
Abstract
Background There is a genetic component to the QT-interval. This study investigated whether a polygenic risk score for QTc (PRSQTc) could predict ΔQTc and short-term mortality in first-time users of QT-prolonging medications (QTPM) with a known risk of Torsade de Pointes.
Methods First-time users of psychoactive QTPM in the Copenhagen Hospital Biobank and the Danish Blood Donor Study from 2009-2021 were included. ΔQTc was calculated and all-cause 30-day mortality following initiation of treatment was explored. All models were adjusted for conventional QT-prolonging risk factors, and models investigating death were additionally adjusted for potential comorbidity confounders.
Results The PRSQTc could predict ΔQTc (2.88 milliseconds (ms) for every increase of standard deviation in PRSQTc (P <0.001)) following treatment initiation. Individuals in the top ≥ 80 % of PRSQTc had a higher risk of ΔQTc of ≥60 ms compared to individuals in <80 % PRSQTc (OR = 4.88 P = 0.019). Furthermore, the study has also shown that the shorter QTc before initiation of QTPM, the higher the risk of greater ΔQTc.
A high PRSQTc could also predict short-term mortality following treatment initiation: Individuals in the top PRSQTc ≥90 % had an odds ratio of 1.84 (P-value = 0.002) for short-term mortality compared to individuals with PRSQTc <90 %. Individuals in the top PRSQTc ≥99 % had an odds ratio of 4.95 (P-value = 0.009) for short-term mortality compared to individuals in the <99 % PRSQTc
It could be replicated that PRSQTc ≥90 % was a predictor of short-term mortality with OR 1.52 (P-value = 0.002) compared to PRSQTc <90 % in a bigger cohort (N=15.249).
Conclusion PRSQTc seems to be predictive of ΔQTc following initiation of treatment. PRSQTc proves to be a sufficient predictor of 30-day mortality after initiation of QT-prolonging psychoactive drugs with a known risk of Torsade de Pointes.
If used in a clinical setting, PRSQT may help prevent sudden cardiac deaths associated with QTPM.
Introduction
The electrocardiographic QT-interval represents the sum of the ventricular depolarization and repolarization. The QT-interval is clinically important as both a long and a short QT-interval predisposes to ventricular arrhythmias and sudden cardiac death. Many commonly prescribed drugs (QT-prolonging medication, QTPM) may cause QT-interval prolongation and thereby increase the risk of developing Torsade de Pointes (TdP) which predisposes to sudden cardiac death (1–3). Therefore, evaluation of drug-induced QT-prolongation is crucial when developing, testing, and prescribing drugs.
The mechanisms of drug-induced long QT involve the drug’s interaction with several cardiac ion channels, in which the main interaction is a blockade of the rapid potassium current (IKr) encoded by the gene KCNH2. The final manifestation of the drug-ion-channel interactions is a reduction of the net repolarization current in the ventricular action potential, leading to QT-prolongation (4,5). Another important risk factor of QT-prolongation is hypokalemia(6,7). Not all patients develop prolonged QT-interval when exposed to the same QTPM and this variability in response is partly ascribed to genetic factors (8). Indeed, studies show that variants in genes encoding the cardiac channels can modify the drug-channel interaction, resulting in an increase of the binding affinity or the channel gaiting kinetics (9,10). Genome-wide association studies (GWAS) of the QT-interval have been conducted to explain the heritability of the QT-interval in the general population. Studies show that polygenic risk scores calculated based on GWASs of corrected QT-interval (PRSQTc) associate significantly with long QT-syndrome in genotype negative individuals and sudden cardiac death (2,11).
This study hypothesized that PRSQTc may predict the variability in response to QTPM. By designing a case-control study, the aim of the current study was to investigate if individuals in the top quantile of PRSQTc are at greater risk of prolonged QT-interval following initiation of QT-prolonging psychoactive medication with a known risk of TdP. Subsequently, the aim was also to investigate whether individuals belonging in the top quantile of PRSQTc are at greater risk of 30-day-mortality following the initiation.
Methods
Study Design and Population
The study is based on the Copenhagen Hospital Biobank (CHB)(12) initiated in February 2009 and the Danish Blood Donor Study (DBDS)(13) initiated in March 2010. First-time users of psychoactive drugs listed on CredibleMeds (14) as QTPM with a known risk of TdP from 2009-2021 were included. These drugs will hereby be referred to as reference drugs. The following reference drugs were investigated: Citalopram, Haloperidol, Escitalopram, Methadone, Chlorprothixene, Levomepromazine, Pimozide, Sulpiride and Sertindole. For inclusion, the drugs had to be tablets or capsules intended for oral administration.
Twelve lead ECGs were obtained per clinical indication and integrated in the CHB/DBDS environment. Based on the Marquette 12SL algorithm used in the ECGs, ECGs not consistent with a valid measurement of the QT-interval (e.g., branch blocks, atrial fibrillation, bradycardia, see Supplementary for ECG details) were excluded.
Apart from being first-time users of reference drugs, included individuals had to be registered with ECGs with valid measurements of the QT-interval. When exploring the outcome, ΔQTc, individuals had to be registered with at least two valid ECGs: At least one ECG measured within 18 months before the first prescription of the reference drug (baseline-ECG) and at least one ECG measured within 18 months after the first prescription (treatment-ECG). If more than one baseline-ECGs were present, the ECG closest to the date of the first prescription was used. If more than one after-ECGs were present, the ECG closest to day 15 after the first prescription was used. Furthermore, only individuals with after-ECGs, in which the ECG was measured within the treatment period, were included. For more details on calculation of the treatment period, see Supplementary. When investigating short-term mortality, only a valid baseline-ECG was required to be included.
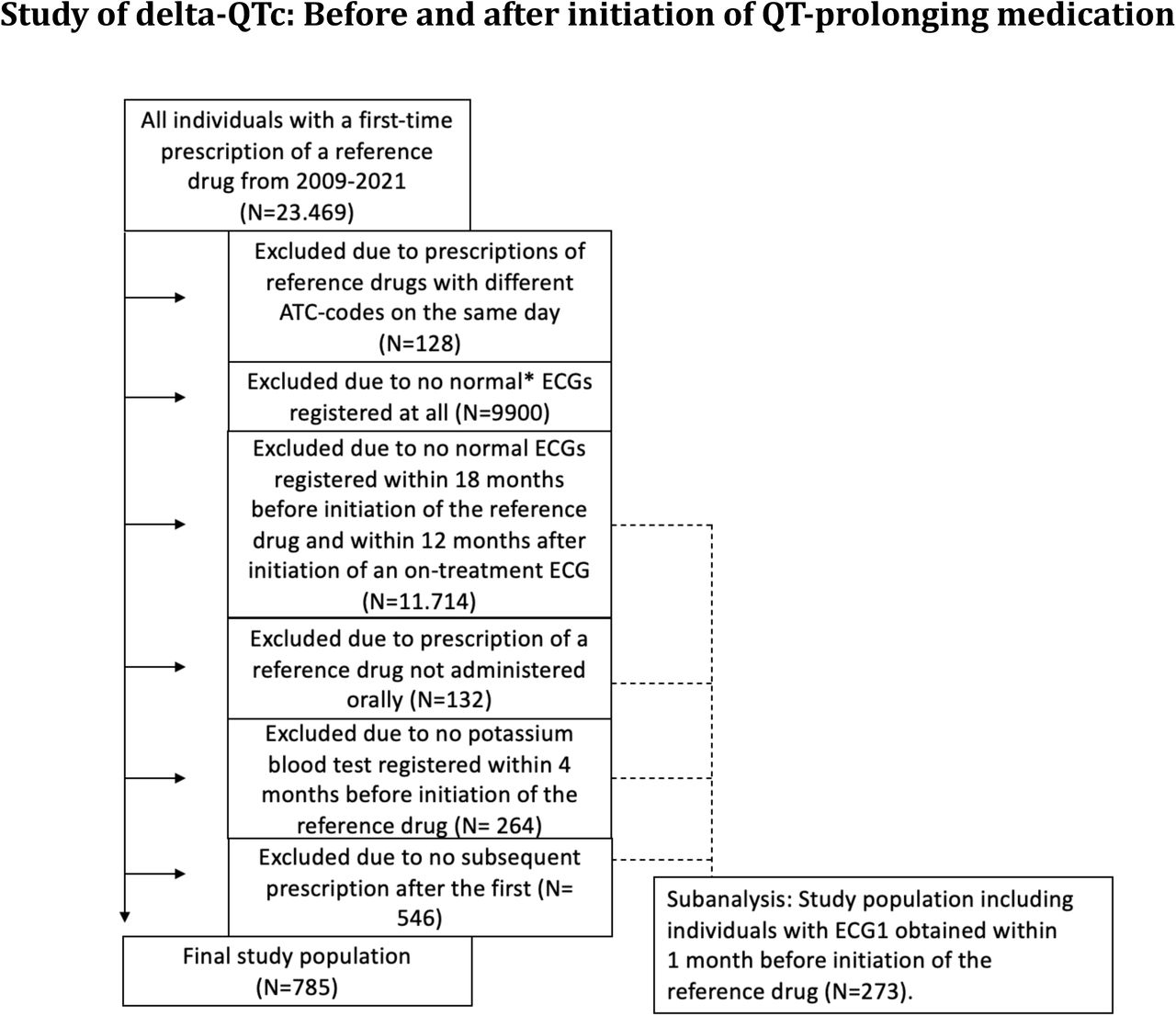
Lastly, using the latest blood test, all included individuals had to be registered with a potassium blood test within 4 months before the first prescription of the reference drug. Figure 1 and Figure 2 illustrate the methods used.

Selection of the study population with a baseline ECG and on-treatment ECG along with a baseline potassium blood test.
*Normal ECG: No presence of atrial Aibrillation/Alutter, right or left bundle branch block, pace rhythms, 2. or 3. degree AV block, premature atrial or ventricular extrasystoles, Wolf-Parkinson-White pattern, or poor-quality data. We additionslly excluded ECGs with a QRS duration >120 ms, bradycardia (heart frequency, <40) or tachycardia (heart frequency, >110). We also excluded extreme outliers based on the following criteria: QTcFridericia (QTcF) <0.1 % of cohort distribution (<320 milliseconds), and QTcF >99.9 % (>614 milliseconds).

Selection of the study population investigating the outcome: On-treatment, 30-day-mortality.
Genetics
GWAS summary statistics on Fridericia-corrected QT-interval (QTcF) from previous published data were queried (15). Using PRS-CS (16), individual polygenic risk in CHB/DBDS was calculated. In CHB/DBDS, individuals were genotyped on Infinium Global Screening Array (Illumina Inc, USA). In sample-wise quality control of CHB/DBDS, samples with missingness < 97%, sex mismatch, genetic ancestry outliers and heterozygosity outliers (>3SD) were removed. In marker-wise QC, variants with missingness < 99%, low Hardy-Weinberg equilibrium (P < 0.0001), and minor allele frequency < 0.1% were removed. Imputed genetic data with an information quality cutoff < 0.9 were used to create genotype files for individuals in CHB/DBDS.
Other covariates
For model adjustment, the following conventional risk factors for prolonged QT-interval were investigated:
Age. Sex. Hypokalemia (plasma-Potassium <3.6 mmol/L). Loop-diuretics or thiazides without potassium: If prescribed within 30 days before prescription of the reference drug had been filled, the individuals were registered as being on diuretic treatment (17).
To explore the additive effect of QTPM on the outcome, it was investigated whether the individuals had a prescription of another QT-prolonging psychoactive medication with a possible risk of Torsade de Pointes according to CredibleMeds (14). The prescription of the other QTPM had to be within 30 days before the prescription of the reference drug. The additional QT-prolonging psychoactive medication could be one of the following drugs: Mirtazapine, Nortriptyline, Misanserine, Fluanxol, Clozapine, Aripiprazole, Perphenazine, Melperone, Maprotiline and Pipamperone.
Models were adjusted for heart failure, using all diagnosis codes for heart failure. When addressing ischemic heart disease (IHD), both disease diagnoses and/or procedure codes involved in ischemic heart diseases were used: Ischemic myocardial infarction diagnoses (IHD) percutaneous coronary intervention or coronary artery bypass grafting (18).
Inhibited drug clearance due to hepatic or renal dysfunction can prolong the QT-interval when exposed to QTPM. Therefore, hepatic or renal insufficiency before prescription of the reference drug was included as a covariate. Diagnosis codes for hepatic failure chronic hepatitis, fibrosis/cirrhosis of the liver, acute kidney failure, chronic kidney disease or unspecified kidney failure were used (19).
For short-term mortality, the models were adjusted for the most common mortality causes in high-income countries: Cancer, IHD, stroke and chronic obstructive pulmonary disease (COPD). Cancer was defined as all cancers except non-malignant melanoma skin cancer. All the used diagnosis and procedure codes had to be registered before the prescription of the reference drug. All the ATC, diagnosis and procedure codes can be found in Supplementary.
Outcomes
The outcome, ΔQTc, was defined as the absolute difference of measured QTcF in treatment-ECG and baseline-ECG. The outcome, ΔQTc, was investigated in a linear regression model adjusted for covariates. The outcome, ΔQTc, was also investigated as a binary outcome in adjusted logistic models, using ΔQTc ≥10 ms, ≥20 ms, ≥30 ms, ≥40 ms, ≥50 ms and ≥60 ms. The binary ΔQTc outcomes were investigated in an interaction analysis, exploring the interaction between PRSQTc and the QTcF in the baseline-ECG.
Short-term mortality was defined as death within 30 days after the first filled prescription of the reference drug. The death had to occur during the treatment period. In addition, only deaths registered to be of natural causes were registered as outcomes, excluding suicides, homicides, accidents, and unknown causes. The decision to use 30-day-mortality as outcome is based on the risk of drug-induced TdP being greatest during the following days after initiation of QTPM (18).
To address ascertainment bias, short-term mortality was tested as outcome in a cohort not limited by the need of ECGs and potassium blood tests prior to initiation of the reference drug. In this cohort, all individuals with the diagnosis atrial fibrillation or atrial flutter were excluded, as atrial fibrillation reduces the likelihood of TdP after initiation of QTPM(20).
Statistics
The case-control association analysis was performed using linear and logistic regression with the generalized linear model (GLM). The results are shown as ΔQTc in milliseconds or odds ratios with belonging confidence intervals and P-values. When calculating statistically significant differences of continuous outcomes in separate groups, the Mann-Whitney U test was used. If the outcomes were binary, Chi-squared test was used. In the latter two tests, only the P-values are shown in this study.
Results
ΔQTc
The cohort exploring the outcome, ΔQTc, consisted of 785 first-time users of QTPM meeting the inclusion criteria. This study found that for every increase in standard deviation (s.d.) of PRSQTc, ΔQTc would increase with 2.88 ms (P <0.001) (table 1 and figure 3).
The absolute delta-QTcF in milliseconds of ECGs measured within 18 months before initiation of QT-prolonging medication and within 12 months after initiation of on-treatment ECG. The inAluence of different QT-prolonging factors on delta-QTcF are shown. The linear model used have additionally been adjusted for PCs 1-10.

Adjusted linear plot showing the absolute delta-QTcF of ECGs measured before and after initiation of QT-prolonging drugs as function of PRSQTc. The plot illustrates the study population in which ECG1 is measured within 18 months before initiation (N=785). ECG2 are on-treatment ECGs obtained within 12 months after initiation of the QT-prolonging drug. The continuous line represents the component plot, and the dashed line represents the residual plot.
The binary traits ΔQTc ≥10 ms, ≥20 ms, ≥30 ms, ≥40 ms, ≥50 ms and ≥60 ms (table 2) were examined. Individuals in the top ≥80 % PRSQTc had greater risk of ΔQTc ≥60 ms compared to individuals with PRSQTc <80 % (OR = 4.88, P = 0.019). Results from the interaction analysis showed that individuals with normal QTc in the baseline-ECG (380-449 ms (M)/390-459 ms (F)) were at greatest risk of higher ΔQTc compared to those with borderline QTc (QTcF 450-496 ms (M)/460-479 ms) or prolonged QTc (470 ms (M)/ ≥ 480 ms (F)) in the baseline-ECG (table).
Results showing the OR of the outcomes, delta-QTc: >=10 ms, >=20 ms, >=30 ms, >=40 ms, >=50 ms and >=60 ms, from logistic models including variables potentially inAluencing delta-QT. All the logistic models used have additionally been adjusted for PCs 1-10.
The study has also shown that the shorter QTc before initiation of QTPM, the higher the risk of greater ΔQTc (figure 4). This is in line with an Icelandic study showing that the shorter QTc before surgery, the higher the risk of greater ΔQTc postoperative (21).

This linear plot illustrates that the shorter QTc before initiation of QT-prolonging drugs, the higher the risk of greater ΔQTc after initiation of treatment.
Short-term mortality
In the studied population consisting of 3001, PRSQTc ≥80 % could predict short-term mortality with OR 1.32 (P-value = 0.089), PRSQTc ≥90 % could predict short-term mortality with OR 1.84 (P-value = 0.002) and PRSQTc ≥99 % could predict short-term mortality with OR 4.95 (P-value = 0.0093) (table 5). All the reported results originate from adjusted models including PCs 1-10, age, sex, heart failure, IHD, loop diuretics/thiazides, additional QTc-prolonging medication, renal insufficiency, hepatic insufficiency, hypokalemia, baseline QTcF, cancer, stroke and COPD.
Analyzing the interaction of PRSQTc >=80 % and intervals of QTcF from ECGs measured within 18 months before initiation, using the binary outcome: Delta-QTc: >=10 ms, >=20 ms, >=30 ms, >=40 ms, >=50 ms and >=60 ms. The ECGs used after initiation have all been on-treatment and within 12 months after initiation. The models have been adjusted for PCs 1-10.
The baseline characteristics of the study population used to calculate OR of 30-day-mortality after initiation of the QT-prolonging medication.
Results of on-treatment, 30-day-mortality in the study population of Airst-time users of QT-prolonging medications. In the logistic models, the risk models in the left column were included. In addition, all the models have been adjusted for PCs 1-10.
Results showing characteristics of the individuals deceased within 30-days after initiation of the QT-prolonging in the study population.
A forest plot showing AUC of the different risk factors for prolonged QTc/mortality is illustrated in figure 5. When analyzing the AUC difference of all risk factors except PRSQTc ≥ 90 % and all risk factors including PRSQTc ≥ 90 %, the difference is statistically significant, though not robust, with a P-value of 0.04.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing the AUC of risk factors for mortality and/or prolonged QT-interval after initiation of QT-prolonging medication. The AUC difference of “All except PRSQTc ≥ 90 %” and “All including PRSQTc ≥ 90 %” is statistically signiAicant, though not robust, with a P-value of 0.04.
This study also found that longer baseline QTcF seems to be protective of 30-day-mortality following initiation of the reference drug: QTcF, OR 0.99 (P-value = 0.0029).
When analyzing the deceased individuals, the ones in the top PRSQTc quantiles are slightly younger than the rest: For instance, individuals belonging to the PRSQTc ≥ 99 %, the mean age at death 64.3 years and individuals belonging to PRSQTc < 99 %, the mean age at death was 74.9 years (P-value = 0.028) (table 7).
Another finding is the increased prevalence of cancer in the top PRSQTc quantiles (table 5): For instance, the prevalence of cancer in PRSQTc ≥80 % is 42.5 % and 33.9 % in the PRSQTc < 80 % group (P-value = 0.0001). In the deceased individuals, cancer was not significantly more prevalent in the top PRSQTc quantiles (table 7).
In the sensitivity analysis without the cohort-limiting factors as baseline ECGs and potassium blood tests, the cohort consisted of 15.675 individuals, and the baseline characteristics are shown in Supplementary, table 1. In adjusted models of the sensitivity analysis, PRSQTc ≥80 % could predict short-term mortality with OR 1.23 (P-value = 0.053), PRSQTc ≥90 % could predict short-term mortality with OR 1.52 (P-value = 0.002) and PRSQTc ≥99 % could predict short-term mortality with OR 1.69 (P-value = 0.12) (table 2 in Supplementary).
When analyzing the deceased in this cohort, it was not observed that the individuals in the top PRSQTc quantiles had lower ages at death (table 3 in Supplementary). When investigating the prevalence of cancer in the top PRSQTc quantiles in this cohort, this study observed increased prevalence in the top quantiles: The prevalence of cancer in PRSQTc ≥80 % is 42.5 % and 33.9 % in the PRSQTc < 80 % group (P-value = 0.0001). In the deceased individuals, cancer was not significantly more prevalent in the top PRSQTc quantiles (table 3, Supplementary).
Discussion
A case-control study investigating whether PRSQTc is of predictive value to the outcome ΔQTc QTc and short-term mortality in first-time users of QT-prolonging psychoactive medication with a known risk of TdP was conducted. This study found that individuals in the top quantiles of PRSQTc may be at risk of greater positive ΔQTc and 30-day-mortality following initiation of treatment.
An abstract presented in the American Heart Association in November 2023 of a prospective cohort study investigating the predictive value of PRSQTc to the outcome delta-QTc in individuals exposed to Sotalol found similar results (22).
It is interesting to discuss the predictive value of PRSQTc in relation to a baseline ECG measured prior to initiation of QTPM. Our results show that the more prolonged the QT-interval is in a baseline ECG, the lower the risk of greater ΔQTc, -0.54 ms (< 1 ∗ 10-4). For instance, for every increase in baseline QTcF, the odds of ≥ 60 ms in ΔQTc decrease by a factor 0.93 (P-value = < 1 ∗ 10-4). This finding prompts that baseline ECGs cannot predict the individuals at risk of greater QT-prolongation when exposed to QTPM. In contrast, when belonging to the top ≥ 80 % in PRSQTc, the odds of ≥ 60 ms in delta-QTcF increase by a factor 4.88 (P-value 0.019). In comparison, when affected by hypokalemia, the odds of ≥ 60 ms in delta-QTcF increase by a factor of 9.38 (P-value = 0.00014).
Results from the interaction analysis show that individuals in the top ≥ 80 % PRSQTc with a normal baseline QTcF were the individuals at greatest risk of positive dΔQTc when exposed to the QT-prolonging psychoactive drugs.
There is no QTc threshold at which TdP is certain to develop, albeit the risk of TdP increases by a twofold to threefold when having a QTc greater than 500 ms. It is also documented that every 10-millisecond increase in QTc, increases the risk of TdP by 5-7 % (23–25).
Based on the results of this study, PRSQTc may be a better predictive tool than the baseline ECG when assessing how an individual will respond to QTPM, especially in individuals with normal baseline QTc.
When stating that PRSQTc may predict 30-day-mortality following initiation of QT-prolonging psychoactive medication, it is important to analyze the baseline characteristics of the studied population. As a baseline ECG and potassium blood test were inclusion criteria in the studied population, most of the individuals originated from the CHB-cohort, which consist of hospitalized patients or outpatients at hospitals. The baseline characteristics of the studied population indicate high frequency of one or more disorders (table 5). This is observed across all PRSQTc groups, though the only variables which are distributed significantly different in the PRSQTc groups are baseline QTcF and cancer: For example, in the group, PRSQTc ≥ 90 %, the mean QTcF was 432.5 ms and the mean QTcF in the <90 % was 420.6ms (P-value= 5.89 ∗ 10-14). The prevalence of cancer in top PRSQTc ≥ 90 % was 43.9 % and in the <90 % group, the prevalence was 34.7 % (P-value = 0.0002). It has not been previously reported that individuals with long QT syndrome are at increased risk of cancer. However, GWASs of the QT-interval typically find common variants in genes regulating ion-channels, calcium-handling proteins and myocyte structure(11,15,26,27). Both ion channels and calcium-handling proteins are important drivers for hallmarks of cancer as proliferation, apoptosis and migration (28–31). As genomic instability is an important feature of cancer, it is plausible that some variants influencing the phenotype of the QT-interval may also influence the risk of cancer.
Though there is an increased prevalence of cancer in the top quantiles in the studied population, there is not a significant increased prevalence of cancer in the top PRSQTc quantiles of the deceased individuals. In models adjusted for all risk factors, PRSQTc ≥ 80 % predicts short-term mortality with OR 1.32 (P-value = 0.089), PRSQTc ≥ 90 % predicts short-term mortality with OR 1.84 (P-value = 0.002) and PRSQTc ≥ 99 % predicts short-term mortality with OR 4.95 (P-value = 0.0093).
In the sensitivity analysis including a younger cohort with fewer counts of disorders, PRSQTc ≥ 90 % could still predict short-term mortality with OR 1.52 (P-value = 0.002).
When finding that PRSQTc may both predict the QTc response and short-term mortality following initiation of QTPM, using PRSQTc as a predictive tool in a clinical setting may help prevent sudden deaths associated with QTPM.
One limitation of this study is the time limit at which the baseline ECG and potassium blood test had to be measured within, as they cannot fully represent the biological conditions in all individuals right before the initiation of the QTPM. Another limitation is that, though, the treatment periods based on the prescriptions were calculated, it cannot be fully validated that the individuals were under influence of the reference drugs when the treatment-ECGs were measured. The main strength of this study is the combination of both clinical, paraclinical and genetic variables in cohorts of reasonable sizes, allowing us to compare baseline ECG and PRSQTc to each other, which has led to one of the novel interesting findings.
In conclusion, this study found that PRSQTc can be predictive of the QTc response following initiation of QT-prolonging psychoactive drugs with a known risk of Torsade de Pointes. PRSQTc might even be a better predictor of the QTc response compared to the baseline ECG. This study also found that PRSQTc could predict 30-day-mortality after initiation of treatment. If used in a clinical setting, PRSQT may help prevent sudden cardiac deaths associated with QT-prolonging medication.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Acknowledgements
I would like to thank Jonas Ghouse, Søren Albertsen-Rand, Henning Bundgaard, Alex Hørby Christensen and Morten Salling Olesen. I would also like to thank deCODE genetics for the work done in Copenhagen Hospital Biobank and the Danish Blood Donor Study.
References



