
Abstract
Risk-based early detection should be cost effective and widely accessible. EarlyCDT-Lung is a blood-based autoantibody biomarker which may improve accessibility to Low dose CT screening. We randomized 12 208 individuals aged 50-75 at high risk of developing lung cancer to either the test or to standard clinical care. Outcomes were ascertained from Register of Deaths and Cancer Registry. Cox proportional hazards models were used to estimate the hazard ratio of the rate of deaths from all causes and lung cancer. Additional analyses were performed for cases of lung cancer diagnosed within two years of the initial test.
After 5 years 326 lung cancers were detected (2.7% of those enrolled). The total number of deaths reported from all causes in the intervention group was 344 compared to 388 in the control group.
There were 73 lung cancer deaths in the intervention arm and 90 in the controls (Adjusted HR 0.789 (0.636, 0.978). An analysis of cases of lung cancer detected within 2 years of randomization in the intervention group showed that there were 34 deaths from all causes and 29 from lung cancer. In the control group there were 56 deaths with 49 from lung cancer. In those diagnosed with lung cancer within 2 years of randomization the hazard ratio for all cause mortality was 0.615 (0.401,0.942) and for lung cancer 0.598 (0.378, 0.946).
Further large-scale studies of the role of biomarkers to target lung cancer screening, in addition to LDCT, should be undertaken.
Introduction
Lung cancer is commonly diagnosed at a late stage, when five-year mortality rates remain over 90% are unacceptably high.1, 2 To improve the poor prognosis, methods that detect lung cancer at an earlier stage, when it is more likely to be treated with curative intent, are required.3 Following the landmark National Lung Screening Trial, low-dose CT screening has been shown to detect cancers earlier and reduce lung cancer mortality by 20-25%.4, 5,6 The US Preventive Task Force currently recommends annual screening with low-dose CT for adults aged 50 to 80 years who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years.7 However, uptake by the public can be suboptimal because of lack of health insurance or low income, difficulties getting time off work, and low perceived risk . 8, 9, 10 Moreover, the widespread adoption of low-dose CT screening is limited in many health systems by resource constraints, high false positive rates and concerns about overdiagnosis.11,12,13 Consequently, in 2023 the American Lung Association reported less than 5% of eligible individuals in the United States had undergone screening.14 If a more specific, acceptable, less expensive and less resource intensive investigation, such as a biomarker, could precede or accompany imaging, then more people at risk of lung cancer might benefit through better targeted screening or case finding.15, 16
More recent approaches to the evaluation of protein biomarkers emphasise the need to move away from observational studies to trials in complex systems.17 Few blood-based biomarker tests have proceeded beyond the early stages of biomarker evaluation.18,19 The EarlyCDT-Lung Test is an enzyme-linked immunosorbent assay (ELISA) that measures seven autoantibodies, each with individual specificity for the following Tumor Associated Antigens (TAA): p53, NY-ESO-1, CAGE, GBU4-5, HuD, MAGE A4 and SOX2. In cohort studies it demonstrated a specificity of 91% and sensitivity of 41% with better performance in early stage disease.20, 21 It has also been evaluated in the management of pulmonary nodules reporting that a positive EarlyCDTLung in the presence of a lung nodule is associated with a three-fold increase in the likelihood that the nodule is a lung cancer. . 22,23 The ECLS trial was a phase 4 (screening) biomarker evaluation that addressed the question:
‘Does using the EarlyCDT-Lung Test to identify those at high risk of lung cancer and any subsequent CT scanning reduce the incidence of patients with late-stage lung cancer (III & IV) or unclassified presentation (U) at diagnosis, compared with standard clinical practice?’ The main trial reported outcomes after two years, as planned in the power calculation, showing a significant reduction in late stage presentation, with a hazard ratio for stage III/IV presentation of 0.64 (95% CI 0.41–0.99), but no significant difference in lung cancer or all-cause mortality at 2 years follow-up. This paper presents a five year follow up per protocol analysis on lung cancer and all cause mortality.24
METHODS
Study Design and Participants
ECLS was a pragmatic randomized trial involving 12 208 high-risk participants recruited through family practices and community-based recruitment strategies in Scotland. 25 Recruitment occurred between August 2013 and June 2016 with follow up undertaken for 60 months after randomization for each participant. An independent Trial Steering Committee provided trial oversight. This report adheres to the CONSORT Statement and Aarhus guidelines for the reporting of clinical trials and studies on early cancer diagnosis.26,27 The trial design has been published previously.28
Adults aged 50–75 considered at increased risk of developing lung cancer compared to the general population using established recommendations were eligible to participate.29 These were defined as current or former cigarette or tobacco smokers with at least 20 pack-years, or with a history of smoking of less than 20 pack-years plus immediate family history (mother, father, sibling, child) of lung cancer. Potential trial participants were identified from the electronic medical records of family physicians in areas within the most socioeconomically deprived quintile in Scotland, or they self-referred based on a range of advertising methods. Trial participants had no symptoms suggestive of current malignancy, terminal illness, were not taking immunosuppressant therapy, and had an Eastern Cooperative Oncology Group (ECOG) performance status of 0-2 at recruitment.
Randomisation and masking
All participants who gave informed consent provided a blood sample prior to randomisation. Participants were then individually randomised, using the Tayside Randomization System (TRuST) , stratified by recruitment site (Tayside, Glasgow, Lanarkshire) and minimized by age, sex and smoking status. Smoking cessation advice was offered in keeping with NHS Scotland advice. Participants allocated to the intervention arm were tested with the EarlyCDT-Lung test. If this was positive, they received a baseline chest X-ray and chest LDCT-scan followed by 6-monthly LDCT scans up to 24 months post randomisation. Mortality. pathology and tumor staging reports were prepared by independent assessors who were unaware of the allocation status of participants.
Procedures
Images from test-positive participants were reviewed by a panel of experienced thoracic radiologists and respiratory physicians at baseline and every six months afterwards for two years, unless diagnosed with lung cancer before 2 years. These participants were then followed-up within the study or via the Fleischner society guidelines in the NHS care pathway: whichever was most intensive.30 Participants allocated to the control group, and those who were test negative, had no further study investigations and received standard clinical care available in the UK at that time following National guidelines for identification and management of symptoms suggestive of lung cancer.31
Blood samples were processed according to the trial protocol and Standard Operating Procedures, consistent with relevant UK and US guidelines.32 The EarlyCDT-Lung test was performed on 0.5ml plasma samples using a validated method.33 With consent, validated data on cancer occurrence, mortality and comorbidities were obtained from National Services Scotland, which is a high quality health services data repository.34 These were linked and analyzed in the Dundee Health Informatics Centre Safe Haven.35
Staging data were taken from the Scottish Cancer Registry (SMR06). Outcome variables extracted from SMR06 were the first occurrence of all diagnoses starting with the International Statistical Classification of Diseases and Related Health Problems 10th Revision codes (ICD-10) C33 (primary malignant neoplasm of trachea) and C34 (bronchus or lung). Where more than one tumor was present at diagnosis, the most advanced tumor was used for classification of disease. To determine staging, reported clinical and pathological “T, N, M” were used with pathological staging taking precedence when present by National Services Scotland staff blinded to allocation status. Pathology reports for other cancers were reviewed to exclude the possibility that such tumors signified lung metastases from a distant primary. Lung tumor histology was coded in accordance with the Third Edition International Classification of Diseases for Oncology and lung cancer staging was determined using TNM 7th Edition.36,37
Outcomes
The primary analyses compared all-cause and lung cancer specific mortality between the intervention and control groups. The analyses followed the intention to treat principle. Cox proportional hazard models were used to estimate the hazard ratio. One participant who withdrew consent for use of their data in public records (but not baseline data)was excluded from analysis.
The models were adjusted for age, gender, smoking history, and practice. Where models converged, random cluster effects for family practice were included to account for cluster effects. Cox proportional hazard models were used to estimate the hazard ratio. An analysis of proportional hazards by year was performed to test the validity of the model.
Similar methodology was used to analyze the secondary outcomes of mortality rates. . Further analysis compared the outcomes of those in the intervention group and those in the control group diagnosed with lung cancer within 2 years of the test - i.e. lung cancers diagnosed within the timescale of the primary endpoint (i.e. reduction in late stage disease at 2 years from randomisation). Comparisons of proportions were carried out using Fisher’s exact test due to the small number of events. Poisson regression models, (adjusting for follow up time when necessary) were used to investigate other clinical outcomes.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report
RESULTS
Characteristics of the participants
77 077 invitation letters were sent to people fulfilling the record search criteria from 166 family practices and 16 268 responded (21.1%). An additional 2 389 potential participants in the three participating health boards self-referred in response to advertising or word of mouth. 12 241 were invited to an in-person screening appointment, and 12 215 were randomised, 6 were then excluded for the reasons in the CONSORT diagram and one person withdrew their consent, leaving 12,208 for the analysis. The recruitment rate of people identified as potential study participants from family practice records was 13.4% (10 352/77 077); and the recruitment rate from self-referral was 79.1% (1 889/2 389). Participant characteristics were balanced between the intervention and control groups (Table 1). 28.5% (3 477/12 208) of participants lived in the most deprived quintile, the mean age at recruitment was 60.5 years (S.D. 6.58), and the mean pack years smoked was 38.2 (S.D. 18.58).
The CONSORT flowchart (Figure 1) demonstrates 99.9% end-point ascertainment in the intervention and control groups. The CONSORT statement is available in Appendix 1. Follow-up was performed using a national, closed administrative data system for five years or to death if within the follow-up period. We also checked national prescribing, and in- and out-patient data systems for activity relating to trial participants in the five-year follow-up period.

Consort diagram
The results of all-cause and lung cancer mortality analyses are presented in Table 2a and Figures 2a and 2b. There were 344(5.7%) all cause deaths in the test group compared to 388(6.3%) from all causes in the group not tested 5 years post-randomization. There were 73 lung cancer deaths (1.2%) in the group tested and 90(1.5%) in the control group. These differences were not statistically significant.

All cause mortality

Lung cancer mortality
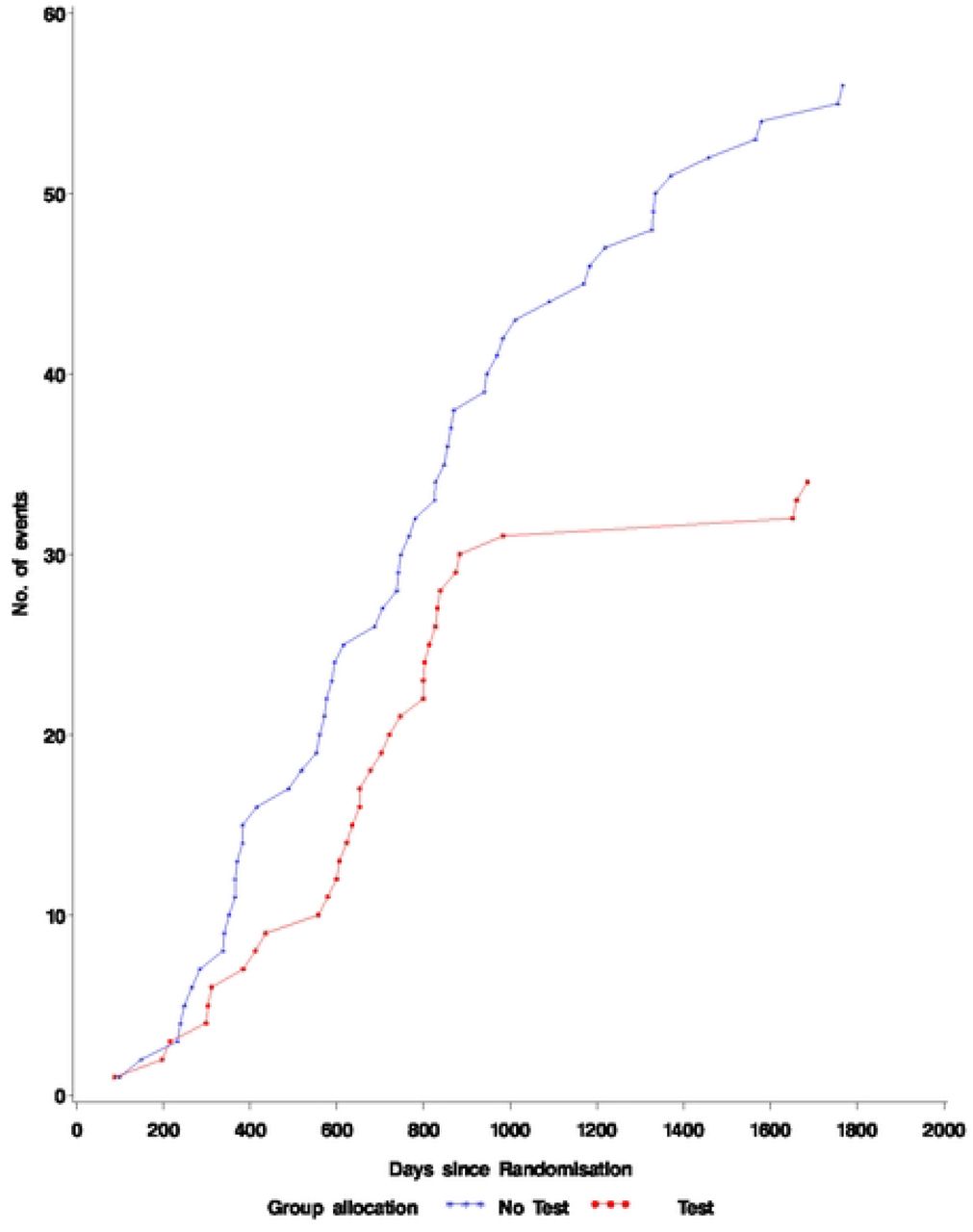
The results for those diagnosed within two years of randomisation are shown in Table 2b and Figures 3a and 3b. There were 34 all-cause deaths (0.6%) and 29 lung cancer deaths (0.5%) in the group who were tested compared to 56 all-cause deaths (0.9%) and 49 lung cancer deaths (0.8%) in the group not tested. When adjusted for age, gender, smoking history, and practice the hazard ratio for all-cause mortality is 0.610 (0.398-0.934) and for lung cancer the hazard ratio is 0.598 (0.378, 0.946) i.e. in the 10% of people who tested positive and were then diagnosed within two years. There was a significant reduction in the hazard of lung cancer death .

All cause mortality in patients diagnosed with lung cancer within 2 years of blood test

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lung Ca mortality in patients diagnosed within 2 years
DISCUSSION
We have presented five-year follow-up data from an RCT comparing a single autoantibody test (EarlyCDT-Lung) compared to standard clinical practice over five years in a pragmatic study design. The main findings are that, after five years, all cause and lung-cancer specific mortality are significantly reduced in patients tested for autoantibodies and diagnosed within two years of the test. The autoantibodies detected by EarlyCDT-Lung are potentially most valuable for detecting early-stage disease in the first year or two after testing and the cancers detected in this study were mainly early stage when patients were able to benefit from recent advances in the management of early stage lung cancer. 38 (Appendix 2).
The 2 year data from this study demonstrated that EarlyCDT-Lung test had an estimated sensitivity of 52.2% (95% CI 30.6–73.2%) for stage I/II disease and 18.2% (95% CI 7.0–35.5%) for stage III/IV disease, and specificity of 90.3% (95% CI 89.6–91.1%) for stage I/II disease and 90.2% (95% CI 89.4– 91.0%) for stage III/IV disease. The positive predictive value was 2.0% (95% CI 1.0–3.5%) for stage I/II disease and 1.0% (95% CI 0.4–2.2%) for stage III/IV disease, and the negative predictive value was 99.8% (95% CI 99.6–99.9%) for stage I/II disease and 99.5% (95% CI 99.3–99.7%) for stage III/IV disease in the population studied.
The cost of the EarlyCDT-Lung test (for 2021/22 costs) was approximately £110 and the National Health Service costs for a LDCT (scan one area) is £95. There is little difference between these costs and it is possible that with a widespread roll out of the EarlyCDT-Lung test it would be possible to negotiate a reduction in the test cost. The costs of these two screening methods need to be considered in the context of capacity issues in healthcare services, particularly in UK National Health Service; rolling out LDCT is more resource intensive than a blood test. Finally, during the study, lung cancer participants in the test arm were typically diagnosed at an earlier stage of lung cancer which is less costly to treat than lung cancer diagnosed at a later stage. Although the test has a marginally larger upfront cost than LDCT, by identifying lung cancer at an earlier stage there are smaller costs for treatment in the future.
Trials based in the community which are open to a more representative sample of the population are likely to provide results which are more generalisable than those conducted in hospital based studies.31 In particular, we recruited a high proportion of participants from the two most socioeconomically deprived quintiles (51.8%) a population shown to engage less with lung cancer screening, integration with a national health care system providing whole population care National data linkage enabled a high end-point ascertainment rate (99.9%), and the intention to treat analysis. In addition, the test being investigated (an ELISA) can be performed at relatively low cost in many laboratories, including in countries where low-dose CT scans are scarce or distributed unequally, increasing the potential for future implementation.
Limitations
The lung cancer diagnosis rate (2.7%) was lower than we anticipated when planning the study. 32 A potential contributor to this may be the “healthy volunteer” effect, which may have led to a higher rate of recruitment of the healthiest among the high-risk population meeting our inclusion criteria.33, 39 This is a challenge shared by all research that requires participants to volunteer and provide consent. It is worth noting that even with a lower rate of lung cancer, those in the intervention group were at a statistically significant and clinically important reduced risk of late-stage presentation.
The comparator arm used in this RCT, namely awaiting the development of symptoms, is no longer standard clinical practice. Although this does not yet constitute a ‘standard of care’ many professional organizations recommend that individuals at high risk for lung cancer (i.e. the targeted population in this RCT) should be screened using LDCT if they are potential candidates for curative-intent therapy rather than being observed for the development of symptoms. This situation lowers the clinical impact of the results. A control arm involving CT screening would have provided evidence comparing USPSTF guidelines against a ‘biomarker first’ approach, but this was not available when the ECLS trial started and it is still unavailable in many health systems.40 We plan a ten year follow up and a cost-effectiveness analysis employing a model to link the short-term outcomes measured within the trial to potential longer-term impacts on health related to morbidity and mortality of early detection and treatment, to allow the estimation of cost-per Quality Adjusted Life Years gained.
Blood tests or other biomarkers could substantially reduce the number of people requiring imaging investigations depending upon where the cut-off for sensitivity and specificity is set. This may have globally significant implications for case finding and screening for lung cancer in people at high risk of the disease.36 Whether blood based biomarkers should be used in screening, case-finding, or to identify individuals at increased biological risk who might be considered in future prevention approaches, requires further elucidation.37
The high specificity of the EarlyCDT-Lung test could be used in combination (concurrently or sequentially) with low-dose CT, which demonstrates high sensitivity, to ensure a high detection rate of early lung cancer cases: a previous report showed that the EarlyCDT-Lung test enhanced the positive predictive power of CT scan and nodule-based risk models for the detection of lung cancer.35 A highly specific non-invasive investigation to confirm or clarify pathology would also be of significant clinical benefit for often elderly patients with small volume disease for whom obtaining tissue is challenging.41
Conclusions
ECLS demonstrates that a blood-based panel of autoantibodies, as in the EarlyCDT-Lung test, may have an important role in future lung cancer screening programmes. The trial provides proof of concept and clinical utility that blood testing in combination with optimal selection of high-risk people and imaging can find cancers at the earliest stages when they are most amenable to cure. Further investigation in large, community-based phase V studies are needed to determine the long-term impact of performing the EarlyCDT-Lung test on mortality; cost-effectiveness, the level of risk that should be targeted; the optimal time interval between tests, and how to improve the engagement of patients at the highest risk.38
Data Availability
Data can be accessed by applying to the ECLS data access committee on tehy template provided at https://eclsstudy.org/request-for-samples-and-data/
References



