
Abstract
We evaluated risk factor differences and cognitive domain markers associated with progression in subjects with subjective cognitive decline (SCD) at baseline from the NYU Alzheimer’s Disease Research Center. We included SCD non-decliners (n = 27), who remained stable, and decliners (n = 24), who progressed to mild cognitive impairment or worse, between the second to sixth yearly follow-up visits. Adjusted mixed-effects models examined group differences and associations between demographic, APOE status, psychometric test performance and comorbidities with longitudinal-decline. Overall, mean (SD) age was 67.4 (9.2) and total follow-up time was 5.1 (1.8) years. Lower education (14.9 (3.2) vs. 17.3 (2.1)), Hispanic ethnicity (50.0% vs. 11.0%), and hypercholesterolemia (aOR: 6.67), p ≤ 0.05 for all, were risk factors for progression in SCD, whereas APOE status was not. Notably, SCD decliners were at increased risk for both amnestic and non-amnestic cognitive-decline with psychometric changes in memory, executive, and language domains (p < 0.001 for all). These findings inform further work on SCD outcomes and related biomarkers, as well as preventive studies that target modifiable risk factors for SCD progression.
Introduction
Subjective cognitive decline (SCD) is considered a preclinical stage of Alzheimer’s disease (AD), identifying persons with normal performance on psychometric tests who progress to subsequent AD stages faster than cognitively normal individuals without subjective complaints.1 Consequently, SCD also associates with imaging and biofluids biomarkers of AD2-5.
Specifically, previous work from our center6 showed that SCD is a precursor of further decline to mild cognitive impairment (MCI) or dementia over a 7-year mean follow-up interval. Specifically, in a sample of 260 subjects (166 cognitively normal with SCD and 47 cognitively normal without SCD), SCD subjects were 4.5 times more likely to decline to mild cognitive impairment (MCI) or dementia. We subsequently studied features of decline in 98 SCD subjects over a 2-year interval, noting worsening scores on the Digit Symbol Substitution Test and the Brief Cognitive Rating Scale for staging assessment, as well as a reduction in anxiety7.
Subsequently, we reported on the characteristics of a pre-SCD condition materializing in likely AD. In this study 47 cognitively normal healthy older subjects (mean baseline age= 64.1±8.9 years) were followed for approximately 6.7±3.1 years. After controlling for age, sex, years of education, and follow-up time, there were significant group differences in the rate of decline and composite psychometric scores between future decliners (n=36) relative to non-decliners (n=11).8
As such, SCD can be a precursor to MCI or AD dementia, taking as long as 7 to 15 years for transition to occur. However, stage transition rates may differ even among SCD subjects, as we have found in the pre-SCD interval8. Moreover, the specific drivers and nature of SCD progression remain unclear. Therefore, in this study we evaluated risk factor differences between SCD decliners and non-decliners related to demographics, genetics, and presence of comorbidities. We also investigated cognitive domain markers associated with progression over time in order to investigate the nature of progression in subjects with SCD.
Methods
Study Design, Participants and Variables
Study Design
A retrospective longitudinal analysis was conducted on selected subjects followed at the NYU Alzheimer’s Disease Research Center (ADRC). The NYU Grossman School of Medicine Institutional Review Board approved all aspects of this study, and written informed consent was obtained from all subjects.
Participants
Subjects were community dwelling, over 55 years of age, recruited by public announcement or referral to participate in this longitudinal study on cognition and brain aging. Inclusion for the ADRC include (1) having a study partner, (2) fluency in English and Spanish (including their study partner), and (3) willingness to undergo ADRC Clinical Core evaluation that includes imaging and blood draw. Exclusion criteria include (1) history of moderate/severe psychiatric illness, significant neurological disease other than AD and related disorders, significant organ disease or transplant, autoimmune disease requiring treatment; malignancy within 5 years (other than low grade prostate cancer, non-melanotic skin cancer); (2) alcohol or drug abuse. Participants are followed yearly, and the ADRC Clinical Core evaluations include full clinical, neurological, psychiatric, neuropsychological, clinical laboratory, and neuroimaging evaluations according to the National Alzheimer’s Coordinating Center Uniform Data Set 3.0. For our analysis we analyzed a subset of Clinical Core participants that (1) had a consensus diagnosis of SCD at baseline by the Global Deterioration Scale9 and (2a) who remained cognitively and functionally normal for six annual visits, deemed “non-decliners” or (2b) who progressed to MCI or dementia between the second to sixth follow-up visits, deemed “decliners.” This resulted in an analysis cohort of 27 non-decliners and 24 decliners. Subjects included in this analysis cohort were recruited between January 1, 2013 and December 31, 2015, followed at yearly intervals until December 31, 2021. Follow-up evaluations were completed without reference to the prior results.
Demographic variables
Demographic variables included age (calculated from reported date of birth), sex (biological variable as reported by subject), years of education (calculated based on highest reported completed diploma/degree), and body mass index (calculated from measured weight and height).
Genetic variable (APOE)
APOE genotype was characterized as having at least one APOE □4 allele or at least one APOE □2 allele.
Medical Co-morbidities
Clinical co-morbidities assessed included clinical history of hypertension, diabetes, anxiety, insomnia, obstructive sleep apnea, osteoarthritis, hypercholesterolemia, and thyroid disease. These conditions were reported by subjects during clinical assessment.
Cognitive variables
Cognitive measures assessed in this study included the functional and cognitive assessments used in the National Alzheimer’s Coordinating Center’s Uniform Data Set 3.0: Clinical Dementia Rating (CDR) scale, Mini Mental State Exam (MMSE), Montreal Cognitive Assessment (MoCA), Digit Span Recall (Forwards, Backwards), Benton Visual Retention Tests, Craft story, Multilingual Naming Test (MINT), Vegetable and Animal naming, Trail Making Test Part A and Part B.
Statistical Analysis
All models included age, sex, education, self-reported Hispanic ethnicity, baseline psychometric data, and APOE genotype.
Comparison of baseline participant characteristics between SCD decliners vs. non decliners
Generalized linear models examined group differences in continuous demographic risk factors. Differences in categorical variables were assessed with the Fisher exact test to compare proportions of subjects between SCD groups.
Comparison of Psychometric test performance over time in SCD decliners vs. non-decliners
Analysis of Covariance (ANCOVA) was conducted to test whether significant differences in changes in mean cognitive scores existed between SCD groups over time. In the ANCOVA analysis, time was treated as continuous. Psychometric test performance associations with longitudinal decline, comparing decliners to non-decliners, were also investigated with linear mixed effects models.
Examining associations of medical comorbidities with longitudinal decline
To investigate the associations of medical comorbidities with longitudinal decline, comparing decliners to non-decliners, logistic (i.e., non-linear) mixed-effects models with random intercept and slope were used controlling for covariates/potential confounders, and their interactions with time (operationalized as years from baseline for each participant).
Results
Comparison of baseline participant characteristics between SCD decliners vs. non decliners
At baseline, there were no significant differences between decliners and non-decliners in age, sex, clinical co-morbidities, APO-ε2 or APO-ε4 carrier status (Table 1). The mean (SD) age for decliners vs. non-decliners was 68.5 (11.3) vs. 66.3 (7.1) years (p =0.41). The proportion of females was 67% vs. 74%, and APOE4 was 29% vs. 33%, p≥0.70 for both. There were significant differences in follow-up time, years of education and Hispanic ethnicity. The mean (SD follow-up time was 3.7 (1.97) vs. 6.3 (1.60) years, (p <0.001) for decliners vs. non-decliners. Subjects with lower years of education (14.9 (3.2) vs. 17.3 (2.1)) and those of Hispanic ethnicity (50% vs. 11%) were more likely to be decliners (p ≤ 0.004 for both).
Comparison of Psychometric test performance over time in SCD decliners vs. non-decliners
Results of the ANCOVA analysis are shown in Table 2. SCD decliners were at increased risk for psychometric changes in the Craft story (verbal short-term memory), Multilingual Naming Test (MINT), Vegetable and Animal semantic fluency tests, and the Trail Making Test Part A and Part B assessing for processing speed and executive function (p < 0.001 for all).
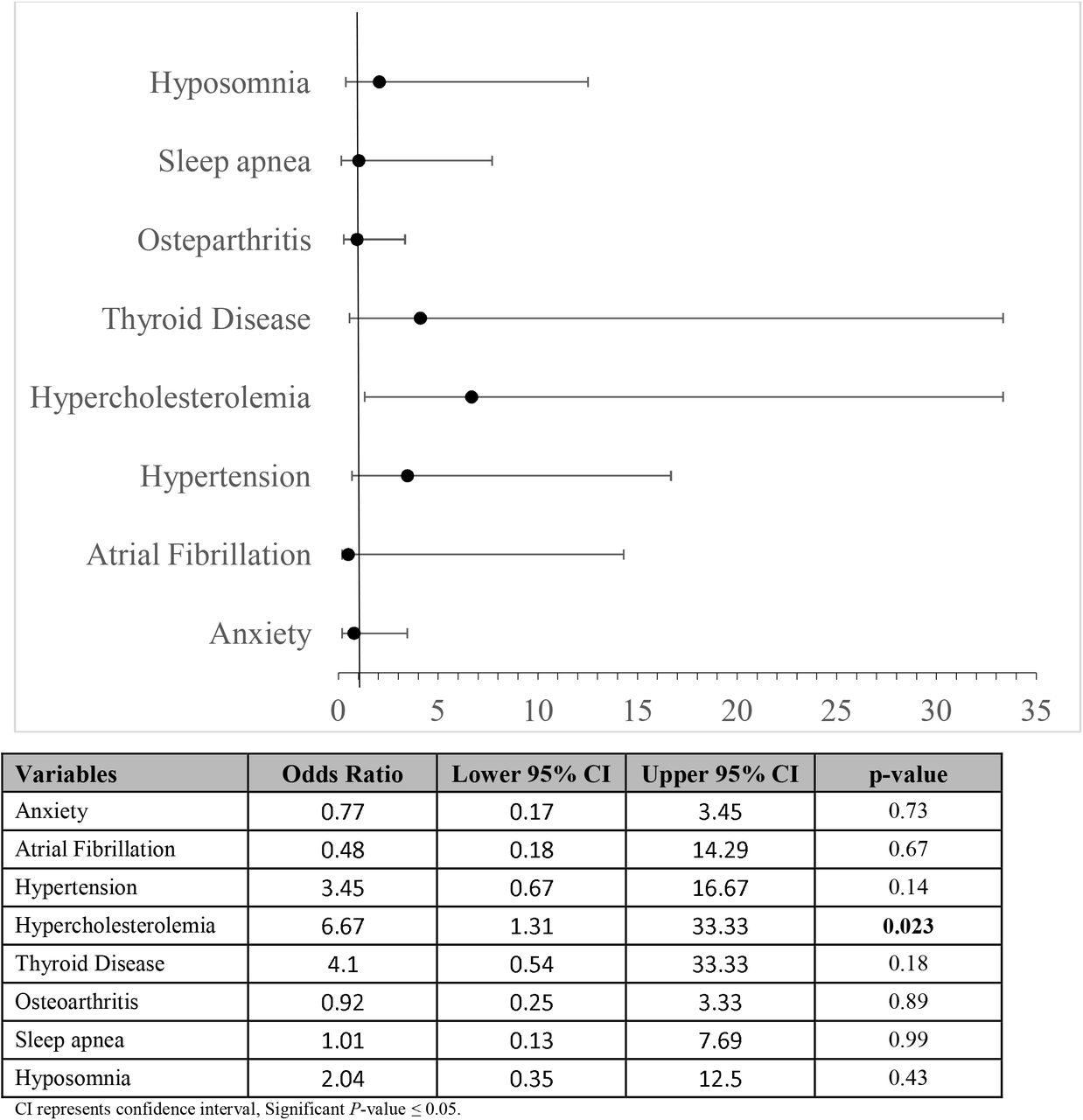
Examining associations of medical comorbidities with longitudinal decline
Logistic mixed effects estimates examining associations of medical comorbidities with longitudinal decline are shown in Figure 1. Only hypercholesteremia had a significant association. Decliners were approximately 7 times more likely (aOR: 6.67; 95% CI: 1.30 – 33.33, p =0.002) to have hypercholesterolemia compared to non-decliners.

{kind=link}
Discussion
Our findings indicate that lower education, Hispanic ethnicity, and hypercholesterolemia are risk factors for progression in SCD, whereas APOE-ε4 carriage is not. The nature of progression showed prospective decline in psychometric tests across multiple domains: memory, language (naming and semantic fluency), processing speed and executive function. Thus, SCD decliners are at increased risk for both amnestic and non-amnestic cognitive decline.
Regarding the demographics risks factors, education and related factors of educational quality and literacy are well established risk factors for dementia.10,11 Racial and ethnic minorities (e.g. Hispanic persons) have disproportionately higher rates of dementia and clinical AD,12 and vascular risk factors (e.g. hypercholesterolemia) lower the threshold for cognitive impairment.13,14 Moreover, such factors are synergistic in that racial and ethnic minorities with lower education, and associated social determinants of low income and reduced health care, have even higher risk of SCD15. Additionally, these challenges can be exacerbated when individuals fail to discuss cognitive decline with health care professionals. Thus, our results suggest that SCD screening, monitoring, and intervention in these groups is of high clinical importance.
Our finding of hypercholesterolemia as a risk factor for SCD progression is not only expected as a risk factor for vascular cognitive impairment, but it is also has links to AD. Indeed, we have previously observed that hyperlipidemia is equivalently prevalent in MCI from neuropathologically-confirmed AD and microvascular disease16,17. Yet, imaging biomarkers of microvascular disease (e.g. white matter hyperintensities on MRI FLAIR sequence) are not driven by hypercholesterolemia in SCD18. However, hypercholesterolemia has been associated with elevated brain amyloid levels and hypometabolism in AD-susceptible brain regions19-22. As it is a modifiable factor, lipid control in persons with SCD may be an important intervention to prevent the onset of objective cognitive decline.
APOE-ε4 carriage was surprisingly not a risk factor for progression in SCD in our cohort, despite its well-known association with increase AD risk23 likely due to increased amyloid deposition24. In other studies of SCD, APOE-ε4 carriage has been associated with higher CSF p-tau, lower CSF AB42, and higher amyloid deposition25. Such abnormalities, particularly CSF AB42/tau ratio, are reliably predictive of SCD progression to MCI and AD dementia26. One possibility to explain this discrepancy, apart from cohort and SCD assessment differences, is that SCD progression may correlate with accelerated spread of tauopathy, which may be less driven by APOE-ε4.
Furthermore, since we do not have biomarkers assessments in this cohort, it is also possible that some of the progression is due to vascular disease. This may be supported by aspects of non-amnestic progression and hyperlipidemia as a risk factor. Future work could potentially observe biofluids and/or imaging markers of amyloid, tau, and cerebrovascular disease in SCD participants to investigate their predictive value for amnestic vs. non-amnestic decline. Such work would help establish these biomarkers as complements to psychometric testing as predictors of disease status and progression, and provide more objective clinical insights into SCD pathology.
Strengths of our study include the comprehensive psychometric assessments and the longitudinal follow-up of study participants. Limitations of this study include the small sample size, as well as the absence of established markers of AD neuropathology such as amyloid and tau.
In summary, our findings inform on the design of biomarker studies of SCD outcomes, as well as preventive studies of MCI and eventual AD that target education and vascular risk in SCD subjects.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Conflicts of Interest
The authors declare no conflicts of interest
Acknowledgements
This work was funded by NIH P30 AG008051 and P30 AG066512.
References



