
Abstract
Background We aimed to identify influential drivers of the cost-effectiveness of older adult respiratory syncytial virus (RSV) vaccination in Denmark, Finland, the Netherlands and Valencia-Spain.
Methods A static multi-cohort model was parameterised using country- and age-specific hospitalisations using three approaches: (1) the International Classification of Diseases (ICD)-coded hospitalisations, (2) laboratory RSV-confirmed hospitalisations and (3) time-series modelling (TSM). Plausible hypothetical RSV vaccine characteristics were derived from two protein subunit vaccines for adults aged ≥60 years (“60y+”). Costs and quality-adjusted life-years (QALYs) were compared between four strategies: (a) “no intervention” and RSV vaccination in adults (b) 60y+; (c) 65y+; (d) 75y+, from both the healthcare payers’ and societal perspectives. Value of information, probabilistic sensitivity and scenario analyses identified influential drivers.
Results Besides vaccine price, the hospitalisation estimates were most influential: Using adjusted RSV-ICD-coded hospitalisations at a vaccine price of €150 per dose, no intervention was cost-effective up to willingness-to-pay (WTP) values of €80000 per QALY gained in Denmark, and up to €34000 and €62000 per QALY gained in Finland and the Netherlands, respectively. Using the adjusted RSV-confirmed dataset, the findings were consistent in Denmark and comparable in Finland. In Spain-Valencia, the 75y+ strategy became cost-effective at WTP >€17000. Using TSM-based estimates, the 75y+ strategy was cost-effective at WTP >€16000, >€28000, >€13000 and >€37000 in Denmark, Finland, the Netherlands and Spain-Valencia, respectively. The (in-hospital) case fatality ratio and the specification of its age dependency were both influential. Specifying different ways in which protective efficacy waned and RSV seasons were shaped and timed had both relatively limited impact on results.
Conclusion Data gaps and uncertainties on the RSV-related burden in older adults persists and influences the cost-effectiveness of RSV vaccination. More refined age- and country-specific data on the RSV attributable burden are crucial to aid decision making.
Introduction
Respiratory syncytial virus (RSV) is a leading cause of respiratory tract infections (RTI) in both young children and older adults. Among adults aged 60 years and above (60y+), a meta-analysis estimated 5.2 million RSV cases, 470000 hospitalisations and 33000 in-hospital deaths across high-income countries in 2019 [1]. With ageing populations in these countries, this disease burden is expected to increase.
RSV is contagious and seasonal, and it typically peaks during the winter months in Europe, in line with several other respiratory pathogens. RSV leads to a substantial burden, exerting pressure on healthcare resources [2]. The RSV-related disease burden among European older adults has not been well established, in terms of country- and age-specific hospitalisation rates, which are essential ingredients for cost-effectiveness analyses.
Previous systematic reviews included multiple studies that reported hospitalisation rates, but the majority of these studies were conducted outside of Europe [1, 3].
Since 2023, two protein subunit RSV vaccines, Arexvy (GSK) and Abrysvo (Pfizer) were approved for the prevention of RSV disease among adults aged 60y+ and marketed in several high-income countries. In 2024, an mRNA-based vaccine mResvia (Moderna) was approved in the United States (US) [4]. All vaccines have demonstrated protective efficacy lasting for more than one season, with waning immunity observed in the second season [5–8].
Recommendations on RSV immunisation in older adults were made by several National Immunisation Technical Advisory Groups. In the US, the Advisory Committee on Immunization Practices (ACIP) recommended a single-dose RSV vaccine for all adults 75y+ and adults aged 60-74 years who are at increased risk for severe RSV disease [9]. In the United Kingdom (UK), the Joint Committee on Vaccination and Immunisation (JCVI) advised a programme for older adults aged 75 years and above (75y+)[10]. Cost-effectiveness analyses were conducted to inform these ACIP and JCVI recommendations.
The PROMISE (Preparing for RSV Immunisation and Surveillance in Europe) Consortium (https://imi-promise.eu/) aimed to produce new evidence on the burden of RSV disease in Europe, before and after the emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causing coronavirus disease 2019 (COVID-19). For instance, data on RSV International Classification of Diseases (ICD)-coded and RSV-confirmed hospitalisations were collected using national or regional registries in several countries. Moreover, time-series modelling (TSM) was employed to estimate the RSV-attributable hospitalisations for these countries.
We used the data on RSV hospitalisations generated by the PROMISE project to identify and explore the influential parameters and assumptions driving the cost-effectiveness of RSV vaccination strategies among older adults in four European countries: Denmark, Finland, the Netherlands and Spain-Valencia. The choice of these countries was guided by the timely availability of data of sufficient quality and detail within the PROMISE project.
Methods
Cost-effectiveness model
We developed a static multi-cohort model (Figure 1) named Multi-Country Model Application for RSV Cost-Effectiveness policy for Adults (MCMARCELA). The modelled population consists of adults aged 60 to 99 years, who were tracked monthly over a five-year time horizon, which aligns with the expected maximum protective duration of RSV vaccine [11]. The model considered costs and quality-adjusted life-years (QALYs) lost for RSV cases seen in primary care, admitted to hospitals, and symptomatic RSV cases requiring no medical attendance (non-MA). It also assumed that RSV-related mortality occurs only in a hospital setting. Premature RSV-related deaths were calculated from the model using hospital-fatality ratios to estimate QALYs lost over the remaining life-expectancy at the age of death. The model did not separately account for RSV cases requiring only an outpatient visit in hospital or an emergency department visit without admission, because such type of data was not available for most of the countries considered.

Model structure.
The model made comparisons between four strategies: “no intervention” and three age-based single-dose universal RSV vaccination strategies among older adults. Each vaccination strategy was modelled as if a single dose were offered to everyone in an age band at the same time in October, prior to the start of the first RSV season considered over the 5-year time horizon:
I. 60 years and above up to 99 years (‘60y+’ strategy) based on the approved age-indication,
II. 65 years and above up to 99 years (‘65y+’ strategy) considering the universal influenza vaccination programmes in many European countries,
III. 75 years and above up to 99 years (‘75y+’ strategy) based on the JCVI and ACIP recommendation.
This analysis was conducted separately from a healthcare payers’ (HCP) perspective considering only direct medical costs and from a societal perspective, additionally including costs associated with productivity losses of patients. Both costs and QALYs were discounted at rates recommended by the country-specific pharmacoeconomic guidelines (see Supplement Table 6) [12–15].
Model input parameters and assumptions
All parameters are listed in Supplement Table 6, and each input parameter is described in detail in Supplement section 1.1.
In brief, for Denmark, Finland and the Netherlands, RSV-ICD-coded hospitalisations by age and calendar month were estimated retrospectively using national registries. The RSV-confirmed data were also obtained in Denmark and Finland using the same registries [16]. In Valencia, a region of Spain, the RSV-confirmed hospitalisations were collected retrospectively through their regional active hospital-based surveillance network (descriptions in previous publications [17, 18]). The catchment area represented 21% of the overall population in Valencia (approximately 1 million), or 0.2% of the population in Spain. Patients meeting preliminary inclusion criteria and meeting the influenza-like-illness (ILI) case definition [19] were included and systematically tested for RSV with a multiplex polymerase chain reaction (PCR) test. RSV-confirmed data was adjusted to the RSV season as active surveillance was not performed throughout the whole year [16, 20]. The brief description of the data collection methods is in Supplement section 1.1.1, and the full details are available elsewhere [16].
Subsequently, a TSM analysis was conducted to attribute respiratory tract infection (RTI) hospital admissions to RSV, using the number of positive virological isolates of respiratory pathogens, including influenza A and B, SARS-CoV-2, and RSV, over time as covariates. Under this approach influenza and RSV laboratory test frequency was regressed against RTI incidence over time, to determine the proportion of RTI cases that were attributable to the two viruses [21]. In Spain-Valencia, ILI was used instead of RTI in the TSM analysis and an inference on missing weeks without active surveillance was performed in order to account for the fact that data was not available throughout the whole year. The brief description of the TSM analysis is in Supplement section 1.1.1.3 and the full details are available elsewhere [20].
To account for uncertainty on the choice of source data for the hospitalisation estimates, we explored the cost-effectiveness of using (1) the RSV-ICD-coded hospitalisations with an adjustment factor of 2.2 for diagnostic under-ascertainment, except for Spain-Valencia due to insufficient sample size [22]. (2) the RSV-confirmed hospitalisations with the adjustment factor of 2.2 (except for the Netherlands due to data unavailability), (3) the TSM estimated RSV-attributable hospitalisations. The differences among the three hospitalisation datasets were illustrated in Supplement Figures 1-4. We used the average data over three or four seasons (depending on data availability) prior to the COVID-19 pandemic (2016/2017 to 2019/2020).
The RSV-related primary care episodes by age were estimated based on a meta-analysis of US studies [23], which found for every RSV hospitalisation in adults aged 60y+, 8.5 RSV primary care episodes occurred on average. We additionally used higher estimates of RSV-related primary care episodes based on a UK modelling study in scenario analysis [24]. A multi-country prospective study among European community-dwelling older adults provided an estimate of 2.27 non-MA episodes per primary care episode [25, 26]. We used 7.13% (95% CI: 5.4-9.36) for the in-hospital case fatality ratio (hCFR) for all 60y+ based on a meta-analysis [1]. The age-specific RSV-confirmed hCFRs in Finland were used in scenario analysis.
In order to focus on identifying general drivers of cost-effectiveness of RSV vaccination among older adults, and to avoid detractions due to minute interpretative differences in differently defined product-specific clinical endpoints, we consider in this analysis the use of a hypothetical RSV vaccine. We used plausible efficacy (mean and 95% CI) values against non-MA episodes, primary care episodes, hospitalisations, and deaths by combining information available at the time of the analysis for both Arexvy and Abrysvo (Table 1, Supplement 2.1.5) [5, 6]. Based on waning assumptions made in published cost-effectiveness analyses for older adults [27–31], we explored 13 waning scenarios accommodating a range for the duration of protection from 18 months to 48 months (Supplement section 1.15). The RSV vaccine price was assumed to be €150 per dose for all countries in this study [32]. RSV vaccination coverage was based on country-and age-specific influenza vaccination coverage (Supplement Table 6).
Country-specific costs were obtained for hospitalisations, including intensive care unit admissions, primary care consultation, and vaccine administration (Supplement section 1.1.7). A cost of €4.06 per non-MA episode was used for all countries based on a European multi-country prospective study [26]. From a societal perspective, the costs of productivity losses were estimated using the human capital approach: the age- and country-specific daily salaries were adjusted by employment rates and multiplied by the number of workdays lost. We accounted for one and two lost workdays per non-MA and primary care episode, respectively [33], and the country-specific length of hospital stay plus three days per hospitalised case. Productivity losses due to RSV-associated premature deaths were not included in order to avoid double counting [34]. All costs were inflated to their 2023 value using the country-specific consumer price index (CPI) of all sectors, and those reported in local currency were converted to euro (€) using the annual exchange rates of 2023 [35, 36].
QALY losses due to RSV deaths were estimated using remaining life expectancy at age of death and standard age-specific utility values by country [37, 38] (Supplement section 1.1.8 and Table 6). A prospective study in European older adults estimated an average QALY loss of 0.004 (95% CI: 0.001-0.010) per non-MA or primary care episode [33]. There was no utility value available for individuals aged 60y+ who were hospitalised with RSV. Hence, we assumed QALY losses of 0.01023 (95% CI: 0.0089-0.0170) based on another European multi-country prospective study among RSV-hospitalised infants’ parents [39], this value was comparable to QALY losses in hospitalised influenza patients [40]. However, in scenario analysis, we also assumed alternative average QALY losses of 0.0185 (CI: 0.0053-0.0347) for non-hospitalised patients and 0.0193 (CI: 0.0095-0.0316) for hospitalised patients, based on US ACIP meeting presentations of 2022 without full peer-reviewed publication [27].
Analytical approach
We conducted a full incremental analysis of costs and effects arising in all strategies to identify the cost-effective program for willingness-to-pay (WTP) values ranging from €0 to €80000 per QALY gained [41, 42].
To evaluate the impact of uncertain input parameters on the estimated cost-effectiveness, the expected value of partial perfect information (EVPPI) was calculated over a range of WTP values through probabilistic sensitivity analysis. A probabilistic price threshold analysis was also performed for each country applying the method demonstrated by Pieters and colleagues [43].
To explore the impact of key assumptions and input parameters, we also conducted deterministic scenario analyses including 13 scenarios on vaccine characteristics (i.e., efficacy, duration of protection, waning curves), and 16 scenarios on input parameters suchas burden of disease, QALY losses, RSV seasonality, price per dose, and the impact of the COVID-19 pandemic. An overview of scenarios analyses was summarised in Supplement Tables 1 and 7 and section 1.4. All analyses were conducted in R version 4.3.2.
Results
RSV health and economic burden without vaccination
Over a five-year time horizon, (1) using the adjusted RSV-ICD-coded dataset (Supplement Table 10), we estimated 30844, 251938, and 316164 RSV cases (including non-MA, primary care episodes and hospitalisations), as well as 558, 4376, and 8374 discounted QALY losses among adults 60y+ in Denmark, Finland and the Netherlands, respectively. From the HCP and societal perspectives, the discounted costs were €3.6 and 4.0 million in Demark, €32.1 and €34.5 million in Finland, and €76.2 and €90.2 million in the Netherlands, respectively. (2) Using the adjusted RSV-confirmed hospitalisation dataset, the estimated RSV cases were 84671 in Denmark, 325860 in Finland, and 73925 in Spain-Valencia, as well as 1514, 5697, and 1475 discounted QALY losses among adults 60y+ in Denmark, Finland and Spain-Valencia, respectively. From the HCP and societal perspectives, the discounted costs were €9.9 and 11.0 million in Demark, €41.5 and €44.7 million in Finland, and €10.6 and €10.9 million in Spain-Valencia, respectively. (3) Using the TSM RSV-attributable estimates, we observed 24- and 9-fold higher RSV-attributable cases (0.7 million) in Demark compared with the adjusted RSV-ICD-coded and adjusted RSV-confirmed hospitalisations. Consequently, there were higher QALY losses and direct medical and indirect medical costs. In the Netherlands, 4-fold higher RSV-attributable cases (1.3 million) were estimated compared with using the adjusted RSV-ICD-coded dataset. However, both in Finland and Spain-Valencia, the RSV-attributable cases from the TSM were 11% (289079) and 55% (33600) lower than the adjusted RSV-confirmed estimates, respectively. Consequently, large differences were observed in the discounted QALY losses, and the direct and indirect costs attributable to RSV. Despite the large differences in baseline disease burden while using different datasets, it was consistent that the 75-84y age group had the highest number of hospitalisations (except the Netherlands using adjusted RSV-ICD-coded dataset); consequently, the highest number of primary care and non-MA episodes, and discounted medical costs. However, the highest discounted QALY losses mainly occurred in the 65-74y age group (except Spain-Valencia). Most indirect costs due to productivity losses occurred in the 60-64y age group, as it had the highest active labour force participation.
RSV-burden averted with single-dose one-time vaccination over two years protection
Irrespective of the hospitalisation data source, in every country the 60y+ strategy had the greatest impact on disease burden in terms of cases, hospitalisations and deaths averted, QALYs gained, and direct and indirect medical costs averted. However, this was also the most expensive strategy with one-time vaccination costs of €195 million, €139 million, €482 million and €0.03 million in Denmark, Finland, the Netherlands, and Spain-Valencia, respectively. Detailed RSV burden averted estimates are presented in Supplement Tables 9 and 11 by strategy, country and methodological approach.
Cost-effectiveness
In general, more expansive vaccination strategies became cost-effective for the HCP with increasing WTP values per QALY gained (Figures 2-4). A societal perspective increased the potential cost savings per averted case and, therefore, it rendered more expansive strategies cost-effective at lower WTP values than the HCP perspective did (Supplement Figures 8, 11 ,14 and 15)
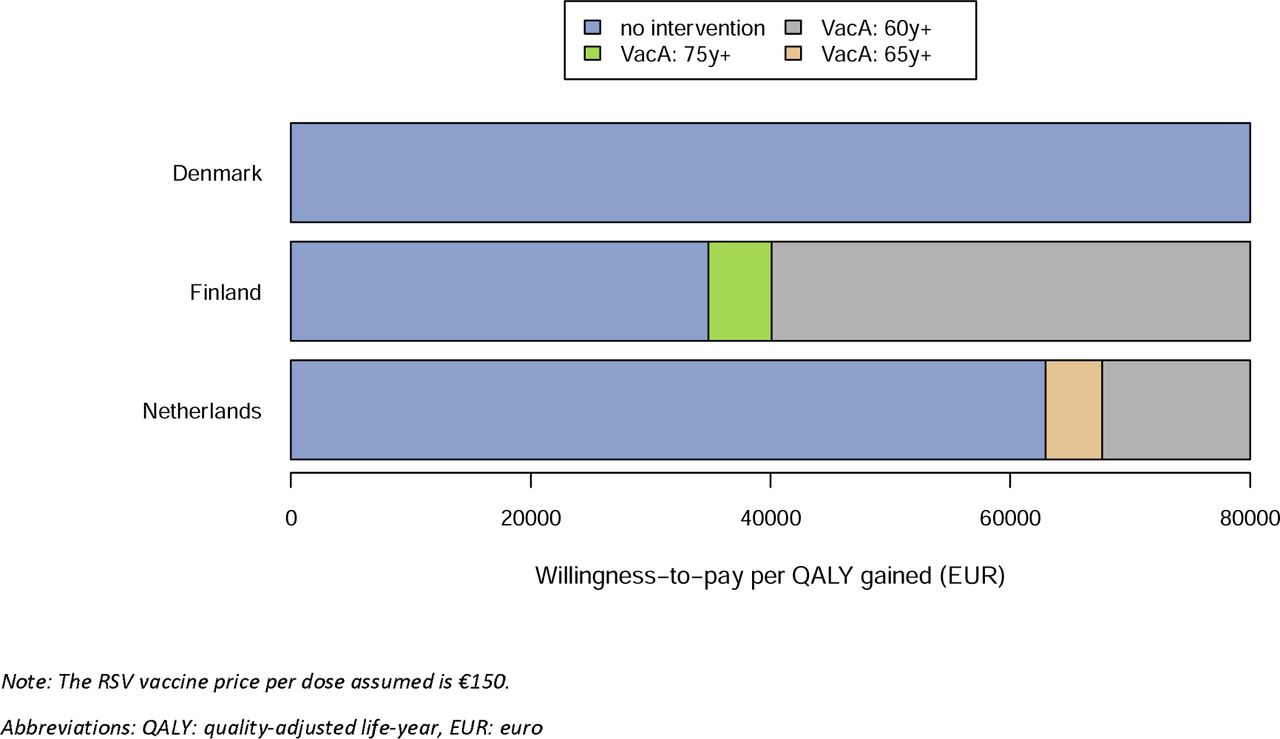
(1) Using the adjusted RSV-ICD-coded hospitalisations (Figure 2), ‘no intervention’ was cost-effective up to a WTP value of €80000 per QALY gained for the HCP in Denmark. In Finland, the 75y+ and 60y+ strategies would be preferred at WTP values exceeding €34000 and €40000, whereas in the Netherlands, the 65y+ and 60y+ strategy became cost-effective at WTP values exceeding €62000 and €68000 per QALY gained, respectively. From the societal perspective, the 65y+ strategy was dominated by the 60y+ strategy in all countries (Supplement Figure 11).
(2) Using the RSV-confirmed hospitalisations (Figure 3), the finding was consistent for Denmark that ‘no intervention’ is cost-effective, whereas in Finland the 75y+ and 60y+ strategies became preferred at lower WTP values (≥27000 and ≥30000, respectively) versus using adjusted RSV-ICD-coded hospitalisations. In Spain-Valencia, the 75y+, 65y+ and 60y+ strategies became cost-effective at WTP values above €17000, €25000 and €34000, respectively.
(3) Using the TSM estimates (Figure 4), the 75y+ strategy was preferred if the WTP value exceeded €16000 in Denmark, €28000 in Finland, €13000 in the Netherlands, and €36000 in Spain-Valencia. The 60y+ strategy became the preferred strategy at higher WTP values of €17000, €36000 in Finland, and €18000 in the Netherlands. In Spain-Valencia, the 60y+ strategy was not preferred up to a WTP value of €80000. Only in Denmark, the 65y+ was weakly dominated by 60y+ (Supplement Figure 9).

Using adjusted RSV-ICD-coded disease burden: preferred strategy based on cost-effectiveness analysis from the healthcare payers’ perspective.

Using adjusted RSV-confirmed disease burden: preferred strategy based on cost-effectiveness analysis from the healthcare payers’ perspective.

Using time-series-modelling RSV estimates: preferred strategy based on cost-effectiveness analysis from the healthcare payers’ perspective.
Influence of price
Variations in the vaccine price from €50 to €250 per dose changed the preferred strategy over a wide range of WTP levels from the HCP perspective. (1) Using the adjusted RSV-ICD-coded dataset (Supplement Figure 17), ‘no intervention’ was cost-effective in Denmark irrespective of WTP per QALY. However, at €50 per dose, in Finland the 75y+ strategy was cost-effective at a WTP value of €30000, whereas in the Netherlands the 65y+ strategy could be cost-effective at a WTP value of €25000. (2) Using the adjusted RSV-confirmed dataset (Supplement Figure 18), findings are consistent in Denmark and comparable in Finland versus adjusted ICD-coded hospitalisation. In Spain-Valencia, at €50 per dose, the 65y+ strategy would be cost-effective at a WTP value of €10000 per QALY gained. (3) Using TSM estimates (Figure 5), the 75y+ strategy would be cost-effective at a WTP of €5000 per QALY gained in Denmark and the Netherlands, €10000 in Finland, and €15000 in Spain-Valencia, and the 60y+ strategy would become cost-effective at higher WTP ranges. Overall, the price reductions led to sharp decreases in the WTP level at which strategies became cost-effective for Denmark. This effect was less pronounced for the Netherlands and even less so for Finland and Spain-Valencia. Decision uncertainty was highest nearby the WTP values at which the cost-effective strategy switched.

Using TSM estimates: Price threshold analysis showing the cost-effective strategy at different WTP thresholds from HCP’s perspective.
Highly influential factors on the optimal strategy (other than price)
● Choice of datasets
The choice of optimal strategy at a given WTP level and price depended in all countries heavily on the choice of dataset to estimate the incidence of RSV hospitalisations (RSV-ICD-coded, RSV-confirmed and RSV-attributable).
● Hospital case fatality ratio (non-age specific and age-specific)
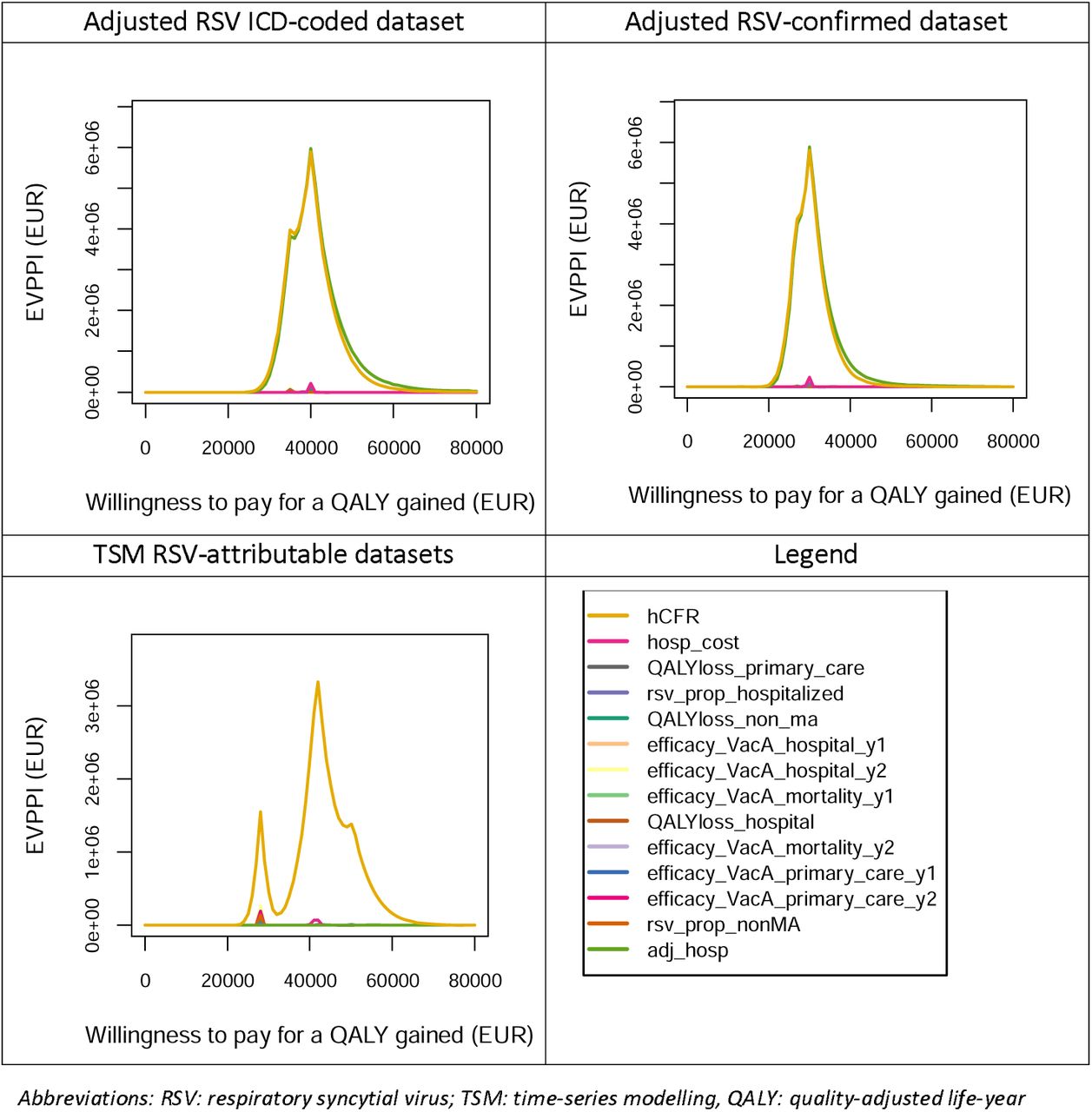
The hCFR was identified as another key driver. The EVPPI graphs demonstrated that the uncertainty around the non-age-specific hCFR caused the most decision uncertainty for all countries across all three datasets (Figure 6 and Supplement Figures 10, 13 and 16).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Expected value of partial perfect information for Finland, using three di 1 fferent hospitalisation datasets
Compared with assuming non-age-specific hCFR for adults 60y+, using relatively higher hCFRs among adults 75y+ made the 75y+ strategy preferred at lower WTP values, and lower hCFRs in the 60-64y and 65-74y age groups made the 65y+ strategy only preferable over the 75y+ strategy at much higher WTP values (Supplement Figure 20).
● Adjustment factor for diagnostic under-ascertainment
The adjustment factor of 2.2 for diagnostic under-ascertainment of hospitalised cases was also influential when using the RSV-ICD-coded and RSV-confirmed datasets (Figure 6 and Supplement Figures 10, 13, 20). Its parametric uncertainty was as influential as that of the non-age-specific hCFR when using the adjusted RSV-ICD-coded and adjusted RSV-confirmed datasets (Supplement Figures 10 and 13).
● Vaccine coverage
RSV vaccine coverage increases in the 60-64y age group can be particularly influential for the competition between the 65y+ and 60y+ strategies in countries with low baseline coverage rates in the 60-64y age group (see also Supplement Figure 20). This is due to the differences in age-specific input values for utility and hospitalisation costs for those younger and older than 64 years of age and the fact that changes in coverage in 60-64y olds imply different weighted average impact changes in the 60y+ age group, which do not occur in the 65y+ age group. For instance, if the coverage rate of 28.5% in the 60-64 y age group in Denmark increased to the same level as the rate in 65y+ age group (78%), the 65y+ strategy would become the preferred strategy at WTP values between €17000 and €38000 per QALY gained. Hence, higher coverage in those incurring lower cost and QALY losses when ill (the 60-64y portion of the target group 60y+) makes the entire 60y+ age group a less optimal choice for vaccination versus the other age groups (which do not include 60-64-year-olds).
Less influential factors on the optimal strategy
The duration of protective efficacy showed more impact than the type of waning curve assumed (Supplement Figure 19). Scenarios considering a seasonal shift of RSV as observed during the COVID-19 pandemic, administering RSV vaccine prior to a “mild” season and applying lower vaccine efficacy in adults 80y+ all yielded negative impacts on the cost-effectiveness results compared to the reference analysis. Scenarios administering RSV vaccine prior to a “severe” season, using higher QALY losses associated with RSV illness and a higher ratio of hospital to primary care, led to more expansive cost-effective strategies. Nevertheless, these scenarios have relatively limited impacts (Supplement Figure 15), in the context of comparing multiple age-based RSV strategies using a single RSV vaccine.
Discussion
We performed a full incremental analysis comparing no intervention and three vaccination strategies in adults aged 60, 65 and 75 years and above to each other using a hypothetical RSV vaccine which bridged phase 3 trial efficacy data available up to June 2024. Our analyses used three hospitalisation datasets in four countries to explore the influential drivers of the cost-effectiveness of RSV vaccination in European older adults. Although there are substantial differences observed among countries in term of cost-effectiveness, the influential drivers are consistent across countries. We found that apart from the vaccine price, the key driver of decision uncertainty regarding which strategy is cost-effective in all countries is the choice of the RSV hospital admissions dataset to use. The second most important uncertainty driver is the non-age-specific hCFR and the adjustment for diagnostic under-ascertainment of hospitalised cases, when using the adjusted RSV-ICD-coded and RSV-confirmed datasets as they were co-related.
Since RSV clinical symptoms are indistinguishable from those of many other respiratory virus infections and laboratory testing for RSV is relatively rare in older European adults, RSV-ICD-coded hospitalisation rates can substantially underestimate the disease burden, especially in countries without routine RSV testing [25, 44]. We, therefore, investigated the impact of using RSV-ICD-coded (except Spain-Valencia), RSV-confirmed (except the Netherlands), or TSM model-based RSV-attributable hospitalisations to inform RSV hospitalisation rates. We showed this impact to be very high. For instance, after applying an adjustment factor of 2.2 to the RSV-ICD-coded hospitalisations and RSV-confirmed, no intervention was cost-effective up to the WTP value of €80000 per QALY gained in Denmark, and up to €34000 and €27000 per QALY gained in Finland. No intervention was cost-effective up to a WTP value of €62000, and €17000 per QALY gained in the Netherlands (using adjusted RSV-ICD-coded hospitalisations) and Spain-Valencia (using adjusted RSV-confirmed hospitalisations), respectively. However, model-based analyses of TSM data yielded increased age-specific RSV attributability, and when using the resulting hospitalisation rates, the 75y+ strategy was shown to be cost-effective at much lower WTP values per QALY gained, except Spain-Valencia.
The TSM-based approach used in this analysis is a method commonly used to estimate the burden of many other diseases such as influenza [45]. In our analysis, we used laboratory test data series on four pathogens (influenza A, influenza B, SARS-CoV-2 and RSV) that cause RTIs (in Spain-Valencia, ILI was used as a proxy for RTI). Although these are four highly important pathogens for RTIs, this is not an exhaustive inclusion of potential causative pathogens and, therefore, the attributable fractions estimated for each or some of these pathogens to RTI hospitalisation may be overestimations, although this was partially adjusted for by including a constant term. On the other hand, RSV-ICD-coded hospital admission data are likely to substantially underestimate RSV-related hospital admissions [44, 46]. RSV diagnostic tests were also not systematically performed except in Spain-Valencia.
When adjusting RSV-ICD-coded and RSV-confirmed datasets with the diagnostic under-ascertainment factor of 2.2, the findings were substantially different than those using TSM estimates in Denmark. The large differences were also observed in the Netherlands when comparing the adjusted RSV-ICD-coded hospitalisation with the TSM estimates. However, the results of using three datasets were comparable in Finland. In Spain-Valencia, the adjusted-RSV-confirmed dataset showed more favourable results for RSV vaccination. This could be explained by the fact that testing was already systematic in all included in patients in Spain-Valencia. However, the use of ILI as inclusion criteria (in Spain-Valencia) is known to underestimate the real RSV burden in the surveillance networks compared to other case definitions an under-ascertainment that has not been corrected for here [25, 47, 48]. Hence, the adjustment factor and its uncertainty need to be interpreted with caution, taking into account country-specific coding and testing practices.
Moreover, the hCFR and the specification of its age dependency were influential (Supplement Figures 10, 13, 15 and 20). Despite the efforts to link the RSV-confirmed deaths with hospital and mortality registries of multiple countries, we were only able to use the age-specific hCFR for Finland, which had a sufficient sample size and was compliant with the applicable data privacy law. Importantly, we demonstrated that acknowledging the age-dependent nature of the hCFR is important when selecting optimal age-based RSV vaccination strategies in older adults.
Our price threshold analysis showed that different “vaccine price per dose” thresholds exist for different “WTP per QALY” levels, implying different optimal choices of strategies. When considering vaccination strategies among 60y+, 65y+ and 75y+, the strategy protecting the oldest (75y+) age group is first selected from the HCP perspective. With increasing WTP values or decreases in price, the 65y+ and 60y+ strategies can become the optimal strategy. Embedded in our calculations is the budget impact. Clearly, the smaller older-age cohorts have a budgetary advantage over larger younger-age ones. In many countries, budget-impact considerations may determine the choice of preferred strategy as much as cost-effectiveness considerations do. For instance, Hodgson and colleagues assumed one year protection and estimated the threshold price at which the 75y+ strategy can be cost-effective at a much higher price (£20.71) than the price (£3.63) at which it would be considered affordable, given a UK-set budget constraint for an individual programme of £20 million annually during the first three years of implementation [49].
The extensive exploration of different shapes of waning and protective duration types of showed it has limited impact on the potential for a cost-effective result for a single RSV vaccine. However, it can become more important in head-to-head comparisons of different vaccine brands, especially so when vaccines compete more on marginal differences in age-specific protective efficacy over time than on more influential differences in price-setting. Given the trial-based information available, with different case definitions of the clinical endpoints of the licensed vaccines, such a head-to-head comparison is beyond the scope of this paper.
We assumed the RSV vaccines would be administered prior to the expected RSV season in Europe in October (with instant protection) in order to maximise the effectiveness. However, depending on the country, influenza, pneumococcal and COVID-19 vaccines are also typically administered in the last quarter of the calendar year in the same target populations, which can lead to implementation challenges for RSV vaccines due to crowded schedules. Given that RSV vaccines protect longer than one season, a year-round programme might be considered, possibly together with the pneumococcal or herpes zoster vaccine among older adults. However, given the clear seasonal pattern of RSV in Europe, a year-round programme would be less effective than a seasonal programme due to waning protection. Moreover, the coverage of pneumococcal vaccines is generally lower than the coverage of influenza vaccines among adults 65 years and above in Europe. Joint advice for RSV, influenza and COVID-19 vaccine before the winter might simplify the communication and, hence, achieve higher coverage.
This is the first analysis that assessed the cost-effectiveness of three age-based RSV vaccination strategies among older adults in more than two countries and identified the key evidence gaps that were most influential to cost-effectiveness. Previous analyses on a single country or two countries did not explore the sensitivity to different data sources, the influence of a shift in seasonality and the severity of a season [29, 30, 40, 49, 50]. Our results are comparable with two cost-effectiveness analyses published in 2023, which applied vaccine protection over two RSV seasons. Moghadas and colleagues evaluated both marketed RSV vaccines in the US among adults aged 60y+. They concluded that both vaccines can be cost-effective at a price of $235 (∼€219) and $245 (∼€228) per dose given a WTP value of $95000 (∼€88000) per QALY gained, with sensitivity analyses on WTP values of $80000 (∼€75000) and $120000 (∼110000) per QALY gained [29]. Using the time-series estimates, our study showed that if the RSV vaccine is priced at €250 per dose, the 60y+ strategy can be cost-effective at WTP values of €30000 and €35000 per QALY gained in Denmark and the Netherlands, respectively. We used age-specific hospitalisation rates, which led to much higher estimates for the 85y+ age group (∼366 per 100000 in the Netherlands and 533 per 100000 in Denmark) in comparison to the US study (214 per 100000 for any adult aged 60y+, with a 54.8% proportion in 85y+). Wang and colleagues conducted a cost-effectiveness analysis in Hong Kong and used adjusted hospitalisation rates ranging from 23.0 to 221.4 per 100000 in the 60-64y and 75y+ age groups, respectively [30]. By adjusting ICD-coded hospitalisations, our analysis estimated a lower rate in Denmark (4.2 and 17.8 per 100000), the Netherlands (0.4 and 2.2 per 100000) and Spain (2.6 and 13.1 per 100000), but a higher rate in Finland (37.1 and 168.0 per 100000). The Hong Kong analysis also generally highlighted the price and disease burden as influential drivers for the cost-effectiveness analysis, as did previous analyses, which assumed protection over one RSV season [40, 49, 50].
Unlike in the UK, where the WTP thresholds of £20000 (∼€24000) and £30000 (∼€35000) per QALY gained from the National Health Service (NHS) perspective are clearly indicated, the four European countries in our analysis do not have an explicit WTP reference value [51]. In Denmark, a WTP value of DKK 88000 (∼€12000) per QALY gained was estimated via a population survey in 2001, which might need updating [52]. In Finland, infant varicella, pneumococcal and rotavirus vaccination programmes were considered to be cost-effective at WTP values ranging from €15000 to €25000 per QALY gained from HCP perspective [53]. In the Netherlands, the reference values of €20000, €50000 and €80000 per QALY gained depended on the disease severity and perspective [54]. In Spain, a threshold of €30000 from the NHS perspective is commonly cited [55]. Instead of using one or multiple arbitrary threshold values, our analysis presented findings over a range of WTP values (€0-80000 per QALY gained) to assess the influence of the WTP value on the optimal choice.
Our study has some additional strengths. It used the most recent country-specific data to populate the model according to country-specific pharmacoeconomic guidelines. Considerable differences in the RSV health and economic burden exist between countries, and policy makers should reflect on these when making decisions. Most strikingly, RSV seasonality changed during the COVID-19 pandemic in many countries. Therefore, we simulated an off-season hospital admission peak (four months earlier) observed during the pandemic and found the results would be less favourable because administering RSV vaccine in October would miss either a portion or the entirety of the seasonal peak. On top of that, we also investigated introducing RSV vaccine in a country with a biannual seasonal pattern and found whether the vaccine was introduced first in a “severe” or in a “mild” season had relatively little impact. This result seems a consequence of protective efficacy remaining substantial in the second season. Furthermore, we explored multiple vaccine efficacy waning scenarios in combination with duration of protection based on the latest clinical data and demonstrated that the duration of protection tends to have more impact than the type of waning curve assumed. Finally, extensive sensitivity analyses were performed using a wide range of WTP values to investigate the sensitivity of the optimal choice of strategy to the adopted WTP level.
An important limitation of our analysis is that we investigated age-based and not risk group-based strategies. We investigated one-time RSV vaccination, but did not attempt to model scenarios with repetitive vaccination of cohorts over time. Future refined information on vaccine effectiveness and durability may allow the evaluation of such strategies realistically in future. Moreover, hCFR was used to estimate RSV-related deaths in the inpatient setting. However, deaths that occurred in community setting (i.e., nursing home) were not captured due to data availability, hence, it might underestimate cost-effectiveness of the RSV vaccine.
There are a few other limitations. Due to data limitations, the hospitalisation rate of a wide age group (18-64 years) was applied to a small subgroup (60-64 years) in all four countries when using TSM estimates. However, the impact on the overall insights from this analysis was negligible. We were unable to explicitly evaluate the impact of potentially disproportionately prevented re-admissions, long-term consequences due to RSV hospitalisation (e.g., transfer to a nursing home instead of home after discharge), RSV vaccine’s potential prevention of exacerbations of chronic respiratory disease and cardiac events [56], and productivity losses of caregivers under the societal perspective, mainly because the occurrence of, and effectiveness against, these endpoints were unavailable.
Conclusion
Large data gaps and uncertainties around the RSV burden among older adults persist in many European countries, contributing to substantial uncertainties regarding the cost-effectiveness of intervention programs. Given that these countries need to make urgent decisions about RSV vaccination, more refined age-, risk group-, and country-specific RSV burden data are crucial. Evidence-based vaccine introduction decisions will require greater investment in enhanced RSV surveillance and better data linkage systems to enable accurate assessments of the age-and country-specific RSV burden, especially in tertiary and primary care settings, such as those established in Finland. Without this, costly and potentially suboptimal decisions risk being made, leading to substantial opportunity costs due to the large target populations to be vaccinated.
Declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Availability of data and materials
Almost all the data analysed and generated during this study are included in this published article and its supplementary files. Formal requests for additional data can be made to the corresponding author (XL) or the senior authors (PB).
Funding
This project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement number 101034339. The JU receives support from the European Union’s Horizon 2020 research and innovation program and European Federation of Pharmaceutical Industries Associations. MJ received funding from the NIHR Health Protection Research Units in Modelling and Health Economics (NIHR200908) and Immunisation (NIHR200929).
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Competing interests
Outside the submitted work, PB declares funding received by his institute from Merck for research on varicella-zoster and Pfizer for research on pneumococcus vaccine, XL declares funding received by her institute from Icosavax, but they have not received any personal fees or other personal benefits. CKJ reports a research grant from Nordsjællands Hospital, travel grants from the University of Copenhagen, William Demants Fond in Denmark, and the European Society of Clinical Virology and expert consultation fees from Sanofi, outside of the submitted work. Outside the submitted work, HN declares consulting fees received from WHO, Pfizer, Bill and Medlinda Bill and Melinda Gates Foundation and Sanofi, honoraria for lectures/presentations from Astra Zeneca, GSK and Pfizer paid to his institution, travel grants from Pfizer and Sanofi, and participation on a Data Safety Monitoring Board or Advisory Board of GSK, Sanofi, Merck, Icosavax, Pfizer (paid to his institution), as well as WHO and ResViNET (unpaid). AUF declares grants/contracts from Moderna and VAC4EU paid to her institution, outside submitted work. AOS and JDD declares grants/contracts from Moderna, MSD and GSK paid to their institution, outside submitted work. AOS also declares consultancy fees from GSK and Moderna, outside submitted work. JDD declares consultancy fees and honoraria from GSK, Pfizer and MSD, and travel grants from Sanofi and GSK, outside the submitted work. HS declares attending Adult Immunization Board meetings twice a year, the meetings (and travel) are funded by an unrestricted grant from Vaccines Europe, outside submitted work. LW declares grants received from Research Foundation Flanders (FWO), Antwerp University Research Council and Horizon Europe 2.1 – Health paid to his institute, outside the submitted work. MJ declares research grants from NIHR, RCUK, BMGF, WHO, Gavi, Wellcome Trust, European Commission, InnoHK, TFGH, CDC, Gates Foundation paid to his institution, outside the submitted work.
Other authors declared no competing interests.
Authors’ contributions
PB and HN initiated and supervised the study. XL, LW, JB and PB conceptualised the study. XL analysed input data, performed literature searches and auxiliary data collection. XL, LW and JB wrote the cost-effectiveness model codes. XL performed the cost-effectiveness analyses. CKJ, AUF, and LT conducted national/regional database analyses, and collected and validated data in Denmark, Spain-Valencia, and Finland, respectively. CKJ, ROY, and TL led and estimated the time-series model-based hospitalisations. HS, AOS and JDD provided implementation, resource use and cost data for Finland and Spain. HN, MJ, JB and PB advised on model parameters, intervention characteristics and scenario analyses. XL, LW, JB and PB wrote the initial manuscript draft. All authors critically reviewed the manuscript and provided final approval of the manuscript.
Data Availability
Almost all the data analysed and generated during this study are included in this published article and its supplementary files. Formal requests for additional data can be made to the corresponding author (XL) or the senior author (PB).
Acknowledgements
PROMISE investigators: Harish Nair and Harry Campbell (University of Edinburgh, Edinburgh, UK); Louis Bont (University Medical Centre, Utrecht, the Netherlands); Philippe Beutels (University of Antwerp, Antwerp, Belgium), Peter Openshaw (Imperial College, London, UK), Andrew Pollard (University of Oxford, Oxford, UK), Hanna Nohynek (Finnish Institute for Health and Welfare, Helsinki, Finland), John Paget (Netherlands Institute for Health Services Research, Utrecht, Netherlands), Eva Molero (Teamit Research S.L., Barcelona, Spain), Javier Díez-Domingo (Vaccine Research Department, FISABIO-Public Health and CIBERESP, ISCIII, Valencia, Spain), Rolf Kramer (Sanofi Pasteur, Lyon, France), Jim Janimak (GlaxoSmithKline, Wavre, Belgium), Veena Kumar (Novavax, Gaithersburg, Maryland, United States), Elizabeth Begier (Pfizer Limited, New York City, New York, United States), Jenny Hendri (Janssen, Beerse, Belgium).
The authors would like to thank You Li, Valerie Sankatsing and Matthieu Beuvelet for their critical review of our study report and valuable comments.
List of abbreviation
- ACIP
- Advisory Committee on Immunization Practices
- CI
- confidence interval
- COVID-19
- coronavirus disease 2019
- CPI
- consumer price index
- EVPPI
- expected value of partial perfect information
- hCFR
- in-hospital case fatality ratio
- HCP
- healthcare payer
- ICD
- International Classification of Diseases
- ILI
- influenza-like-illness
- JCVI
- Joint Committee on Vaccination and Immunisation
- MA
- medical attendance
- MCMARCELA
- Multi-Country Model Application for RSV Cost-Effectiveness policy for Adults
- PCR
- polymerase chain reaction
- PROMISE
- Preparing for RSV Immunisation and Surveillance in Europe
- QALY
- quality-adjusted life-years
- RSV
- respiratory syncytial virus
- SARS-CoV-2
- severe acute respiratory syndrome coronavirus 2
- TSM
- time-series modelling
- UK
- United Kingdom
- US
- United States
- WTP
- willingness-to-pay
- Y
- year
Reference



