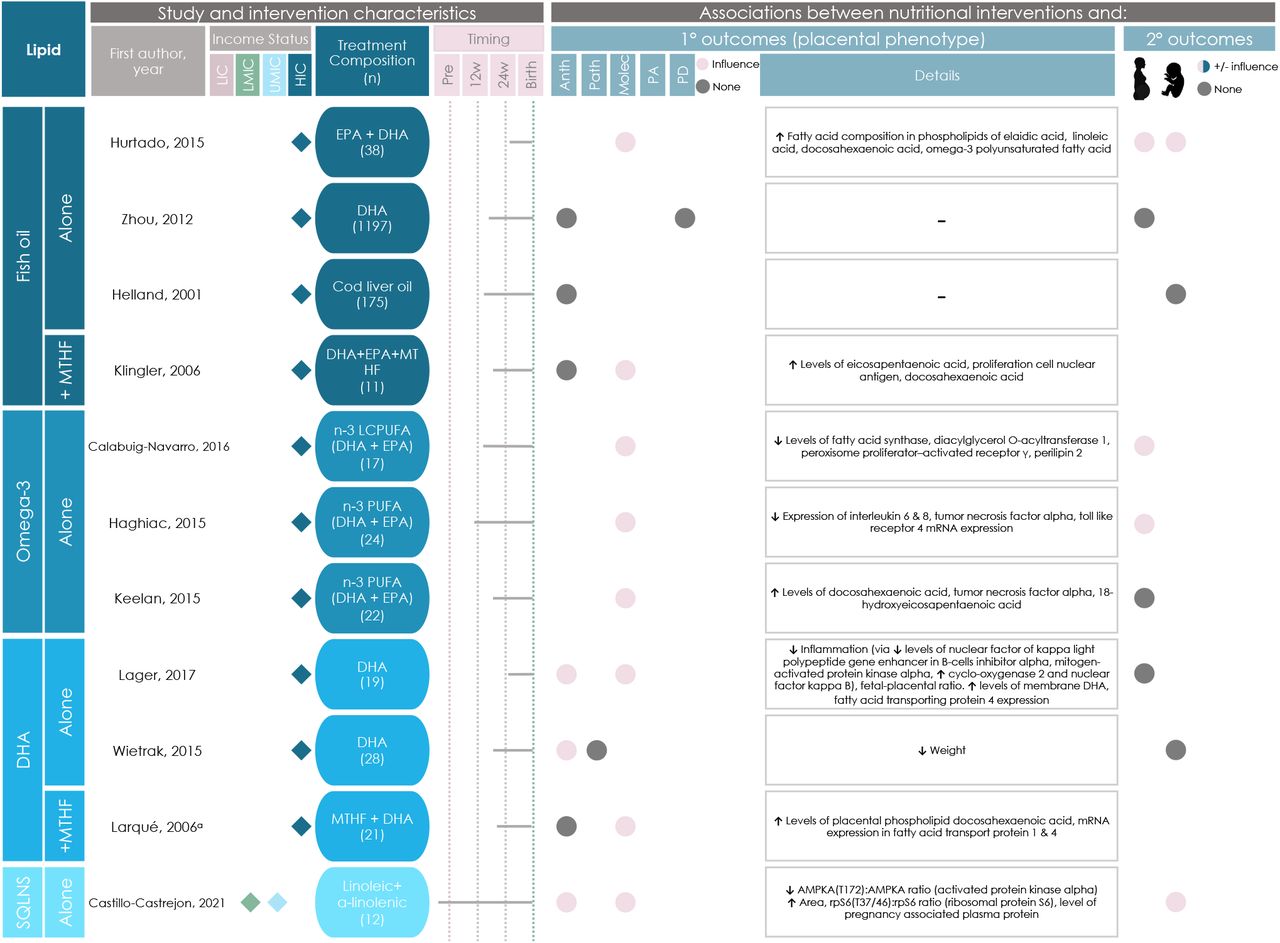
Of the 11 studies that reported on lipid-based interventions, nine (82%) reported placental changes in the intervention group (Figure 7). Lipid-based interventions that associated with altered placental phenotype began during the first (n=2), second (n=5), and third trimesters (n=2; Figure 7).

Income status of study location obtained from World Development Indicators by The World Bank Database. LIC = Low-income country. LMIC = Low- to middle-income country, UMIC = Upper-middle-income country, HIC = High-income country. N = Number of participants. Pre = Pre-conception. L-arg = L-arginine. MTHF = 5-methyl-tetrahydrofolic acid. SQLNS = Preconceptional maternal small-quantity lipid-based nutrient supplementation. EPA = eicosapentaenoic acid. DHA = docosahexaenoic acid. N-3 PUFA = omega-3 polyunsaturated fatty acid. Anth = Anthropometry. Molec = Molecular Alterations. Patho = Pathology. PA = Placental abruption. PD = Placenta-related disease. A dash (-) under “Details” indicates no significant placental phenotype alterations. Circles for this review’s secondary outcomes were only placed if the study reported fetal/infant or maternal outcomes as a primary outcome of their study. aVadillo-Ortega, 2011, and Larqué, 2006 appear as duplicates on 2 separate pages between figures 6-8 due to their crossover between intervention categories.
Changes in placental anthropometry were reported in three lipid-based intervention studies (Figure 7). Decreased placental weight [69] and fetal:placental weight ratio [70] were reported following daily DHA supplementation that began in the second and third trimester, respectively, while pre-conceptionally initiated daily maternal small-quantity lipid-based nutrient supplementation (SQLNS) was associated with an increase in placental area [39] (Figure 7).
Eight lipid-based interventions were associated with molecular changes in the placenta, namely in placental processes related to inflammation and fatty acid transport (Figure 7). The molecular changes included increased expression or concentration of: placental linoleic acid (following daily fish oil supplementation that started in the third trimester [40]), proliferating cell nuclear antigen (PCNA; which plays a key role in nucleic acid metabolism [71]; following daily fish oil supplementation that began in the second trimester [72]), and tumor necrosis factor alpha (TNFα; following daily omega-3 supplementation that started in the second trimester [73]). Decreased expression of placental inflammatory markers (following daily DHA supplementation initiated in the third trimester [70]), and decreased activated protein kinase alpha ratio (AMPKA [a regulator in cell metabolism]; following daily pre-conceptionally initiated SQLNS supplementation [39]) were also reported (Figure 7). Two studies from a single clinical trial that supplemented omega-3 fatty acids (beginning in the second trimester) reported a significant reduction in the expression of pro-inflammatory genes in placental tissue and decreased placental lipid storage capacity [35, 74, 75]. Two studies that reported findings from a trial of daily DHA and MTHF supplementation that began in the second trimester reported alterations to DHA content in placental phospholipids and expression of PCNA [72] and alterations to placental fatty acid transport proteins [50].
Two of the 11 (18%) lipid-based interventions did not associate with placental changes (Figure 7). In both interventions, a daily fish oil supplement was taken, beginning in the second trimester, and placental weight [76] and preeclampsia risk [77] were not altered (Figure 7).
Three of the 53 studies used amino acid- or protein-based interventions (Figure 8). Two (66%) of these three studies reported associations between the intervention and placental phenotype. Daily supplementation with L-arginine initiated during the third trimester was associated with an increased cerebro-placental ratio (a gestational indicator associated with adverse pregnancy outcomes like low-birth weight [78]) when compared to the control group [41], and twice daily supplementation with L-arginine and antioxidant vitamins that began in the second trimester associated with a decreased risk of preeclampsia [37] (Figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Income status of study location obtained from World Development Indicators by The World Bank Database. LIC = Low-income country. LMIC = Low- to middle-income country, UMIC = Upper-middle-income country, HIC = High-income country. N = Number of participants. Pre = Pre-conception. L-arg = L-arginine. IPTp-SP = intermittent preventative treatment in pregnancy with sulphadoxine-pyrimethamine. DiMO = monochorionic diamniotic twin pregnancy. Anth = Anthropometry. Molec = Molecular Alterations. Patho = Pathology. PA = Placental abruption. PD = Placenta-related disease. A dash (-) under “Details” indicates no significant placental phenotype alterations. Circles for this review’s secondary outcomes were only placed if the study reported fetal/infant or maternal outcomes as a primary outcome of their study. aVadillo-Ortega, 2011, and Larqué, 2006 appear as duplicates on 2 separate pages between figures 6-8 due to their crossover between intervention categories.
Of the one (33%) amino acid- or protein-based intervention that did not associate with placental phenotype, supplementation of L-arginine initiated in the third trimester did not associate with changes in placental weight, abruption risk, or thrombosis [79] (Figure 8).
Specific diet and lifestyle-based interventions influence placental phenotype
Eight interventions were diet and lifestyle-based and three (38%) associated with placental phenotype.
An intervention that delivered a daily probiotic supplement and dietary education and support (to promote a diet in line with nutritional guidelines and maintenance of appropriate fat consumption) that began during the second trimester associated with increased concentration of polyunsaturated fatty acids in the placenta [80]; Figure 8).
Two diet and lifestyle-based interventions were associated with a reduced risk of placental-disease. Daily Ensure® liquid nutritional supplementation initiated during the second trimester was associated with reduced TTTS diagnosis and incidence at birth [42] (Figure 8). Haematinics and intermittent preventative treatment (IPTp-SP) administered daily during the third trimester until birth was associated with reduced placental malaria incidence in the treatment group when comparing mothers with the same human immunodeficiency virus (HIV) status [81] (Figure 8).
The remaining five (63%) of diet and lifestyle-based interventions did not associate with placental changes (Figure 8) [31, 82-85].
Intervention effects on the placenta vary by study location
Studies that took place in LIC and LMIC reported fewer associations between nutritional interventions and placental changes than studies that took place in UMIC and HIC (Figure 3A). All nutritional interventions in LIC (n=4) were micronutrient-based (Figure 3B). Of these, two (50%) reported associations between the intervention and placental pathology (n=1 study) and placental molecular phenotype (n=1; Figure 3A). Nutritional interventions in LMIC were micronutrient-based (n=9 [75%]), lipid-based (n=1 [8%]), or diet and lifestyle-based (n=2 [16%]), of which, five (42%) reported placental changes following the nutritional intervention (Figures 3A-B). In the five LMIC-based studies, associations between the nutritional intervention and placental anthropometry (in n=2 studies [29%]), placental molecular phenotype (n=2 [29%]), and placenta-related disease (n=3 [43%]) were reported.
Nutritional interventions in UMIC were micronutrient-based (n=8 [89%]) or lipid-based (n=1 [11%]), and of these, six (66%) reported associations between the intervention and placental phenotype (Figures 3A-B). In these six UMIC studies, associations between the nutritional intervention and placental anthropometry (in n=1 study [13%]), placental molecular phenotype (n=1 [13%]), placental abruption (n=1 [13%]), and placental-related disease (n=5 [63%]) were reported.
Nutritional interventions in HIC were micronutrient-based (n=16 [48%]), lipid-based (n=16 [48%]), protein-based (n=2 [6%]), or diet and lifestyle-based (n=6 [18%], Figure 3B), of which, 51% (n=17) reported associations between the intervention and placental phenotype (Figure 3A). These 17 HIC-based studies reported associations between the nutritional intervention and placental anthropometry (in n=4 studies [20%]), placental molecular phenotype (n=14 [70%]), placental abruption (n=1 [5%]), and placental-related disease (n=1 [5%]).
Interventions associated with placental phenotype are more likely, overall, to improve maternal and offspring outcomes
Maternal outcomes positively associate with placental changes
Maternal outcomes were more likely to be improved in studies that reported placental changes following nutritional intervention than studies that reported no placental changes (n=11 [69%] vs. n=2 [13%], RR = 2.6 [1.3, 5.3]; Figure 5C).
Of the eight micronutrient-based intervention studies that reported improved maternal outcomes, seven (89%) reported associations between the intervention and placental phenotype. Placental changes and improved maternal outcomes included: a reduction in oxidative stress markers in both the placental tissue and maternal blood plasma (following vitamin C supplementation starting once the mother was diagnosed with gestational diabetes [32]) and increased mRNA expression of placental iron uptake transferrin receptor 1 and increased maternal iron and zinc levels (after multiple micronutrient supplementation initiated in the second trimester [34]), and decreased risk of placental abruption (which was classified as both a placental and maternal outcome in this study; following magnesium citrate supplementation starting in the second trimester [38]). Additionally, reduced risk of preeclampsia was reported in four studies, as discussed above [36, 37, 53, 57].
For macronutrient-based interventions, all three of the lipid-based studies that reported improved maternal outcomes also reported placental changes following nutritional intervention. Omega-3 supplementation beginning in the first trimester was associated with increased maternal plasma DHA and EPA levels and decreased expression of placental factors like interleukin 6 and 8 [74], whilst omega-3 supplementation beginning in the second trimester was associated with increased maternal plasma DHA and EPA enrichment, and decreased total lipid content and ability of the placenta to store and esterify lipids [35]. Further, daily fish oil supplementation initiated during the third trimester was associated with increased maternal circulating DHA and plasma nervonic acid content, and increased fatty acid concentration in placental tissue [40]. Reduced risk of preeclampsia, but not placental abruption, was reported in one protein-based study as discussed above [37].
One of the four diet and lifestyle-based interventions that included maternal outcome data reported improved maternal outcomes following intervention without changes in the placenta [83].
Offspring outcomes positively associate with placental changes
Studies that reported placental changes were more likely to report improved offspring outcomes than those that did not reported placental changes (n=6 [54%] vs. n=1 [11%], RR = 1.9 [1.0, 3.6]) (Figure 5D).
Of the 12 micronutrient-based interventions that included data on offspring outcomes, two (17%) reported changes in placental phenotype and improved offspring outcomes following nutritional intervention. In mothers with gestational diabetes mellitus, daily supplementation with vitamin C from diagnosis onwards was associated with a reduction in both fetal and placental oxidative stress markers and newborn birthweight, in comparison to the non-treatment group [32]. A decreased risk of both preterm birth and placental abruption was also reported in a cohort of mothers who smoked during pregnancy following daily vitamins C+E supplementation initiated during the first trimester [43]. One of the 12 studies with offspring outcome data also reported an adverse offspring outcome (increased incidence of preterm birth) following daily ferrous gluconate supplementation from preconception to birth, despite noting a reduced risk of chorioamnionitis [28].
Of the macronutrient-based interventions, two of four lipid-based interventions that reported offspring outcome data observed altered placental phenotype and improved offspring outcomes. SQLNS supplementation initiated preconceptionally was associated with improved fetal growth, increased placental area [39], and changes in expression of multiple placental metabolic genes. Fish oil supplementation initiated in the third trimester was associated with higher offspring plasma nervonic acid content, increased polyunsaturated placental fatty acid composition, but no changes to visual or cognitive development outcomes measured in the offspring [40]. Additionally, two protein-based interventions reported on offspring outcomes, with one noting increased cerebro-placental ratio and decreased incidence of intrauterine growth restriction (IUGR) following daily L-arginine supplementation initiated during the third trimester [41].
Improved offspring outcomes were reported in two diet and lifestyle-based intervention studies, one of which also reported placental changes following the intervention. First, Ensure® liquid supplementation initiated upon diagnosis of a monochorionic diamniotic pregnancy was associated with decreased risk of TTTS and incidence at delivery time [42]. Second, daily chlorella supplementation beginning in the second trimester was associated with decreased fetal dioxin transfer (measured through decreased total toxic equivalents), but no significant change in toxin concentrations pre- and post-treatment [31]. Notably, we determined the second study to have a high RoB.
Data on sex differences in placental response to nutritional interventions are lacking
Only 17 (32%) of the studies under review included data on the number of male and female offspring in the study, and no studies reported data on placental outcomes stratified by sex.
Discussion
Here, we synthesized evidence on how direct maternal nutritional interventions influence placental phenotype in humans. Lipid-based interventions were the most likely to associate with altered placental phenotype, most often related to changes in placental inflammatory processes or markers. Further, we found that interventions that associate with placental changes are more likely to also improve maternal and offspring outcomes. Studies that took place in HICs were the most likely to report associations between nutritional interventions and placental phenotype, although LICs were underrepresented in the reviewed studies. Sex-differences or -specific effects of nutritional interventions on placental outcomes were underreported. Critically, investigating how direct maternal nutritional interventions during the preconception and pregnancy periods influence placental phenotype strengthens our understanding of the mechanisms underlying intervention effectiveness, and could inform the development of better targeted approaches to improve maternal-fetal health.
Nutritional interventions that associated with placental changes were more likely to also improve maternal and offspring outcomes. Specifically, we found that improved maternal iron levels, inflammatory status, and blood sugar control may be accompanied by placental changes, including increased placental nutrient transporter expression [34] and decreased placental expression of inflammatory and oxidative stress markers [32, 74], respectively. Similarly, decreased placental abruption risk [43], increased cerebro-placental ratio [41], and greater placental area [39] following nutritional intervention corresponded with a decreased risk of preterm birth, IUGR, and improved fetal growth, respectively. While it is well-accepted that nutritional interventions have the potential to improve maternal and offspring outcomes [86, 87], our findings suggest that understanding the placental response to nutritional interventions may reveal insights into the biological mechanisms that determine an intervention’s impact on maternal or offspring health.
Several studies reported changes in maternal, placental, or offspring expression and/or levels of various pro-inflammatory biomarkers following micronutrient- and lipid-based nutritional interventions [32, 40, 50, 70, 72-74]. Decreased levels of oxidative stress markers, which in excess can amplify pro-inflammatory pathway and process activity [88], were reported in placental tissue and maternal and offspring blood following vitamin C supplementation [32]. Increased oxidative stress in the placenta can adversely affect fetoplacental development and pregnancy health [89, 90], and has implications in fetal programming for future disease risk [91]. Additionally, increases in placental and maternal circulating levels of anti-inflammatory DHA and EPA were reported following lipid-based interventions [40, 50, 70, 72, 73]. During pregnancy, DHA and EPA play a key role in promoting angiogenesis and reducing oxidative stress and inflammation in the placenta, and are required to support fetal brain development throughout pregnancy [92]. Collectively, our findings suggest that common nutritional interventions may impact placental inflammatory processes which can, in turn, associate with altered maternal and offspring outcomes [89-91]. An improved understanding of how maternal nutritional interventions can influence placental inflammation is critical for improving outcomes in pregnancies with maternal comorbidities like obesity and metabolic syndrome, which are associated with chronic, low-grade inflammation and altered placental nutrient transport [93, 94].
None of the reviewed studies reported on placental changes stratified by sex. As there are sex-specific differences in placental development, including in nutrient exchange capacities [95], it is likely that the sex of the placenta would influence the placental response to a nutritional intervention [96] and this is an area requiring further study. Similarly, LICs were underrepresented in the reviewed studies, with only four studies taking place in LICs. As LICs are often the setting where nutritional interventions are most needed due to higher rates of undernutrition [97, 98], further research on the placental response to nutritional interventions in these settings is needed.
Strengths of this study include it being the first to synthesize knowledge on relationships between direct maternal nutritional interventions and placental phenotype, with consideration of placental outcomes beyond placental-related pregnancy complications [99], and that our focus was limited to only human studies to increase the clinical relevancy of our findings [100]. Further, we identified key gaps in the literature, related to the lack of sex-stratified placental data and underrepresentation of LMICs, which may inform future studies. Limitations of this review include the lack of formal meta-analysis due to the high variability in the types of placental outcomes reported in the reviewed studies, and our inability to consider how individual differences in study participants, including dietary history or nutritional status, may have influenced placental response to an intervention. In many cases, the scope and detail of placental data available in the reviewed studies were limited, and intervention timing, frequency, and duration varied, which made direct comparisons between studies difficult. The reviewed studies were also largely concentrated in HICs, limiting the generalizability of our findings to other contexts. Lastly, around one quarter of studies did not report or had unclear compliance data, limiting our ability to consider how intervention adherence may have influenced the intervention’s impact on placental phenotype.
Advancing nutritional interventions and maternal-child health through placental research
Informed by the findings of this review, we recommend that future research on direct maternal nutritional interventions include comprehensive placental analysis following birth. To do so, we recommend the following implementations and future directions:
Build upon the variables in the existing core outcome set, “Pregnancy Nutrition Core Outcome Set” such as diet quality, pregnancy complications, and need for interventions and nutritional supplements [101], to set a universal standard for capturing and reporting on placental and maternal variables important to fully understand the maternal and placental response to nutritional interventions. New variables should include:
Placental sex
Placental anthropometry (weight, diameter)
Placental pathology (where applicable, or banking of fixed placental specimens for future histomorphology and pathology assessments)
Collection of placental tissue core samples for future analysis of placental phenotype, including function, if not intended for the immediate study
Maternal characteristics and environmental factors such as pre-pregnancy nutritional status, comorbidities, age, medical history, and anthropometry.
Adverse events and effects
Increase collection and phenotyping of placental samples from nutritional intervention studies situated in LMICs and LICs, to improve representation and understanding of placental mechanisms and adaptations associated with the early life nutritional environment across diverse populations and geographies.
Determine optimal windows for nutritional interventions (i.e., interventions initiated pre-conceptionally, in early pregnancy, or in later pregnancy) for improving maternal and offspring outcomes, and how the placenta adapts to, and influences pregnancy outcomes, based on timing of exposure.
Research focused on developing human nutritional intervention(s) targeted to the placenta to, in turn, improve pregnancy/offspring outcomes. Non-nutritional based therapies (such as the use of liposomes to enhance drug delivery to the placenta) have the potential to improve offspring outcomes via placental changes [102], and nutritional interventions may be able to do the same.
We found that direct maternal preconception and prenatal nutritional interventions that target maternal health and nutritional status also influence placental development and function. These (potentially unintended) placental adaptations are likely beneficial for the pregnancy and may underlie the improved growth and development of offspring observed in these pregnancies. Understanding the placental response to nutritional interventions is key for modifying and improving approaches to address nutrient deficiencies, to reduce maternal and neonatal morbidity and mortality globally.
Data Availability
All data discussed are available in the published articles included in this review.
Author contributions
Conceptualization, MW and KLC.; methodology, VB, MW, and KLC; formal analysis, VB and MW; investigation, VB, MW, and KLC; data curation, VB and MW; writing—original draft preparation, VB, MW, and KLC; writing—review and editing, VB, MW, and KLC; visualisation, VB, MW, and KLC; supervision, KLC and MW; funding, KLC. All authors have read and agreed to the published version of the manuscript.
Funding
KLC is funded by the Canadian Institutes of Health Research (310063) and Natural Sciences and Engineering Research Council of Canada (315096). MW was supported by an Ontario Graduate Scholarship and VB was supported by an I-CUREUS internship.
Footnotes
↵† Senior authors
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.
- 16.
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵



