
ABSTRACT
We report general acceptance of an mpox vaccine (61.0%) in the Democratic Republic of the Congo (n=5226) with higher acceptance among healthcare workers and respondents in historic mpox-endemic regions. These data highlight the need for increased community engagement and sensitization before widespread deployment of the mpox vaccine.
INTRODUCTION
Mpox is a zoonotic viral infectious disease first identified in humans in the Democratic Republic of the Congo (DRC) in 1970 (1-3). Monkeypox virus (MPXV) has historically circulated in the tropical forest regions of Central and West Africa, where it is considered endemic (4, 5). However, rapid spread of MPXV to new regions worldwide in 2022 resulted in >91,000 confirmed infections in non-endemic regions and the declaration of a public health emergency of international concern (6). The virus is subclassified into two clades: Clade I, formerly known as the Congo Basin (Central Africa) clade, and Clade II, formerly known as the West African clade (7, 8). Several studies have suggested that clade I infections are associated with greater disease severity, more pronounced rash, and increased human-to-human transmission as compared to clade II infections (9, 10). Additional factors likely also influence the severity of the disease, such as host factors, access to healthcare, and reporting bias.
Among mpox-endemic regions, the DRC has faced the greatest public health burden. In recent years there has been a sharp increase in cases in DRC, nearly doubling from 2021 to 2022 and more than doubling from 2022 to 2023 with >28,000 suspected cases from January 2023 to July 2024 (case fatality rate of 4.5%) (11). While most mpox emergence events have been due to zoonoses, recent outbreaks have demonstrated increasing human-to-human transmission. This has been accompanied by geographic expansion of mpox cases to large urban centers, suspected cases among sex workers, and male-to-male and male-to-female transmission through sexual contact (12).
In spite of the ongoing concurrent mpox outbreaks in DRC and continuing regional expansion with confirmed mpox cases in adjacent locations in East Africa, there is no mpox vaccine access for the general population. Modeling of the potential impacts of modified vaccinia Ankara-Bavarian Nordic (MVA-BN) vaccinations suggested that vaccination of 80% of children <15 years in DRC would result in robust reductions on morbidity, mortality, and mpox circulation (13). While past studies have demonstrated an overall 90% acceptance rate among respondents for routine immunization (RI) vaccines (including BCG, polio, measles) in the DRC, outbreak-related vaccine acceptance (including cholera, COVID-19, and Ebola) was 54% (14). Given the increasing support for vaccine deployment within DRC, there is a critical need to address mpox vaccine acceptance and knowledge to inform mpox vaccination deployment and prioritization strategies.
THE STUDY
The study sample included a cross-sectional subset of a longitudinal phone survey from December 2023 to February 2024 including participants from all 26 provinces in the DRC. Ethics approvals were provided by the Kinshasa School of Public Health (ESP/CE/188/2023), and a public health response activity designation by UCLA and Task Force for Global Health (TFGH). The survey included questions to address behavioral and social drivers of vaccination, vaccine acceptance, and attitudes related to the introduction of new vaccines to the national RI schedule, including mpox. Participants were contacted by phone with their numbers selected from historical phone survey records (n = 10,835); 5226 adult participants were enrolled. Vaccine acceptance was measured by asking participants if they would be interested in an mpox vaccine that has not yet been introduced into RI in DRC.
Attitudes towards the introduction of an Mpox vaccine were categorized with responses “Yes, for all populations”, “Yes, for children only” and “Yes, for adults only” collapsed as general vaccine acceptance, and “No, not interested” and “Do not know the disease” as separate categories. We computed the proportion of vaccine acceptance with 95% confidence intervals (95%CI) by province, by sociodemographic characteristics and compared them using the chi-square test (α = 0.05).
Respondents were predominantly male (79.2%), with the highest percentage from Kwilu province (12.6%). There was roughly equivalent representation of those from urban or rural settings. Most respondents reported some college/university education (41.2%) and identified as healthcare workers (55.5%). (Table 1).
For all vaccines, responses on a 5-point Likert scale suggested that participants generally disagreed that there were greater risks associated with newer vaccines as compared to older vaccines. Twelve provinces had at least 50% of respondents who strongly disagreed with this statement, while Lualaba had the highest percentage (33.5%) of respondents who strongly agreed that greater risks exist. There was general agreement that information received about vaccines from the vaccination program was reliable and trustworthy. Aside from Kinshasa and Tshuapa, all provinces had at least 50% of respondents who strongly agreed with this statement (Figure 1).

(A) Reported responses to the statement “New vaccines carry more risks than older vaccines” (B) Reported responses to the statement “Information I receive about vaccines from the vaccine program is reliable and trustworthy”. Responses are recorded based on a 5-point Likert scale (1 = Strongly disagree; 5 = Strongly agree).
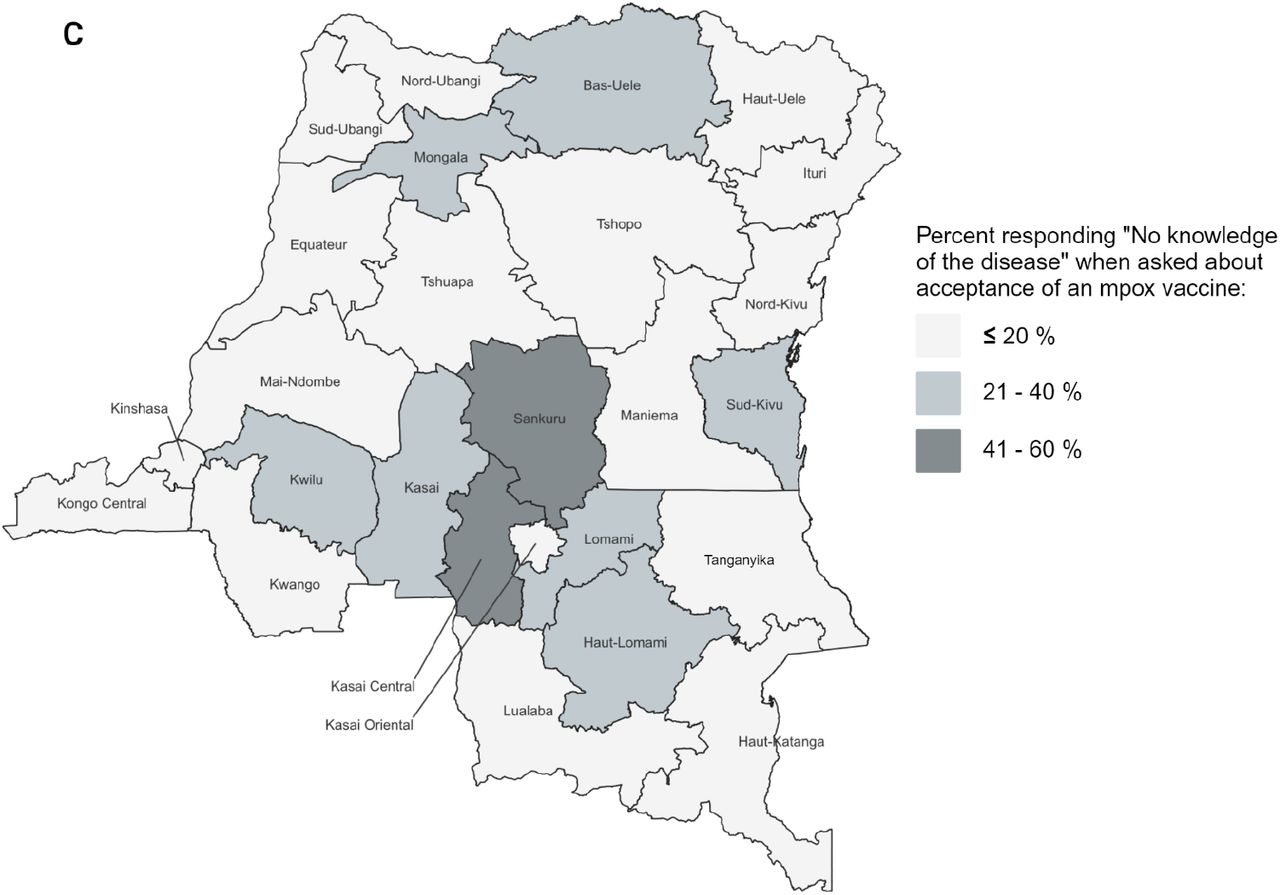
Nationally, there was general acceptance of mpox vaccination by all respondents (61.0%, [59.6-62.4]). Of all respondents, 21.7% had no interest in an mpox vaccine, and 17.3% reported no knowledge of mpox. At the provincial level, >80% of respondents from Kwango, Tshuapa, Nord Ubangi, Tanganyika, and Maniema were accepting of a vaccine, while respondents from Sankuru province had the lowest acceptance (19.9%, [14.3, 26.6]). Sankuru also had the highest percentage of participants that reported no mpox knowledge (57.4%, [49.7-64.8]) (Figure 2).


{kind=link}
{kind=link}
{kind=link}
(A) Reported acceptance as the collapsed responses of “Yes, for all populations” and “Yes, for children only” and “Yes, for adults only” (B) Reported non-acceptance by the response “No, not interested”. (C) Reported lack of knowledge of mpox disease. Percentages are reported by province.
We report significant association between acceptance of the vaccine and province (χ2 = 885.0, p-value <0.0001). Respondents who completed secondary school had higher acceptance of an mpox vaccine compared to those who did not (61.0% vs 60.9%, p-value = 0.7496). When assessing acceptance by occupation, healthcare workers had the greatest acceptance rates of all occupations reported (69.4%, [67.6, 71.1]). The lowest acceptance rate was among those not employed (43.6%, [37.7, 49.7). Respondents from rural locations had greater acceptance of mpox vaccine deployment than their urban counterparts (64.4% vs 57.7%, p-value <0.0001). Of note, among respondents who had received a COVID-19 vaccine (n = 4396), 63.2% indicated mpox vaccine acceptance (Table 2).
COVID-19 vaccination was dichotomized by whether the respondent received the COVID-19 vaccine. Health condition was dichotomized based on whether the respondent stated they had a chronic disease or were immunocompromised.
Mpox knowledge was significantly associated with educational attainment; respondents who had completed secondary school had greater knowledge of the disease (χ2 =4.0961, p-value = 0.0430). Among those currently not working, 21.1% reported no knowledge of mpox.
CONCLUSION
Given the ongoing escalation of the concurrent DRC mpox outbreaks, there is increasing likelihood for the introduction of an mpox vaccine. However, there is a paucity of information regarding either mpox vaccine acceptance or mpox knowledge across DRC, in both rural and urban regions. This phone survey-based investigation demonstrated that there is general acceptance of mpox vaccine deployment nationally, with the greatest acceptance rates among historically mpox-endemic provinces. When comparing urban and rural populations, respondents from rural locations had the greater interest in mpox vaccine deployment. This is perhaps unsurprising given that the highest burden of mpox within the DRC has historically been found among children within rural regions. However, this survey was limited to those with access to phones; individuals with a lower socioeconomic status may have been inadvertently excluded from this study, including those in largely rural regions of DRC. However, the representation of participants from across all provinces in DRC ensures that these insights are broadly applicable to the general population. These results will help provide guidance for imminent mpox vaccine rollouts in DRC and future deployments in adjacent regions. Further, this investigation also provides important insights regarding vaccine acceptance and deployment strategies within DRC, or regionally, for other emerging infectious diseases.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
FUNDING
The project or effort depicted is funded by the Task Force for Global Health (TFGH) under Grant # 20234052:1. The content of the information does not necessarily reflect the position or the policy of TFGH, and no official endorsement should be inferred.
ACKNOWLEDGEMENTS
All cartographic figures were generated using qGIS (Maidenhead, 3.3.4).
We thank Brooke Aksnes and Emma Wray Aberle-Grasse for their continued support of this ongoing research endeavor.



