
Abstract
Background The dietary pattern along the downstream of the Yangtze River in Eastern China has garnered widespread attention for its potential health benefits; however, population-based evidence is limited. This study aimed to identify and characterize this dietary pattern, develop a dietary pattern index, and evaluate its associations with adiposity, cardiometabolic diseases, mortality, and gut microbiota.
Methods This study included 8,852 adults aged 18-80 from the WELL-China cohort in Hangzhou, Eastern China, between 2016 to 2019. Dietary intake was assessed using a validated food frequency questionnaire. We adopted K-means clustering to identify the Eastern Diet (EastDiet) pattern within the study population and developed a dietary index to quantify adherence to the EastDiet. Adiposity was characterized by total and regional fat measured via dual-energy x-ray absorptiometry. Incident cardiometabolic diseases were documented through October 2022. In addition, we extrapolated the EastDiet index to a nationwide representative cohort of old individuals, including 13,773 participants of the Chinese Longitudinal Healthy Longevity Survey (CLHLS), followed from 2008 to 2018. Linear regression and Cox proportional models were used to assess the associations of the EastDiet index with the study outcomes.
Results In the WELL-China, we identified an EastDiet pattern emphasizing high consumption of plant-based foods and low consumption of refined grains and red meat, aligning with previously reported healthy eating habits in Eastern China. The EastDiet index was constructed based on intake levels of 12 food groups. Higher EastDiet adherence was significantly associated with lower level of overall adiposity (BMI and body fat percentage) and central adiposity (waist-hip ratio and android-gynoid fat ratio), reduced incident cardiometabolic diseases (HRhigh v.s, low = 0.65, 95% CI: 0.43-0.97), and higher gut microbial diversity and abundance of beneficial genera. In the CLHLS, individuals living in the eastern regions had higher EastDiet index scores compared to other regions of China. Higher EastDiet adherence was also associated with decreased mortality.
Conclusion Higher adherence to the EastDiet was associated with more favorable cardiometabolic outcomes, reduced mortality risk, and improved diversity and taxonomy of gut microbiota. These findings support that the EastDiet identified in this study, could be considered an important healthy dietary pattern for Chinese adults.
Introduction
Dietary patterns, reflecting the habitual combinations of foods consumed over time, are critical determinants of global health and well-being.1 These patterns, which include the complex interactions and synergies among various dietary components, provide a holistic view of nutrition beyond the scope of single nutrients or foods.2, 3 In China, there has been a shift from traditional diets rich in whole grains and vegetables to those higher in fats and energy, a transition associated with the rising prevalence of chronic metabolic disorders.4-6 With China having over one-sixth of the world’s population, the discovery of a habitually healthy diet in China has significant implications for public health worldwide.
Intriguingly, regions such as the Yangtze River Delta on the east coast of China exhibit higher average life expectancies and lower rates of obesity and cardiovascular events compared to other regions of the country, particularly northern China.7, 8 This observation suggests that regional dietary habits might influence health outcomes.9 The dietary pattern of the Yangtze River Delta on the east coast of China, characterized by a high intake of vegetables, fruits, aquatic products, soy products, and dairy products, has recently been highlighted as a potential model for healthful eating across China.5, 10 However, this dietary pattern has not yet been identified and lacks empirical evidences for its purported health benefits.
Thus, in this study, our first objective is to apply an unsupervised clustering analysis to dietary data from a large population-based cohort in Hangzhou, located within the Yangtze River Delta in eastern China, to identify and define a healthy dietary pattern specific to this region. Our secondary objective is to develop a dietary index based on this pattern and assess its associations with adiposity, cardiometabolic diseases and gut microbiota. Our final objective is to extrapolated this dietary index to a nationwide representative cohort and investigate its association with all-cause mortality.
Methods
Study Population
The present study employed the WELL-China cohort, a population-based prospective cohort, which enrolled 10,268 residents aged 18-80 years from three districts of Hangzhou, Zhejiang Province, China, between 2016 to 2019.11 We excluded participants with incomplete or illogical food frequency questionnaire (FFQ), those with self-reported cancer and/or gastrointestinal disease, and those with implausible energy intake (<800 or >4,000 kcal/day for males, <500 or >3,500 kcal/day for female). This resulted in 8,852 eligible participants for analysis. Additionally, participants without fecal samples were excluded, leaving 6,193 participants for gut microbial analysis. The flowchart of study selection is presented in Figure S1. The WELL-China study was approved by the Institutional Review Boards of Zhejiang University, Hangzhou, China, and Stanford University, CA, USA. Written informed consent was obtained from all participants.
Dietary Assessment and Measurement of Other Variables
Dietary information was assessed using a validated semi-quantitative FFQ comprising 26 commonly consumed food items in China.11 Participants reported the frequency and average amount of each food/beverage consumed over the past 12 months. Detailed descriptions of the FFQ have been published elsewhere.12 Referring to prior studies, nutritional data were presented as the energy contribution of each food item in this study.12, 13
Participant characteristics were collected through structured questionnaires in face-to-face interviews. Educational status was categorized into three levels: elementary (illiterate and primary school), secondary (junior high school, high school, and professional college), and higher (university and beyond). Alcohol consumption was categorized as non-drinkers and current drinkers. Smoking status was categorized as non-smoker, former smoker, and current smoker. Physical activity was evaluated using the International Physical Activity Questionnaire-Short Form and classified into low, moderate, and high levels.14 Antibiotic use was defined as described according to previous study.15 Medication use was defined as self-reported use of hypertension, dyslipidemia, and/or type 2 diabetes medications.
Fasting venous blood samples (12 hours) were collected on the same day as the questionnaires, processed, and stored at -80°C. They were then tested to assess fasting blood glucose, triglycerides, and other indicators.
Identification of Dietary Patterns
We derived the dietary patterns using the unsupervised K-means clustering analysis on standardized dietary intake data (percentage of energy contribution of each food item). The optimal number of clusters was determined using the NbClust function. We grouped the 26 food items obtained from the FFQ into 17 food groups based on similarities in nutrient sources or habitual practices.
Development of the Eastern Diet Index
After identifying one dietary pattern (Pattern 1) as the Eastern Diet (EastDiet) from the cluster analysis, we developed the EastDiet index to assess adherence to the EastDiet. We created the EastDiet index by selecting 9 healthy food groups significantly higher in Pattern 1, including vegetables, fruits, soy products, aquatic products, dairy products, whole grains, nuts, tubers and roots, and eggs, and three unhealthy food groups significantly lower in Pattern 1, including refined grains, red and processed meat, and deep fried foods (Figure 1). Food groups that were inconsistent with health outcomes in previous studies were not included13. Participants whose energy contribution of each healthy food component was below the median received a value of 0, and those above the median received a value of 116. Conversely, for unhealthy food components, those below the median received a value of 1, and those above received a value of 0. Thus, the EastDiet index ranged from 0 (minimal adherence) to 12 (maximum adherence). The index was divided into three groups: low adherence (0-4), medium adherence (5-7), and high adherence (8-12).

The radar map was created using standardized dietary data, showing the comparison of standardized mean values for 12 food groups between the two dietary patterns.
Measurement of Adiposity-related Phenotypes
Detailed information for measuring weight, height, waist, and hip circumference has been previously described17. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters. Waist to hip ratio (WHR) was calculated as waist circumference divided by hip circumference. Dual-energy x-ray absorptiometry (DXA) was used to measure fat mass in the whole body, trunk, android, gynoid, and leg regions.18 Body fat percentage (BFP) was calculated as whole body fat mass divided by weight. Trunk fat mass percentage (TFP), android fat mass percentage (AFP), gynoid fat mass percentage (GFP), and leg fat mass percentage (LFP) were calculated as a percentage of whole body fat mass. Android to gynoid fat ratio (AOI) was calculated as AFP divided by GFP.
Follow-up for Cardiometabolic Diseases
Incident cases of cardiometabolic diseases, including type 2 diabetes and cardiovascular diseases (ischemic heart disease and stroke),19 were tracked through electronic links to established death and disease registries with unique personal identification numbers. Incident cases were ascertained using The International Classification of Diseases, Tenth Revision (ICD-10): Type 2 diabetes (E11/E14/O24), ischemic heart disease (I20-I25), and stroke (I60-I63). Patients were followed from baseline until the onset of diseases or the end of the study period (October 28, 2022), whichever came first. Participants with a history of type 2 diabetes, ischemic heart disease, and stroke at baseline were excluded from cardiometabolic diseases analysis.
Gut Microbiota Profiling
During the in-person interview, participants were asked to collect fecal samples, which were then store in -80L freezers. The V3-V4 region of the 16S rRNA gene was sequenced using the Illumina HiSeq PE-250 platform (Illumina Inc. USA). Detailed information on DNA extraction and paired-end 16rRNA gene sequencing were described previously. Taxonomic profiles were created using QIIME2.20 Pair-end reads were assembled using the qiime tools import command. The DADA2 pipeline was used to filter low-quality regions of the sequences, marker gene Illumina sequences, and chimeric sequences. Reads were then summarized to amplicon sequence variants (ASV) in a feature table and annotated using the Naïve Bayes classifier trained on the Sliva_132 99% OTUs reference databases.
Extrapolation of the EastDiet Index
To assess the reproducibility of the EastDiet index, we utilized data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), a community-based prospective cohort study initiated in 1998 among older adults in China.21 This study features a nationally representative sample recruited from 23 provinces across China. For our analysis, we used data from the 2008 wave as a baseline, followed up in the 2011, 2014, and 2018 cycles. After applying exclusion criteria, a total of 13,773 participants were included in the analysis (Figure S2). Detailed descriptions can be found in the Supplementary Methods section of the Supplementary Material21-23.
Statistical Analysis
Data were presented as mean (SD) for continuous variables and percentages for categorical variables. In the WELL-China cohort, unsupervised K-means clustering analysis was used to determine dietary patterns. Cross-sectional associations of the EastDiet index with body fat and fat distribution traits were investigated using linear regression, adjusting for age, gender, smoking, alcohol, education, physical activity, and total energy intake. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated to explore prospective associations of the EastDiet index with incident cardiometabolic diseases, type 2 diabetes, and cardiovascular diseases using the Cox proportional regression, adjusting for the aforementioned covariates and BMI.
In gut microbiota analysis, linear regression models were applied to investigate the associations between the EastDiet index and microbial alpha-diversity (at the ASV level), adjusting for age, gender, BMI, smoking, alcohol, education status, physical activity, total energy intake, medication use, and antibiotic use. Alpha-diversity indices were transformed into Z-scores for analysis. To determine taxonomy variation, beta-diversity was calculated based on genus-level Bray-Curtis dissimilarity.
Permutational multivariate analysis of variance (PERMANOVA) was used to investigate microbial community structure across EastDiet adherence levels using the Adonis function with 999 permutations.
For per-taxonomic feature tests, taxa with a prevalence below 10% and a relative abundance below 0.01% were filtered out. The relative abundance of the taxa was transformed using rank-based inverse normal transformation for downstream analysis. MaAsLin 2 was used to explore genera associated with high EastDiet adherence, adjusted for the aforementioned covariates. High-dimensional tests corrected the false discovery rate (FDR) using the Benjamini-Hochberg method with a target FDR of 0.05 considered significant for per-genus tests. To determine whether identified taxonomic features were beneficial to human health, Spearman correlation was used to quantify associations between identified genera and metabolic risk factors, with significance set at 0.05 after the Benjamini-Hochberg correction.
To assess the reproducibility of the EastDiet index, we extrapolated the EastDiet index to the CLHLS, by recalculating the index based on 9 food components. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated to explore prospective associations of the EastDiet index with all-cause mortality using the Cox proportional regression, adjusting for the age, gender, residence, geographic regions, BMI, education, smoking, alcohol, physical activity, and history of cardiometabolic diseases.
All statistical analyses were performed using Stata 15.0 (Stata Corp) and R version 4.2.2. Statistical significance was set at P < 0.05 (two-tailed).
Results
Identification of Dietary Patterns
Among the 8,852 participants from the WELL-China cohort, two distinct dietary patterns were identified (the optimal number was 2) (Table 1). Pattern 1, observed in 48.2% of participants, closely mirrored healthy eating patterns popular for residents in the Yangtze River Delta of eastern China as outlined in the 2022 Dietary Guidelines for Chinese.10 This pattern was characterized by high consumption of vegetables, fruits, soy products, aquatic products, and dairy (Figure 1). Additionally, Pattern 1 captured another 7 recognized characteristics of healthy eating behaviors, including high consumption of whole grains, tubers and roots, eggs, and nuts, alongside low consumption of refined grains, red and processed meat, and deep-fried foods. Nutrient analysis revealed that Pattern 1 had higher protein, fat, and fiber content but lower carbohydrate compared to Pattern 2. Health metrics analysis showed that Pattern 1 had lower BMI, BFP, AFP, WHR, and AOI, and higher LFP and GFP (Table S1). Based on these findings, Pattern 1 was designated as the “Eastern Diet” (EastDiet).
EastDiet Index and Participant Characteristics
Table 2 presents the participants characteristics categorized by EastDiet index levels in the WELL-China. High adherence was associated with older age, female gender, non-smoking, non-alcohol drinking, medication users, lower BMI, higher education, and greater physical activity. In the CLHLS, participants with high adherence had similar characteristics to those in the WELL-China, such as older age and more female gender (Table S2).
In the WELL-China, validation comparing participants born in the Yangtze River Delta with those born in other regions of China demonstrated significantly higher EastDiet index scores (Figure S3). In the CLHLS, further comparing participants from the Yangtze River Delta compared with those from other regions of China also showed significantly higher EastDiet index, which demonstrated the robustness of the EastDiet (Figure S4).
EastDiet Adherence and Adiposity, Incident Cardiometabolic Diseases, Mortality
In the WELL-China, multivariable cross-sectional analyses indicated that high adherence to EastDiet was significantly associated with lower measures of total fat (BMI and BFP) and central fat distribution (WHR, AOI, TFP, and AFP), as well as higher GFP, compared to low adherence (all P <0.05) (Table 3). High EastDiet adherence was also significantly associated with lower blood pressure, fasting blood glucose and triglycerides levels (all P <0.05) (Supplementary Table 3).
Over a median follow-up of 4.6 years, 192 cases of cardiometabolic diseases were recorded. After multivariable adjustment, high EastDiet adherence was significantly associated with a reduced incidence of overall cardiometabolic diseases (Table 4). HRs (95% CIs) were 0.65 (0.43, 0.97) for the highest vs lowest EastDiet index categories and 0.93 (0.87, 0.99) per 1-point increment in the index. Regarding specific diseases, high EastDiet adherence was significantly associated with a 42% reduced incidence of type 2 diabetes. No statistically significant associations were found between the EastDiet index and cardiovascular diseases.
In the CLHLS, during the follow-up period from 2008 to 2018, a total of 9,506 (69.02%) deaths were documented. After multivariable adjustment, high EastDiet adherence was significantly associated with a reduced risk of all-cause mortality (Table 4). HRs (95% CIs) were 0.90 (0.85, 0.96) for the highest vs lowest EastDiet index categories and 0.96 (0.93, 0.98) per 1-point increment in the index.
EastDiet Adherence and Gut Microbiota
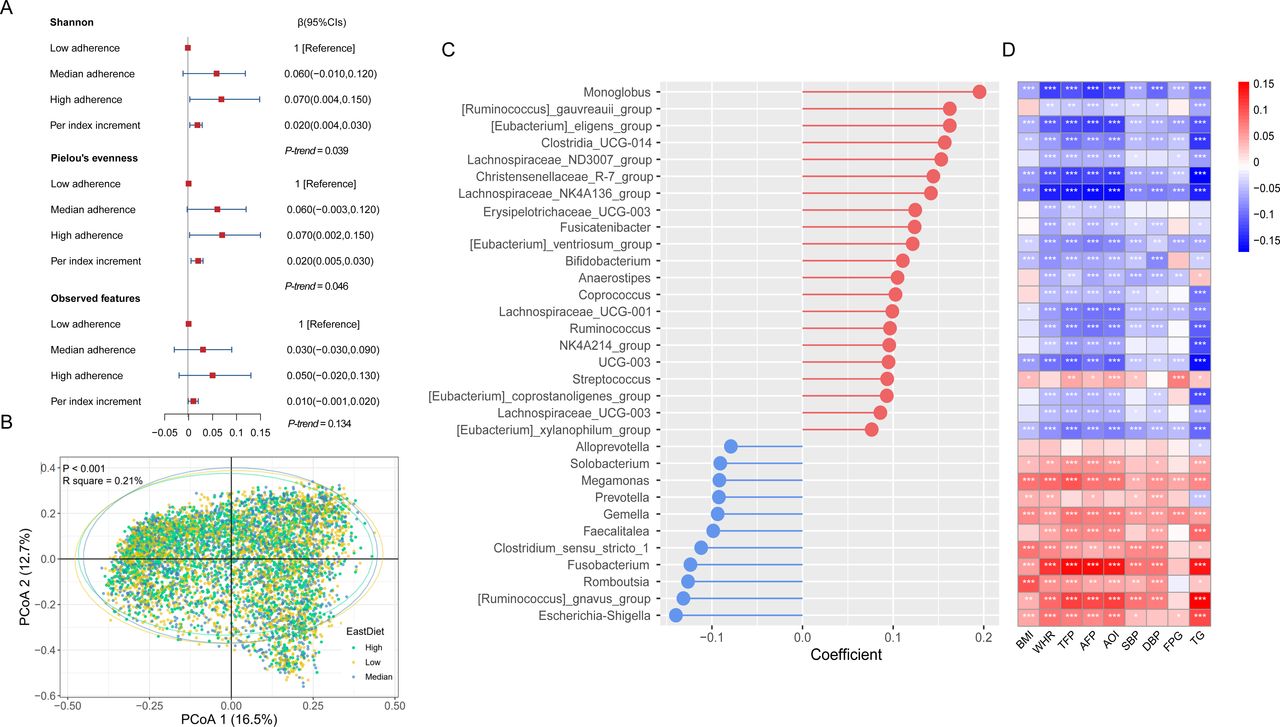
In the WELL-China, multivariable analyses of microbial alpha-diversity indicated that high EastDiet adherence was associated with significantly higher Shannon (P-trend = 0.039) and Pielou’s evenness (P-trend = 0.046) indices compared to low adherence (Figure 2A). Beta-diversity analyses showed significant differences in gut microbial community structure across EastDiet adherence levels (P < 0.001) (Figure 2B). The EastDiet index explained a substantial proportion of the overall gut microbiota structural variations (Adonis R2 = 0.21%).

{kind=link}
{kind=link}
A. Multivariable linear regression was used to estimate the associations of the EastDiet index with alpha-diversity metrics. B. A PERMANOVA test (999 permutations) was used to estimate the proportion of variation in gut taxonomy by the EastDiet. Principal coordinates analysis (PCoA) based on Bray-Curtis distance was used to estimate the dissimilarity of different levels of the EastDiet index. C. Multivariate Analysis by Linear (MaAsLin) was used to identify the associations of the EastDiet index with specific genera. Covariates included age, sex, BMI, education, smoking status, alcohol consumption, physical activity, total energy intake, medication use, and antibiotic use. D. Spearman correlation was used to estimate the associations of the EastDiet-related genera with obesity and other metabolic risk factors. The false discovery rate (FDR) was adjusted using the Benjamini-Hochberg method. A FDR < 0.05 was considered significant. All significant correlations are marked with an asterisk.
Using MaAsLin 2, we identified 32 significant genus-level taxa associated with high EastDiet adherence (FDR < 0.05) (Figure 2C). Among these, 12 genera belonged to the Lachnospiraceae family. Genera enriched in participants with high EastDiet adherence were predominantly associated with lower BMI, central fat distribution (WHR, TFP, AFP, and AOI), blood pressure, fasting glucose, and triglyceride levels (FDR < 0.05) (Figure 2D). Conversely, genera depleted in participants with high EastDiet adherence showed positive associations with these metabolic risk factors. These findings suggest that taxa associated with high EastDiet adherence may confer metabolic health benefits.
Discussion
In this large-scale, population-based cohort study, we utilized unsupervised clustering to identify and characterize a health-oriented dietary pattern prevalent in the Yangtze River Delta of eastern China, termed it “Eastern Diet” (EastDiet). This pattern is distinguished by its high consumption of plant-based foods and relatively low intake of carbohydrates. For the first time, we defined the components of the EastDiet and developed the EastDiet index. Our analysis revealed that high EastDiet adherence was associated with lower total fat and central fat content in cross-sectional analyses and a reduced risk of developing cardiometabolic diseases in prospective analyses. We also observed favorable associations between EastDiet adherence and gut microbial diversity and taxonomy. Furthermore, applying the EastDiet index to a nationwide cohort of elderly Chinese demonstrated a protective association between the EastDiet and mortality.
China accounts for one-fifths of the global population; however, it lacks a dietary pattern that aligns with its cultural context. Dietary patterns vary dramatically across countries, and generalizing dietary patterns identified in other countries to China is inappropriate.24 Considering the current high and rising incidence of obesity and cardiometabolic diseases in China,25-27 identifying a healthy diet pattern that can be generalized throughout China could serve as a crucial health promotion strategy.
The 2022 Dietary Guidelines for Chinese recommended a prototype healthy diet from China’s eastern coastal regions, characterized by high consumption of vegetables, fruits, aquatic products, soy products, and dairy products.10 However, this recommendation was conceptual and lacked empirical support. This is the first study to empirically define the EastDiet and develop a corresponding index. Utilizing unsupervised clustering, our study not only confirms the consumption of these food groups but also identifies additional healthy eating features within the EastDiet, distinguishing it from traditional Chinese diets known for their high glycemic index.28 For instance, our findings revealed a low intake of deep-fried foods and refined grains, but a high consumption of whole grains and tubers, aligning with some aspects of the Mediterranean diet while emphasizing local dietary practices like increased soy and freshwater product intake.5, 16
We developed the EastDiet index to comprehensively measure dietary quality and composition and generalized it to a nationwide database. This index helps assess adherence to the EastDiet and explore its associations with health outcomes. It can also serve as a useful tool in public health campaigns and interventions aimed at improving diet quality not only in eastern China but also nationwide.
Several healthy eating patterns have been proposed in China based on the Dietary Guidelines for Chinese and the Chinese Diet Pagoda.13, 29, 30 Dissimilarly, the EastDiet is derived from the actual dietary patterns of residents in eastern China. Our data demonstrated that a large proportion of the study population, especially older individuals, already adhered to the EastDiet pattern. We also successfully extrapolated the EastDiet to a nationwide representative dataset and found a trend toward older age in high adherence to the EastDiet. As to China’s population ages rapidly, improving diet quality is particularly important to achieve healthy ageing.31 Thus, our findings have the potential to be generalized to the national population as a dietary approach to improve metabolic health and reduce mortality risk, especially among older adults.
Diet is a key factor in obesity development and high-calorie, poor-quality dietary patterns significantly contribute to weight gain.32 Our data showed an inverse association between EastDiet adherence and whole body fat (BMI and body fat percentage). In line with our findings, a randomized controlled trial of a diet based on Eastern Chinese-style cuisine found that it could achieve weight loss over six months in Chinese adults with pre-diabetes.33 In addition to total fatness, we also found an inverse association between EastDiet index and lower central fat distribution (e.g., WHR and AOI). Given that Chinese people tend to develop more trunk fat for a given BMI compared to non-Hispanic Whites,34 our findings provide evidence on strategies to target abdominal fat accumulation for Chinese people.
The shift in diet pattern in China has led to an increase in type 2 diabetes prevalence.35 Key dietary risk factors fueling this rise include low consumption of whole grains, high intake of refined grains, and insufficient intake of seafood, vegetables, fruits, nuts, and dairy.35 The EastDiet addresses these risk factors, showing a potential relationship between adherence to the EastDiet and a reduced risk of new-onset cardiometabolic disease and type 2 diabetes. This relationship mirrors the protective effects of Mediterranean and plant-based diets against type 2 diabetes,36, 37 supported by the beneficial role of dietary fiber and antioxidants found in plant-based foods in enhancing glycemic control and insulin sensitivity.36, 38
We indicated that high EastDiet adherence promotes the development of beneficial gut microbiota, playing a pivotal role in disease prevention. The influence of dietary patterns on gut microbiota composition is well-documented, and recent studies has underscore the importance of gut microbiota as a marker of dietary quality.39 We observed that the EastDiet enhanced microbial alpha-diversity, aligning with previous research linking high diet quality to high microbial diversity.40, 41 Moreover, the EastDiet significantly influenced microbial structure variation, similar to the effect observed with the Mediterranean diet.16
We identified 32 gut bacterial genera associated with the EastDiet index. Many of them are from the Lachnospiraceae family, known for their role in fiber fermentation and butyrate production, which promote intestinal homeostasis.42, 43 In this study, the abundance of Lachnospiraceae-related genera exhibited beneficial associations with health risk factors such as BMI, central fat content, blood pressure, glucose, and triglyceride levels, suggesting a plausible mediating role of gut microbiota.
Our study has several notable strengths. Firstly, we utilized unsupervised clustering to characterize the EastDiet from the Yangtze River Delta in Eastern China. The pattern determined through these steps is more realistic and reliable because it is not assessed by simply picking out several food items without quantitative evidence. Secondly, we extrapolated the EastDiet index to a nationwide representative dataset to demonstrate the robustness of the EastDiet. Thirdly, we used both cross-sectional and prospective designs to assess the associations between EastDiet and health outcomes. Fourthly, we employed a large-sample gut microbiota data to investigate the associations among EastDiet, gut microbiota, and metabolic risks, providing an in-depth understanding of the EastDiet.
However, our study has several limitations. The lack of repeated dietary assessments is a notable constraint. Additionally, while the food frequency questionnaire used in the WELL-China has undergone validation, it may not capture all aspects of daily energy intake and lacks investigation of condiment use. Furthermore, in the CLHLS, dietary information was collected using non-quantitative dietary questionnaires, and several food groups identified in the WELL-China, including whole grains, tubers and roots, and deep-fried foods, were missing, which limited the ability to assess the EastDiet index.
Conclusion
This study identifies the Eastern Diet, a healthful dietary pattern from Eastern China. Our findings underscore the importance of the Eastern Diet, which not only aligns with regional culinary preferences and mitigates cardiometabolic risks but also has protective effects on mortality in a large nationwide dataset. The Eastern Diet highlights its potential to serve as a local reference for daily healthy eating for Chinese people, similar to the Mediterranean diet for Western populations.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Source of Funding
This work was funded by the Amway (China) Fund [519600-I 5210H]; the Nutrilite Health Institute Wellness Fund; the China Medical Board (CMB) [15-216]; the Cyrus Tang Foundation; and the Hsun K. Chou Fund of Zhejiang University Education Foundation [419600-11107].
Disclosures
None.
Acknowledgements
YWS, WH, and SKZ designed the study and were responsible for the manuscript. YWS analyzed data. YWS, JTK, XML, YJ, YFH, QYW, JD, WH, and SKZ wrote the manuscript and created the tables and figures. SKZ supervised the study. All authors contributed to the critical revision of the manuscript for intellectual content. All authors read and revised the manuscript, and approved the final submitted version.
References



