
Abstract
Background The National Health Service (NHS) has the most diverse workforce in the United Kingdom (UK), 25% (n= 309,532/1,200,000) of staff belong to ethnic minority groups. However, there is evidence of longstanding issues of racism within the NHS and discrimination towards ethnic minority healthcare staff has been rising since 2016. In the first wave of the COVID-19 pandemic, 95% of COVID-19 deaths among doctors were in an ethnic minority group. There has been no definitive answer for the disproportionate COVID-19 mortality but socioeconomic factors due to structural racism have been suggested as the main drivers. No studies have assessed the effectiveness of antiracist interventions for healthcare staff.
Methods We conducted a systematic review; databases searched included: AMED, Medline via OVID, CINAHL, APA Pyscinfo, Web of Science and OVID Emcare 25th– 31st January 2022. The interventions were structured using a model of antiracist interventions and analysed using narrative synthesis methods.
Results 16 papers were reviewed with interventions at different levels: personally mediated (n=9), multilevel (n=4) and institutional (n=3). Personally mediated interventions were workshops (n=8) and a mentorship scheme (n=1). Institutional interventions were policies (n=2) and increasing diversity initiative (n=1). Multilevel interventions were a mix of both. Study designs and risk of bias tools indicated that the quality of evidence was of low quality. Only two studies included control groups. Countries included the USA (n=11), Canada (n=1) and the UK (n=4).
Conclusion There is a lack of robust evidence for antiracist interventions for healthcare staff, especially at an institutional level. High quality research is required to evaluate the long-term effects of interventions.
Funding statement The Wales COVID-19 Evidence Centre was funded for this work by Health and Care Research Wales on behalf of Welsh Government.
Introduction
The National Health Service (NHS) has the most ethnically diverse workforce in the United Kingdom (UK), with 21% of staff belonging to ethnic minority groups (1). However, racism towards staff operates at many levels; from bullying and harassment (2), to limited career advancement (3), and increased disciplinary action (4). During the first COVID-19 wave (year), 95% of all doctors who died were from ethnic minorities (5). There has been no definitive answer for this disproportionate COVID-19 mortality. Socio-economic factors, such as deprivation, due to longstanding structural racism were cited as main contributors to this mortality rate and the effectiveness of interventions addressing this is unclear (6).
Institutional racism can be defined as ‘the collective failure of an organisation to provide an appropriate service to people based on their ethnic origin, evident in processes, attitudes and behaviours amounting to discrimination, disadvantaging people in ethnic minority groups’ (7). In 1999, the NHS established ‘The National Plan for Action to Tackle Racial Harassment (8)’, and diversity training and equal opportunities (EO) policies have existed for the past 30 years (9).
However, NHS Workforce Race Equality Standard (WRES) data show Black Asian and Minority Ethnic (BAME) staff experiences of harassment and discrimination from colleagues and patients has been increasing since 2016 (2, 10).
An antiracist outlook accepts that racial inequities are rooted in power and policy and works to dismantle systems which have racism embedded within (11). Therefore, an antiracist intervention tackles multiple levels within the system and is “action oriented” (12). We identified a paper reviewing antiracist interventions in outpatient healthcare settings which presented a conceptual model for implementing anti-racism interventions in healthcare at the personal or institutional level (see Figure 1) (13). Publications in recent years that focus on antiracist interventions in a healthcare setting include opinion pieces (14-19), literature reviews (9, 20-24) or studies focussed on patients (13, 25-27). Currently, there is no systematic review assessing the effectiveness of antiracist interventions for healthcare staff.

Adapted conceptual model for implementing anti-racist interventions in healthcare (13).
Our aim was to conduct a systematic review and describe the effectiveness of antiracist interventions for healthcare staff. Our objectives included:
Identifying interventions addressing racism in healthcare systems in ‘Organization for Economic Cooperation Development’ (OECD) countries
Classifying the interventions level based on our adapted conceptual model for implementing anti-racist interventions in healthcare (Figure 1)
Evaluating the effectiveness of these interventions; and
Methods
This review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (28), following the framework outlined in the Cochrane Handbook for Systematic Reviews of Interventions (29). Stakeholders from the General Medical Council (KL, BL) and Health Education Improvement Wales (CP, RJ) supported the project and assisted with clarification of terminology, protocol planning, review progress meetings and dissemination of findings. Four meeting were held from July 2021 to April 2022.
Eligibility criteria
We developed the eligibility criteria (Table 2) in consultation with the stakeholders and the supervisors. As this is the first review focussed on antiracist interventions for healthcare staff, the population, outcome and study design criteria were purposefully broad to map all available evidence. Only evaluated interventions were included as the research question was focused on effectiveness.
Search Strategy
We developed the search strategy in consultation with information scientists (DM, EG), project supervisors (AC, MG, AE and HP) and stakeholders (KL, BL, CP, RJ). Search terms used key concepts from the research question: ‘racism’, ‘healthcare staff’ and ‘ethnic minority groups’ (found in supplementary material). No restrictions were placed on publication date and non-English language studies were excluded.
Data sources
Databases searched were Medline via OVID, Ovid Emcare, PsycINFO, CINAHL, Web of science, AMED from 25th– 31st January 2022.
Selection process
Both title and abstract and full text screening had 20% dual screened by another reviewer (TA) as per the Cochrane rapid review guidelines (30). Any uncertainty about paper inclusion was discussed with the co-authors (AC, MG, HP). Aside from searching the databases, citation searching of relevant papers was undertaken. The final included papers were exported to Microsoft Excel spreadsheets for data extraction.
Data analysis
The included studies were mapped onto the conceptual model to categorise whether they targeted the institutional or personal racism level.
Critical appraisal
Most of the studies did not use robust analytic study designs, hindering the selection of an appropriate critical appraisal checklist. Study descriptors were assigned, based on the closest match, using an algorithm for assessing appropriate research design as the authors’ descriptors were unclear (31).
Eight studies were appraised using a quality assessment tool for before-after (pre-post) studies with no control group developed by the National Heart, Lungs and Blood Institute (NHLBI) (32). These study designs were unclear and the algorithm identified them as repeat cross-sectional pre-post non-intervention, making the NHLBI checklist the most appropriate. One further study was appraised using the NHLBI non experimental cross-sectional checklist (32). Three qualitative papers were appraised using the Joanna Briggs Institute (JBI) qualitative checklist (33) and one using the JBI checklist for quasi-experimental studies (34). The mixed methods appraisal tool (MMAT) was used for three mixed-methods studies (35).
Results
Six databases identified 2122 records with 600 duplicates removed. The remaining 1522 records were title and abstract screened, of these 103 were full text screened for eligibility. An additional three papers were identified from citation tracking (see Figure 2). A total of 16 studies was included: qualitative (n=3), quasi-experimental (n=1), mixed methods (n=3) and observational (n=9). Countries included the USA (n=11), Canada (n=1) and the UK (n=4). Most evaluated interventions were aimed at the personally mediated level (n=9), with some multilevel (n=4) and institutional (n=3), based on the adapted model.

PRISMA Flowchart
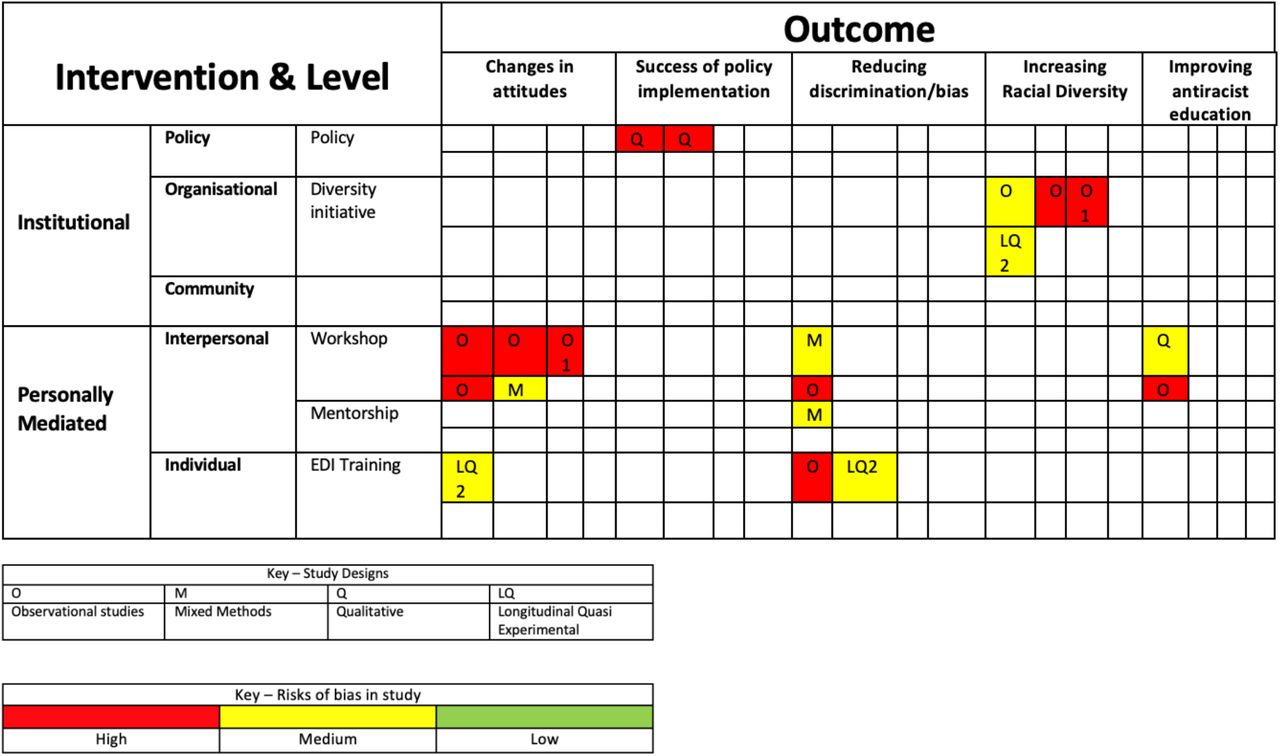
Study designs and risk of bias tools indicated that the quality of evidence was of low quality. Only two studies included control groups (36, 37). Most studies could not confidently attribute positive outcomes to the intervention and the results had limited transferability due to small sample sizes. Both qualitative papers examining the success of policy implementation had high risks of bias; the methodology was unclear and neither study acknowledged the researcher’s role. Figure 3 highlights the lack of evaluated institutional antiracist interventions with no interventions identified at a community level.

{kind=link}
{kind=link}
{kind=link}
Evidence Map of intervention type, study design and outcomes
Institutional Interventions
One paper assessing increasing diversity initiatives (38) and two papers evaluating the effectiveness of policies regarding equal opportunities and ethnic diversity respectively (39, 40) were reviewed.
Diversity Initiatives
In 2019, Wusu et al published an American observational study aiming to increase underrepresented minority (URM) physicians in a residency programme (38). The interventions included: outreach to URM candidates, revising interviews to minimise bias and ongoing analysis of recruitment data. The study ran from 2014-2017 and URM applicants increased by 80%, a statistically significant increase (P<0.001). However, there was no control group and limited generalisability as it was one family medicine programme in Boston. The positive results cannot be solely attributed to the intervention as this study design was low quality with high risk of bias.
Policy Evaluation
There were two papers that evaluated policy. However, both were over 20 years old and did not follow formal qualitative research methodology, therefore these were at risk of bias.
The evaluation of the equal opportunity policy was conducted by interviews with 50 ethnic minority staff and 22 managers at one NHS institution in 1999 (39). The interviews demonstrated the managers lacked knowledge about EO policy and procedures. Despite them all being responsible, only six could identify an EO policy. None received EO training before their role which was attributed to ‘the urgent driving out the important,’ as there were other priorities. Staff interviews highlighted the meaning of EO policies differed between the groups; staff understanding of EO policies centred on career development and promotion, whereas managers focused on recruitment. The paper suggested that these contrasting views may contribute to the disproportionate presence of ethnic minorities in lower grade jobs.
In 2004, the perceptions of ethnic diversity policy in the NHS were evaluated through a mixed methods qualitative and quantitative study (40). A mail survey of every NHS trust was sent out with a response rate of 58% and 32 semi-structured interviews were conducted at a hospital in the south-west of England with employees in charge of employment decisions. Greater diversity was linked to enhanced working relationships and staff perceived an improved service quality. Staff recognised that ethnic minority groups are confined to the lowest paid jobs and that the ultimate goal of ethnic diversity policy should be diversification of senior NHS policymakers as they ‘set the culture of the organisation.’ Staff were supportive of the principles of ethnic diversity policy but unsure how it translates to practice.
Personally mediated Interventions
Of the nine personally mediated interventions, eight were workshops and one was a mentorship scheme. Three workshops had supplementary adjuncts, such as drama teaching.
Singular Workshops
Six discussion-based workshops followed similar structures of a lecture about the topic then group work. One was UK-based (41), one from Canada (42) and four from the US (43-46). The participant numbers varied and were based on opportunistic sampling.
Workshop topics included: racial harassment, microaggressions, cultural competency, equity and inclusion and implicit bias. They all reported positive responses from post intervention surveys. Participants reported improved knowledge and understanding of anti-racist strategies (42, 45). Four papers highlighted knowledge gaps that require ongoing antiracist education – not single workshops (41, 43, 46, 47). They all employed basic study designs with no control group or long-term follow-up. Bheenuck et al recognised this and recommended future research should assess intervention sustainability (41).
Two studies conducted in 2010 and 2021 respectively reported that the interventions were not entirely successful. In Steed’s 2010 mixed methods qualitative and quantitative study, 13 white female occupational therapists, based in Louisiana, participated in a six-hour cultural competency workshop which aimed to reduce racial bias (46). Their attitudes were measured pre- and post-intervention using the racial arguments scale (RAS) and racial attitudes implicit association test (RAIAT). The workshop produced no significant change in racial attitudes. It was noted that the group held strong negative attitudes towards African Americans in the pre-intervention tests (46). These results suggest individuals with negative views require a different approach and may benefit from longer duration projects. However, the wider generalisability is limited due to the small, homogenous sample.
In 2020, an observational study testing the effect of active learning workshops on reducing implicit bias was evaluated on 137 first year American medical students (44). The Implicit Association Test (IAT) was used pre- and post-intervention to measure the students’ bias. The workshop success differed among racial groups. White students showed positive pre- and post-workshop changes yet Southeast Asian and Asian American students did not show a significant reduction in implicit stereotyping (44). The results suggests that antiracism interventions may need to be adapted for individuals’ backgrounds. It is important to note that the IAT is not a validated tool for measuring implicit bias and for first time users, the reliability is much lower due to unfamiliarity (48), therefore this may have affected the results.
Workshops with Adjuncts
Supplemented workshops included a virtual reality experience (49), an interactive map charting locations representing systemic racism in the US (47) and dramaturgical teaching (43). The virtual reality session reported positive outcomes with 94.7% of participants agreeing it was a useful tool for enhancing empathy. The interactive map of racism was acknowledged as a ‘powerful tool’ that improves awareness and shows systemic racism is undeniable. Re-enactment of racial harassment and discussion of how to handle these situations led to positive responses, 100% of participants reported increased confidence in initiating conversations about race.
Mentorship scheme
Naidoo’s 2021 mixed methods qualitative and quantitative study piloted a mentorship scheme for eight ethnic minority physical therapy students in the USA (36). The scheme reduced social isolation and improved socialisation into the physical therapy career. The mentoring faculty reported increases in their cross cultural capital and professional growth (36). The study was robustly conducted but had a small sample size and impact on academic performance was not recorded.
Multilevel Interventions
King et al’s 2012 non-experimental cross-sectional study assessed whether diversity training reduces ethnic discrimination at individual and organisational levels through national surveys in the UK. The research highlighted that training method and content varies between NHS trusts, despite NHS guidance, and diversity training reduces the likelihood of discrimination and organisations can benefit from effective diversity programmes (50). However, the study methodology was poor with risks of bias.
Robinett et al conducted an observational study from 2017-2019 to mitigate bias in US medical school admissions. Interventions targeting the interview process and admissions team were assessed including: interviewer unconscious bias training, focused recruitment strategies and increased diversity on the admissions committee. There was an increase in underrepresented minority (URM) applicants accepted each year, in 2019 27.7% of accepted applicants identified as URM, compared to 49.3% in 2020 (51). The greatest impact was noted after they implemented a multilevel approach, as initially they only held unconscious bias training for the interviewers. Guh et al conducted a similar observational study looking at increasing racial diversity in a US residency programme. The interventions targeted the admissions team and included changes in interview scoring rubrics, targeted recruitment and a race and medicine workshop exploring bias and privilege. The study ran from 2014 to 2018 and resulted in a 19% increase in faculty and 40% increase in residents identifying as URMs (52). However, both papers are low quality, with high risks of bias.
Weech et al’s pre-post quasi-experimental study assessing the impact of a multifaceted cultural competency initiative on hospital performance metrics was the highest quality included paper. This was one of two studies with a control group. Four hospitals participated in the study over a 3.5 years period; two served as the control group and the others implemented the intervention. At an organisational level, focus was on improving diversity leadership, strategic human resource management, and patient cultural competency. At an individual level, the intervention targeted diversity attitudes, implicit bias, and racial/ethnic identity status. For the organisational and individual outcomes, hospitals with the interventions outperformed the control groups in both (37). The organisational outcome for increasing diversity in leadership was measured by Diversity Leadership and Cultural Competence Assessment and the Cultural Competency Assessment Tool for Hospitals (CCATH) and intervention hospitals experienced higher changes in scores. The individual outcome for reduction of implicit bias was measured by the Implicit Association Test (IAT) and found greater reduction in the intervention hospitals. Specific figures were not given for outcomes, limiting the quality of the paper as raw data are not available. The results show that a systems approach is effective at creating change in diversity and cultural competence practices in hospitals.
Discussion
Summary of main findings
This review of the international literature from 1970 to 2022, highlights an evidence gap for the effectiveness of antiracist interventions for healthcare staff, especially at an institutional level. Included studies were of poor quality, lacked long-term data and only four were from the UK. Most interventions focused on the personally mediated level (n=9) and were workshop based (n=8). All the personally mediated and multilevel interventions reported positive outcomes based on their interventions, however due to the poor methodological quality the results are not robust. Three studies assessed the effectiveness of institutional interventions with some indication that a diversity initiative could be successful though data were dated.
Strengths and limitations
This is the first review examining antiracist interventions for healthcare staff in OECD countries. The protocol was published on PROSPERO, the papers were critically appraised using the most appropriate checklists and seven databases were systematically searched. The search was conducted following the Cochrane guidelines and in consultation with information scientists. Stakeholders supported the process to help interpret and validate findings.
Only 20% of the title and abstract screening was double reviewed, however this is in line with rapid review guidance (30). Citation searching was not extensive and there are risks of publication bias as no grey literature was included. The studies included were all low quality therefore knowledge about intervention effectiveness is inconclusive.
Comparison with the literature
In 2021, NHS England published “Making antiracism a reality” where ‘diversity initiatives’ and ‘mentorship schemes’ were listed as interventions, however this review has shown that the evidence base behind them is poor (53). Multiple literature reviews have noted the inconsistencies between formal policies and their effective implementation (9, 21). In 1984, the Commission for Racial Equality (CRE) released guidelines about good practice for employers and in 1998, NHS trusts were surveyed about the implementation of their racial equality policies. Most had formal equal opportunity policies but only 5% implemented their action plans (9). The problems are ongoing and a survey by the Healthcare Commission in 2006 indicated a suspicion of “widespread non-compliance” across the NHS with regards to race relations legislation (54). This review highlights the need for further research to evaluate the impact of current policies and revise them as necessary.
The above “non-compliance” represents the wider issue for antiracism interventions - there is much information about potential interventions but few evaluated data. Various healthcare organisations, such as Kings Fund, a policy think tank, and the BMA, doctors union, publish reports about racial discrimination listing ‘successful’ interventions but use anecdotal evidence and include no methodology (55, 56).
The overall lack of institutional interventions is a key finding as research on racism often focuses on the interpersonal level with little emphasis on institutions (57). Racism manifests at different levels and ‘individual behaviour is shaped by organisational culture and practice’ (58), yet the interventions are disproportionately personally mediated.
Effective antiracist institutional interventions are critical as racism is based on power relationships between dominant and subordinate groups (59). Historical racism, such as colonialism, has shaped modern society and created racial inequities which has bled into our institutions. NHS Workforce Race Equality Standard (WRES) data showed white applicants were 1.46 times more likely to be appointed from shortlisting across all posts, while BAME staff were more likely to be formally disciplined by a factor of 1.22 (2).
The included papers lacked long-term follow-up, therefore it is unclear if the interventions have a continued impact and this requires evaluation. Lai et al examined whether implicit bias interventions had a lasting positive impact on American undergraduate students. While there were immediate positive outcomes the effects diminish over time (60). Furthermore, little is known about behavioural changes outside of the intervention setting (41, 44, 49, 50).
Conclusion
There is a lack of robust evidence for the effectiveness of antiracist interventions targeted at healthcare staff, especially at an institutional level. Research is required to evaluate whether current antiracist policy and practice is effective, especially long-term. The lack of literature from the UK highlights a research gap. Discussions surrounding antiracism in healthcare need to move away from anecdotal evidence and towards high quality, evidence-based interventions which are adopted routinely.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Supplementary Material
Search Strategy
Supplementary material available on request
The data extraction tables are available on request to the corresponding author, Kismet Lalli.
Acknowledgements
The authors would like to acknowledge Rhian Jones and Katie Laugharne for their time, expertise and advice.
References



