
Abstract
Background The prevalence of diabetes is rising rapidly across West Africa, posing a significant public health challenge. Effective diabetes management through accessible and quality primary healthcare is crucial, yet multiple barriers persist. This review aimed to synthesise the available evidence on factors influencing access, utilisation, and quality of diabetes primary care in West Africa.
Methods Our scoping review followed Arksey and O’Malley’s methodology and PRISMA-ScR guidelines. We comprehensively searched electronic databases and grey literature for studies covering 2000-2023 that reported factors related to diabetes primary care in West African countries. Data was extracted and analysed through a framework synthesis approach integrating the World Health Organisation Operational Framework for Primary Health Care, the Social Determinants of Health model, and the Innovative Care for Chronic Conditions model.
Results Twelve studies were included from Nigeria (n=7), Ghana (n=4), and Senegal (n=1). Key barriers to access, utilisation, and quality were identified as health system deficiencies, including lack of infrastructure, workforce shortages, supply gaps, fragmented care coordination, absence of standardised guidelines, high costs of care, and limited governance for chronic disease management. Broader determinants of health, such as poverty, gender, cultural beliefs, reliance on traditional medicine, and health policy gaps, were found to influence access to and utilisation of care significantly. Individual-level barriers like psychological distress and delays in care-seeking were also significant. However, family/social support systems emerged as potential facilitators of accessing and utilising PHC services.
Conclusions Our review indicates a complex interplay between health system deficiencies, deeply rooted cultural beliefs, and lived experiences shaping diabetes care in West Africa. The region’s unique challenges demand a paradigm shift from conventional chronic care models to context-specific, adaptive models. Crucially, the gendered aspects of care and the integration of traditional healing practices emerge as pivotal yet often overlooked factors in diabetes management. Furthermore, addressing the bidirectional relationship between mental health and diabetes offers a promising avenue for improving outcomes. Future strategies must transcend the biomedical model, embracing a sociocultural approach that leverages community assets and addresses structural inequities.
Introduction
According to the World Health Organisation (WHO), the prevalence of diabetes has become a significant threat to global health, with over half a billion adults currently living with this condition worldwide. This burden is profoundly felt in low and middle-income countries (LMICs) in regions such as Sub-Saharan Africa (SSA), where an estimated 24 million people had diabetes in 2021(1). SSA is currently grappling with the double burden of communicable and noncommunicable diseases (NCDs), which is impacting the lives of millions across the continent (1).
In the West African region, the prevalence of undiagnosed diabetes is estimated at 4% and rising, with further estimates asserting that prevalence rates of undiagnosed diabetes in this region outpace rates in the rest of Africa (2–4). According to a systematic analysis (2), the pooled prevalence of undiagnosed diabetes mellitus across West Africa is at 4.72%, higher than the prevalence rates observed in other African regions, such as 4.43% in Eastern Africa, 4.27% in Northern Africa, and 1.46% in Southern Africa. The prevalence of diabetes varies across West African countries, with estimates ranging from 2.8% to 3.95% in Ghana, 1.7% to 2.1% in Burkina Faso, and as high as 5.6% in Niger (5–7).
Uncontrolled diabetes can lead to complications, including cardiovascular disease, kidney failure, blindness, and premature death (8,9). These complications not only impact the quality of life of individuals living with diabetes but also place a substantial burden on healthcare systems and societies. Improving prevention, early detection, and management through effective primary health care (PHC) can prevent complications and adverse outcomes in ambulatory care-sensitive (ACS) conditions such as type II diabetes.
For this study, we define primary health care as encompassing three interrelated components: integrated health services that prioritise primary and public health functions; multisectoral policy and action for health; and empowered people and communities (10). PHC represents the first point of contact within the health system, offering continuous, comprehensive, and coordinated care that includes prevention, early diagnosis, treatment, and management of complications.
The WHO recognises PHC as the most inclusive, equitable, and cost-effective approach to achieving universal health coverage (11). Compared to high-income countries (HIC), LMICs struggle with providing accessible, uninterrupted quality care for managing ACS conditions like diabetes that require lifelong self-care and continuous health system support (12). West Africa, in particular, has considerable barriers hampering access to quality PHC, consequently creating substantial gaps in the delivery of effective first-line services for diabetes (13,14). Health system barriers include limited resources, a shortage of human resources trained to manage diabetes, inadequate infrastructure, equipment, tools and supplies, and essential medicines (15–17).
Furthermore, in many settings, cultural beliefs and practices can also have a positive or negative influence on how people engage with PHC systems. For instance, deeply rooted traditional beliefs of supernatural causes of disease sometimes orient patients towards traditional healing rather than PHC services (18,19); such beliefs and practices can contribute to delayed and interrupted care (18). However, cultural beliefs and practices may facilitate care-seeking if appropriately leveraged through health system adaptation and community engagement (20,21). The multifaceted interactions between cultural factors and health systems highlight the need for a comprehensive approach to successfully integrate diabetes management into responsive PHC systems, which remains an immense challenge across Africa (22).
Framework for Primary Health Care
The WHO’s PHC framework helps to understand and address the challenge of access to primary care by recognising the interdependence of three key elements: integrated health services, multisectoral policy and action, and empowered individuals and communities. These components are connected to primary healthcare (PHC) levers, such as political commitment and leadership, governance and policy structures, funding and resource distribution, and community and stakeholder involvement. When these components and levers function together effectively, they can enhance the quality, equity, and effectiveness of primary care services, ultimately resulting in improved health outcomes. However, deficiencies across multiple points in this continuum persist in LMICs, fundamentally constraining integrated diabetes care (11,23).
The literature on West Africa highlights gaps in integrated health service delivery models that do not adequately address the increasing burden of non-communicable diseases (NCDs). There is limited multisectoral coordination for diabetes prevention and a lack of community awareness and engagement in diabetes care. These factors, spanning across the healthcare system and society, significantly impact primary care for diabetes (22–24).
Quality in Diabetes Care
Quality of care is a complex, multifaceted concept that evolves through patients’ experiences. Key attributes include responsiveness to individual patient needs and preferences, quality of patient-provider interactions, and management practices (25). Hanefeld et al. argued that quality is co-produced by various actors – patients, families, communities, providers, and health systems – and shaped by sociocultural contexts (25). Realising high-quality diabetes care involves providing safe, effective, timely, efficient, equitable and patient-centred prevention and treatment (26). This requires addressing challenges at multiple levels, from health worker skills and medication availability at the health system level to social support systems at the community and individual levels. A holistic view spanning micro to macro factors is necessary to understand the various barriers and ensure quality, patient-centred diabetes care.
While previous studies have looked at the prevalence of diabetes and its risk factors in Africa, there is a notable lack of synthesised evidence on the various barriers and facilitators within primary healthcare systems that affect access to, utilisation and quality of diabetes-related primary care across West Africa (24). This lack of comprehensive understanding hinders the development of effective interventions and policy actions to improve diabetes care in the region. Our scoping review aims to address this gap by identifying and synthesising the literature on factors influencing access to, utilisation and quality of diabetes care in West Africa, exploring how and why these manifest, and distilling recommendations for strengthening PHC policy, practice, and implementation research to improve diabetes care. By providing this synthesis, we aim to inform more targeted and context-appropriate strategies for diabetes management in West African PHC settings.
Materials and Methods
This scoping review followed the methodology outlined in our published protocol (27), which adhered to the framework by Arksey and O’Malley (28), guidance from the Joanna Briggs Institute (29), and the PRISMA-ScR guidelines (30).
Two overall research questions were developed through an iterative process and extensive consultation with the research team and other stakeholders:
(1) What factors influence primary healthcare access, utilisation and quality for diabetes in West Africa?
(2) How and why do these factors work, and what are the gaps in the current literature?
The review focused on original peer-reviewed research published in English or French between January 1, 2000, and December 31, 2023. It focused on factors influencing diabetes care in the adult population, excluding gestational diabetes. The inclusion and exclusion criteria are detailed in Table 1.
The search strategy, developed with the assistance of an experienced librarian, was adapted for each database (PubMed, Scopus, Google Scholar, CAIRN Info) and utilised a combination of keywords and controlled vocabulary terms. Grey literature and reference lists of included studies and relevant systematic reviews were also searched. The search results were exported into Rayyan software for screening and management (31).
The study selection process, conducted by a team of six members who worked in pairs, involved three stages: deduplication, title/abstract screening and full-text screening. Conflicts were resolved through discussion and consensus with a third reviewer. A PRISMA flow diagram illustrates the study selection process (Fig 1).

Data extraction was performed using a standardised form in Microsoft Excel, which included study characteristics (author, year, country, design, population), barriers and facilitators to diabetes care access, utilisation, and quality at the health system and contextual levels, as well as key findings and conclusions. Four reviewers independently extracted data, which were then collated and summarised in a tabular format.
Further details of our methodology are available in our published protocol (27). Twelve papers were included in this scoping review after screening 4,290 documents.
Conceptual Framework
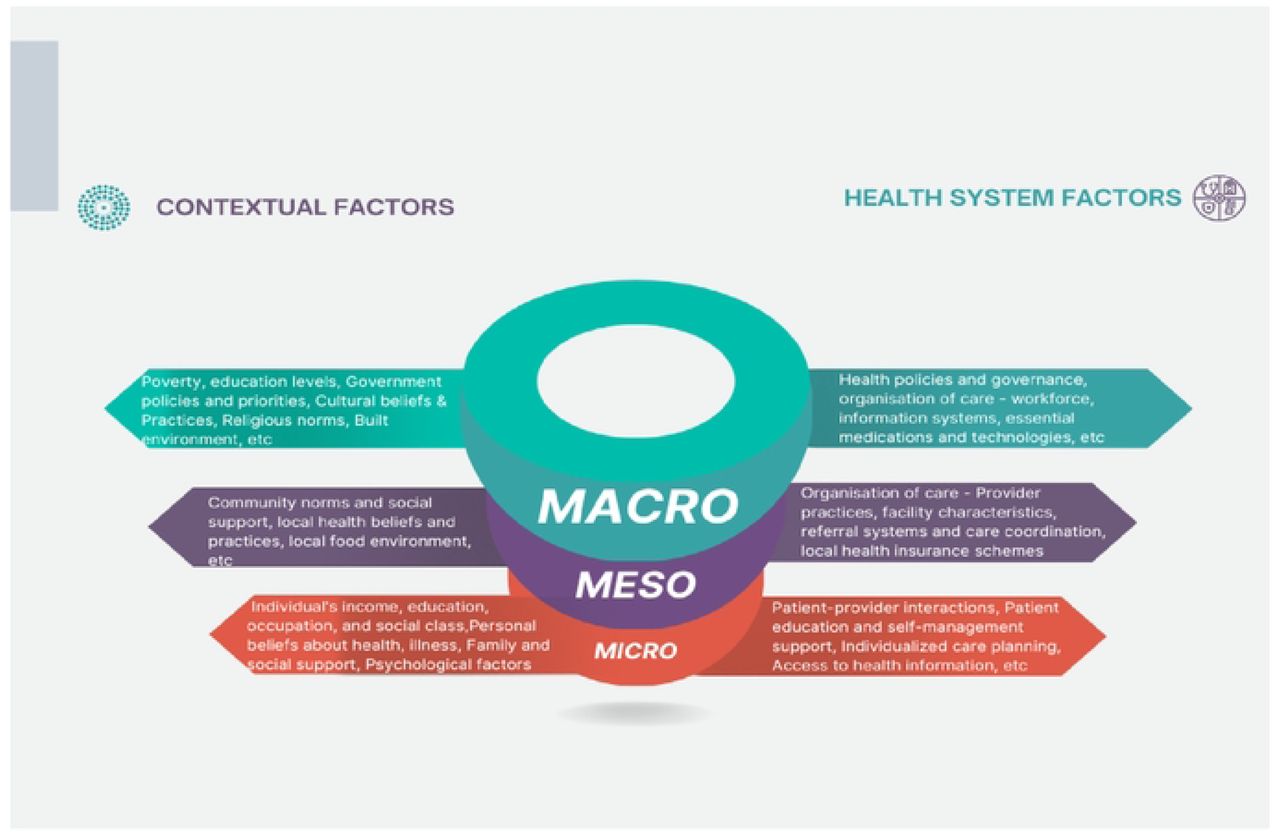
We utilised a framework analysis approach to direct the analysis process for this scoping review. To gain a holistic and context-specific understanding, various factors were analysed at the macro (broader societal, economic, political, cultural, and environmental factors influencing health and healthcare), meso (organisational and community level factors), and micro (individual patient, family, and healthcare provider level factors) levels. This taxonomy drew on multiple complementary frameworks: the Operational Framework for PHC, which is an expansion of the WHO’s six building blocks of health systems (11), the Social Determinants of Health (SDH) framework (32), and the Innovative Care for Chronic Conditions model (ICCC) (33).
These frameworks were selected because of their relevance to the complexity of diabetes care. The three frameworks we combined by examining their key domains and concepts, looking for similarities and differences. The WHO PHC framework served as the primary structure for health system components (11), while the SDH model allowed us to contextualise these within broader societal factors (32). The ICCC model offered specific insights into chronic disease management relevant to diabetes care (33). We then created a unified scheme incorporating elements from all three frameworks. For example, the ‘health workforce’ from the WHO PHC framework was expanded to include social and cultural competencies highlighted in the SDH model and the concept of a ‘prepared, proactive practice team’ from the ICCC model.
During data extraction and analysis, we applied this integrated scheme, allowing us to capture the multifaceted nature of factors influencing diabetes care. In our synthesis, we carefully considered how the findings were related to multiple framework components. For instance, a finding related to patient adherence is analysed in terms of health system factors (WHO PHC), social determinants (SDH), and self-management support (ICCC).
This synthesised approach helped us gain a better understanding of the complex factors influencing diabetes care in West African primary healthcare settings.
Our analytical framework distinguishes two main categories: contextual and health system factors across the macro, meso, and micro levels (Fig 2). Context refers to the surroundings or milieu in which a particular event or phenomenon is situated and is a crucial factor in shaping health and healthcare (34,35).

{kind=link}
{kind=link}
Results
Most of the included studies (n=7) were from Nigeria, with the remaining studies conducted in Ghana and Senegal. The study designs employed across the various studies included qualitative, cross-sectional, and mixed-methods studies, with study populations predominantly involving healthcare providers and patients.
The findings of this scoping review are organised and presented according to the integrated conceptual framework. We will explicitly link each key finding to relevant framework domains to provide a comprehensive understanding of the factors influencing diabetes care in West African primary healthcare settings (Table 2 and Table 3).
To provide a comprehensive overview of our findings and their relationship to the integrated conceptual framework, we have synthesised the key results in Table 3
Health System Factors
This review identified several barriers within the health system that contribute to suboptimal primary healthcare for diabetes in West Africa. As outlined below, these barriers include policy-related challenges, financial barriers, issues at the facility level, and workforce challenges.
Service Delivery and Organisation of Care
Our findings highlight prominent service delivery challenges, such as inadequate clinical spaces and limited avenues for diabetes education and counselling, significantly hindering the delivery of comprehensive diabetes care services (36). This issue was compounded by the absence of standardised clinical guidelines and care protocols for diabetes management at the primary care level, leading to inconsistencies in care provision and potentially suboptimal outcomes (37). Ugwu et al. found that most primary care physicians were unaware of any diabetes management guidelines, suggesting the severity of this issue (37). Furthermore, the fragmentation of services and lack of teamwork undermined the quality and continuity of diabetes care, resulting in poor feedback, coordination, and management of patient transitions across levels of care (38).
Health Workforce
Workforce challenges posed another major barrier to effective diabetes care. Shortages of healthcare professionals, particularly in rural primary care facilities, hampered effective diabetes care delivery (39). This shortage was exacerbated by the fact that frontline PHC workers often lacked up-to-date knowledge, skills, and training in evidence-based standards of diabetes care, leading to poor management of patients (40,41).
Oyewole et al. observed negative attitudes towards caring for people with diabetes among care providers, further impacting the quality of care provided (41). However, the reviewed studies did not explicitly explore the underlying reasons for these negative attitudes.
Insufficient coordination and collaborative practices among healthcare provider cadres compounded these workforce issues. Instead of adopting an integrated, consultative approach to patient care, providers often worked in silos (44). The lack of clear role assignments and poor interprofessional collaboration among different types of healthcare providers involved in diabetes care, such as doctors, nurses, dietitians, and health educators, resulted in these noticeable silos. Iregbu et al. (44) found that nurses felt underutilised and that their roles did not optimally leverage their knowledge and skills. Some doctors believed they were solely responsible for providing diabetes education with little contribution from other professionals. Referrals from doctors to dietitians were inconsistent, and doctors sometimes needed to remember to refer patients or believed they could provide dietary counselling themselves.
Similarly, Mogre et al. showed that silos existed between nurses, doctors, and dietitians/nutritionists. There was limited teamwork and cooperation across these professional groups, with more collaboration occurring within specific professionals (e.g., among nurses) rather than between different health personnel. Poor communication, lack of information sharing, competition, and perceptions of relative importance in diabetes care contributed to these silos. These professional silos primarily occurred at the provider level, reflecting a lack of integrated, multidisciplinary care teams.
Health Financing
Financial barriers emerged as a significant challenge in our review. The lack of health insurance and high out-of-pocket expenditures for medications, supplies, laboratory tests, provider fees, and related healthcare costs severely limited access to quality diabetes care (39,40,42,43). Okoronkwo et al. noted the inadequate implementation of the National Health Insurance Scheme in Nigeria, which failed to protect people experiencing poverty from the impact of out-of-pocket spending and increasing care costs (42). This issue was further compounded by insufficient funding for state-owned and operated hospitals compared to federally funded hospitals, resulting in fewer staff and limited capacity to provide comprehensive diabetes care (44). In some cases, crucial components of diabetes self-management support, such as nutrition and dietetic care, were not covered by health insurance schemes, forcing patients to pay out-of-pocket and further limiting access to comprehensive care (36).
Leadership/Governance
Several policy and governance issues undermined the provision of quality diabetes care. Authorities poorly prioritised and planned for the growing burden of chronic diseases like diabetes as health agendas continued to be dominated by infectious diseases (39). This lack of prioritisation was further worsened by high poverty rates and inadequate financial risk protection policies that limited the affordability of care (42,43). Consequently, the health system lacked the necessary resources and preparedness to manage the increasing prevalence of diabetes effectively.
Another significant challenge was the lack of a robust regulatory framework to ensure evidence-based practices and maintain quality standards in diabetes care. Ugwu et al. reported unregulated alternative medicine practices in Nigeria, which hindered effective diabetes management by promoting the use of unproven or potentially harmful treatments.
The review identified significant evidence of challenges in service delivery, health workforce, financing, and governance in primary healthcare settings in West Africa. However, there were noticeable gaps in evidence regarding health information systems and comprehensive access to essential medicines and technologies for diabetes care. However, some studies found instances of shortages in necessary resources and supplies, such as glucometers, test strips, and teaching aids, which hindered effective diabetes management (41,44).
Contextual Factors
Multiple studies reported widespread beliefs in supernatural causes of diabetes, such as curses, witchcraft, and spiritual attacks (39,40,44,45). These beliefs may lead to over-reliance on alternative medicine rather than evidence-based therapies, delaying effective diabetes management (39).
Furthermore, the dominance of carbohydrate-rich staple foods and dishes in typical West African cuisine presented a significant challenge for the dietary management of diabetes (40,45). The high consumption of carbohydrate-rich foods in West African diets was due to cultural preferences, the affordability of these staple foods compared to healthier options, and the wide availability of high-carbohydrate ingredients in local markets and cuisine. These factors posed significant challenges for adopting diabetes-friendly diets in these contexts.
Distance to health facilities was also cited as a factor influencing the choice of healthcare providers, with a significant proportion of respondents more likely to utilise facilities nearby (46).
Interestingly, while some cultural beliefs posed barriers, family and social support systems emerged as critical enablers deeply rooted in sociocultural norms. Women were identified as playing a central role in leading household dietary modifications for diabetes management, leveraging their traditional responsibilities in food preparation and family caregiving (44). However, the impact of family dynamics was not uniformly positive. The lack of social support also contributed to treatment non-adherence and difficulties in implementing lifestyle changes in specific contexts.(45). These findings emphasised the interplay of cultural beliefs, gender roles, and family structures and their influence on diabetes care.
At the behavioural level, patients’ preferences for traditional medicine over biomedical care and delays in care-seeking (albeit often related to high costs of care) were found to be significant barriers to effective diabetes management (44). Crucially, mental health emerged as a critical psychosocial determinant shaping health outcomes for diabetes. The study by Kretchy et al. highlighted the multifaceted nature of diabetes-related distress and its strong association with poorer self-management behaviours and decreased medication adherence in the Ghanaian context.
The findings also revealed that diabetes distress stemmed not only from the burden of the illness itself but also from its wider psychosocial ramifications (47). Notably, the study shed light on how people living with diabetes experience psychological distress due to poor social support, concerns related to meeting dietary requirements, and the risks of developing complications, leading to significant psychological turmoil. The psychological impact thus extended beyond individual concerns to include socioeconomic well-being.
Furthermore, dissatisfaction with external support from healthcare providers and social networks was found to be a significant component of diabetes distress. Patients who did not receive support from their caregivers and care providers were more likely to experience distress and have poorer medication adherence.
Discussion
Transforming Diabetes Care – Insights from a PHC-Centered Analysis
Amidst the rising burden of NCDs in LMICs, our scoping review explored the factors influencing access to, utilisation of, and quality of diabetes care in West African primary health systems. This review catalogues barriers and facilitators and unravels the intricate connections between health systems, sociocultural contexts, and individual experiences that shape diabetes care. Our findings also highlight the importance of deeply rooted cultural beliefs and the lived experiences of both patients and providers.
As we discuss results, we aim to map out a future that recognises the unique complexities of the West African context while drawing on other, primarily similar global contexts to improve diabetes care in resource-constrained settings.
Our analysis of diabetes care in West Africa is grounded in the synthesis of three complementary theoretical frameworks: the WHO Operational Framework for Primary Health Care (PHC), the Social Determinants of Health (SDH) model, and the Innovative Care for Chronic Conditions (ICCC) model. This multi-framework approach provides a comprehensive lens through which we interpret our findings and develop recommendations. By leveraging the strengths of each framework, we create a more robust analytical tool for understanding and addressing diabetes care in West Africa.
This synthesis allows us to capture the complexity of diabetes care in LMICs, addressing challenges such as fragmented health systems, the impact of social determinants on diabetes management, and the integration of traditional healing practices. Our findings suggest that these frameworks, when adapted to LMIC contexts, can provide a more in-depth understanding of diabetes care challenges. For instance, the ICCC’s emphasis on patient and family involvement is enriched by considering the gendered aspects of care prevalent in West African contexts.
The multi-framework approach enables us to interpret our results using established theoretical constructs and contributes to the evolution of these frameworks for better applicability in diverse global health contexts.
Strengthening Integrated Health Services for Diabetes Care – The Challenges, The Opportunities
Our review reveals profound health system barriers impacting diabetes care in West Africa. Inadequate infrastructure, lack of standardised guidelines, and fragmented services compromise access to and quality of diabetes care. Workforce shortages, insufficient training, and financial barriers further exacerbate these challenges. Overarching these issues are policy gaps, with chronic diseases often deprioritised. Despite these challenges, we uncover critical leverage points to improve diabetes care, potentially leading to fundamental change in resource-constrained settings.
Addressing Work force challenges and Care Fragmentation
In West Africa, the ‘ideal’ integrated PHC system is unique. Healthcare providers often navigate the intersection of biomedical approaches and traditional healing practices in diabetes management. This dual paradigm necessitates reimagining patient education and adherence support rooted in local sociocultural structures.
Although West Africa’s health system barriers share commonalities with other LMICs, they manifest in ways that challenge conventional global health models. For instance, workforce shortages transcend numerical deficits, encompassing capacity issues and competing health priorities. The persistent tension between addressing infectious diseases and the rising burden of NCDs exerts unique pressure on the health system, necessitating strategic resource reallocation and re-evaluations of care delivery. This dynamic connection between communicable and non-communicable disease management represents a blind spot in many global frameworks for chronic care (24). Similar challenges in resource reallocation from infectious disease programs to NCD management are evident in Southeast Asian countries like Indonesia and Vietnam (48), highlighting a broader LMIC phenomenon.
Based on our findings, care fragmentation in West Africa reveals a misalignment between long-term diabetes care needs and current primary health service structures. This misalignment, compounded by resource constraints limiting access to essential medicines and diagnostics, creates a system ill-equipped for effective diabetes management. Moreover, fragmented referral systems further worsen this issue, hindering the provision of comprehensive and continuous care for diabetes patients. Similar challenges have been observed in other regions, like India and South Africa (49,50), where efforts to integrate diabetes care into primary health services have faced implementation barriers, particularly in coordinating care across different health system levels and contributing to poor health outcomes.
The ICCC model’s emphasis on prepared, proactive practice/care teams requires substantial reinterpretation in regions like West Africa. Preparedness in these regions extends beyond clinical knowledge to encompass cultural competence and resource-constrained problem-solving. This calls for rethinking health workforce training and fostering adaptability and innovation beyond standardised guidelines. Addressing diabetes care in LMICs demands more than merely adapting existing care models. It requires a complete rethinking of delivering chronic care, considering local realities, and strategically using global best practices.
Adapting Global Best Practices to Local Contexts
While global recommendations and best practices provide valuable guidance for diabetes care, our findings assert the critical importance of translating these into locally relevant and feasible interventions. This adaptation process must consider West African countries’ unique challenges, resources, and sociocultural contexts. For instance, while comprehensive, the WHO’s Package of Essential Noncommunicable (PEN) disease interventions may need significant modification to fit the West African context. Our review highlighted the prevalence of beliefs in supernatural causes of diabetes, utilisation of traditional medicine and the dominance of carbohydrate-rich diets, necessitating culturally sensitive adaptations.
Adapting the PEN package could involve several key strategies. Diabetes education programs could acknowledge traditional beliefs while integrating biomedical explanations. Additionally, nutritional guidance could focus on modifying traditional West African dishes to be more diabetes-friendly. This approach is similar to efforts in the US to adopt the DASH diet for African American communities (51). Furthermore, the decisive role of family support systems identified in our review suggests that family-centred diabetes education could be more effective than individual-focused approaches, aligning with successful community-based interventions in other developing regions (52).
The adaptation process must be context-specific and involve key elements such as stakeholder engagement, pilot testing, and continuous evaluation. Including patients, healthcare providers, traditional healers, and community leaders in the adaptation process ensures relevance and acceptability.
Implementing adapted interventions on a small scale allows for assessing feasibility before a broader rollout. Regular evaluation of the effectiveness of these adapted interventions will enable iterative improvements over time.
Multisectoral Policy and Action, People and Communities – The Broader Determinants
While addressing health system barriers is crucial, our review uncovered the profound impact of factors beyond the health sector on diabetes care in West Africa. A multisectoral lens reveals how finance, education, urban planning, and agriculture policies significantly influence diabetes care.
For instance, our review revealed that the lack of financial risk protection mechanisms, such as comprehensive health insurance schemes, directly correlates with reduced access to diabetes care and poorer health outcomes. The lack of financial risk protection mechanisms directly correlates with reduced access to diabetes care and poorer health outcomes. This misalignment between health system structures and socioeconomic realities undermines broader health equity and universal health coverage aspirations (53,54). LMICs face unique hurdles due to high poverty rates and limited formal employment sectors, which complicate the implementation of health insurance models (55).
Our review highlights several promising examples of intersectoral collaboration, demonstrating the transformative potential of coordinated action. The implementation of “sin taxes” on unhealthy products in the Philippines, ingeniously generating revenue for health programs, including diabetes prevention, stands out as a beacon of innovative policy (56). Equally compelling is Rwanda’s expansion of community-based insurance schemes, which have significantly reduced out-of-pocket expenses and improved healthcare access for vulnerable populations (57). These initiatives emphasise that successful Universal Health Coverage requires collaboration across sectors to establish sustainable financing mechanisms and prioritise PHC in national budgets (58).
Complementing financial risk protection strategies with intersectoral actions that address the social determinants of health is important. Education, housing, and transportation sectors play crucial roles in creating environments that promote or hinder healthy lifestyles. The “Ciclovia” program in Colombia serves as an example of how urban planning can encourage physical activity and offers an adaptable model for LMICs (59,60). Such initiatives transform cities from contributors to the NCD epidemic into active partners in health promotion.
As we shift our focus to empowered people and communities, we must rethink the connection between health systems and those they serve. The success of interventions at the system level is tied to their capacity to involve and empower individuals and communities as active partners in preventing and managing diabetes. The connection between system factors and community empowerment requires a comprehensive, system-based approach to enhance diabetes care in low– and middle-income countries (LMICs). This approach should acknowledge the interdependence of all PHC components and utilise local strengths and cultural resources to develop sustainable, contextually suitable solutions.
Empowering People and Communities
Our exploration of cultural beliefs and traditional medicine practices provides further insight into our second research question, illustrating how these factors shape diabetes care. The widespread influence of cultural norms and alternative medicine on care-seeking behaviours demonstrates the intricate relationship between sociocultural contexts and health system utilisation.
Cultural Beliefs and Traditional Medicine
The influence of cultural beliefs, social norms, and complementary and alternative medicine on diabetes care-seeking behaviours in Africa is widely recognised (61,62). Rather than viewing these factors as obstacles, they present unique opportunities for creating culturally resonant care models. The systematic study by Zeh et al. (63) highlights the significance of cultural relevance in diabetes care and pushes us to rethink this in various contexts.
Cultural sensitivity remains crucial even in situations of trans-migration. A study of Korean Americans showed improved glycemic control when community health workers had culturally tailored training (64). This example calls for integrating cultural competence into healthcare delivery, linking biomedical and traditional care systems.
Studies in Tanzania and ASEAN countries further highlight the role of traditional medicine in diabetes management, emphasising the need for culturally sensitive interventions (65,66). These indicate the importance of developing culturally appropriate health promotion strategies that engage community stakeholders to raise awareness about diabetes and promote timely care-seeking.
By leveraging cultural beliefs and traditional practices, we can empower communities to take ownership of diabetes prevention and management, fostering sustainable, context-appropriate solutions.
Mental Health and Psychosocial Aspects of Diabetes Care
While cultural factors significantly influence diabetes care, our review also reveals the critical dimension of mental health, particularly in LMIC settings such as West Africa. The manifestation of psychological vulnerability as burnout, low motivation, and disengagement from treatment (67) points to a cyclical pattern where poor mental health further deteriorates glycemic control. The psychological impact of diabetes extends far beyond the burden of self-care routines, encompassing complex psychosocial dimensions that are often overlooked in traditional care models.
Our review found that diabetes distress is deeply intertwined with sociocultural expectations and economic realities. Kretchy et al. revealed how diabetes can undermine one’s sense of identity and social value, particularly among male patients struggling to fulfil traditional breadwinner roles (47). Similar findings in other cultural contexts, such as among Hispanic men in the U.S. (73), highlight the universal nature of this challenge. Moreover, the psychological burden often extends to the entire family unit.
Diabetes-related financial stress significantly impacts family dynamics and the mental health of both patients and caregivers (74).
A growing body of evidence asserts a bidirectional relationship between diabetes and mental health disorders (68,69), with comorbidities significantly impairing self-management behaviours (70). The chronic nature of diabetes and its associated complications contribute to substantial psychological distress and diminished quality of life(71,72), hence creating a cycle of deteriorating physical and mental health.
Addressing the mental health aspects of diabetes care is crucial for empowering individuals to manage their condition effectively, emphasising the need for holistic, person-centred approaches to diabetes care.
Gender Dynamics in Diabetes Management
Just as mental health plays a crucial role in diabetes management, our review also uncovered significant gender dynamics influencing care. Women’s central role in leading household dietary modifications for diabetes management, leveraging their traditional responsibilities in food preparation and family caregiving, is a crucial finding resonating across many cultures, particularly in Africa and other LMICs (44). This observation serves as a springboard for understanding the interactions between gender and diabetes care.
Women’s pivotal role in dietary management significantly influences household nutrition, shaped by local cultural norms and socioeconomic factors (75). However, this responsibility is a double-edged sword, empowering women to lead health-promoting changes and adding to their substantial caregiving burden. Research in South Africa and among Black and Latina women in the U.S. highlights how women with diabetes often struggle to balance their own health needs with caregiving roles (76,77). This struggle is exacerbated by economic constraints, with studies across Africa revealing that women are more likely than men to forgo treatment due to financial limitations (76,78) – a pattern also observed in other LMICs like India (79).
The impact of cultural beliefs and gender roles on diabetes management illustrates the emphasis of the SDH model on sociocultural factors affecting health. These deeply ingrained factors in West African societies highlight the importance of diabetes care strategies that consider both the clinical and broader social context of health.
In essence, the provision of diabetes care in LMICs is influenced by a complex interplay of factors that involve community-level dynamics and broader systemic issues – an intricate web of interactions at macro, meso, and micro levels. For example, macro-level health financing policies directly impact meso-level health system capacities, affecting micro-level patient experiences. Resource scarcity at the meso level influences individual health-seeking behaviours, often causing patients to postpone seeking care or explore alternative treatments.
This analysis highlights the drawbacks of isolated approaches or solutions. It stresses the importance of comprehensive strategies that tackle policy obstacles, enhance healthcare system capabilities, and consider sociocultural factors to bring about positive improvements in diabetes care at all levels in West Africa.
The Path Forward
The path forward for diabetes care in West Africa and other LMICs demands a bold reimagining of health systems and societal structures, transcending traditional boundaries. This calls for a revolutionary approach to interweaving health system strengthening, community empowerment, and multisectoral collaboration. At its core, this approach aligns with the WHO building blocks and the PHC framework while adapting to the unique challenges and opportunities in resource-constrained settings.
Central to this vision is strengthening health service delivery through innovative, context-specific strategies. We must amplify task-shifting approaches and implement a tiered strategy that trains community health workers in diabetes screening, education, and management while enhancing primary care providers’ knowledge and skills through specialised curricula and programs in areas such as dietary management of diabetes. This helps address immediate workforce shortfalls and builds a system of diabetes care expertise. Additionally, we must develop and implement context-specific clinical guidelines, drawing inspiration from successful programs like the PACK (Practical Approach to Care Kit) adopted in South Africa, Botswana, and Brazil (80–82).
These strategies should be complemented by integrating diabetes care with other primary health services, including mental health support, and aligning with global trends towards holistic care models, as seen in places like Chile (83). It is crucial to Train healthcare providers to recognise and address the psychosocial aspects of diabetes. We propose developing integrated care models incorporating mental health and traditional healing practices, ensuring evidence-based and culturally resonant care. A robust referral system leveraging digital health technologies should be a key component, ensuring continuity of care across different levels of the health systems.
The CASALUD model from Mexico offers valuable lessons in leveraging technology and community resources to improve diabetes care in resource-limited settings (84). Building on this, we recommend developing integrated diabetes information systems that combine clinical, community, and social data. This system should support patient management, population health strategies, resource allocation decisions, and policy evaluation, facilitating multisectoral action through interoperability with other sectoral information systems. Furthermore, access to essential medicines and technologies for diabetes care must be improved through strengthened supply chain management. By harnessing digital technologies for improved inventory tracking and forecasting, we can ensure a consistent supply of essential diabetes medicines and diagnostics. This technological integration aligns with the broader vision of leveraging innovation to overcome resource constraints.
We must rethink capacity building as a collaborative endeavour spanning multiple sectors, including education, agriculture, urban planning, information technology, finance, and social services (85).The multisectoral symphony can potentially redefine diabetes care. It can shift our focus from treating a disease to nurturing health-conscious societies. Envision communities where urban planners design cities that nudge citizens towards healthier lifestyles, where agricultural policies cultivate not just crops but community health, and where educational curricula sow the seeds of health literacy from early childhood.
The path forward also demands a fundamental shift in the power dynamics of healthcare, repositioning patients and communities from passive recipients to active co-creators of health. This transformation involves integrating culturally sensitive mental health support into diabetes care, implementing family-centred approaches that address the broader impact of diabetes on household dynamics and economics, and developing community-based support programs to mitigate social and economic challenges, especially for vulnerable populations like women. Engaging stakeholders through community-based education programs and peer support groups is essential. Moreover, exploring collaborative partnerships with traditional healers can foster culturally sensitive care delivery, bridging the gap between formal healthcare systems and community practices.
To support these initiatives, strengthening the health information system is crucial. Establishing clear indicators and targets and promoting data sharing across sectors will enable evidence-based decision-making and policy influence. Innovative tools like the web-based ALMA Scorecards, successfully used for other health issues in developing countries (86), can be adapted to track progress in diabetes care. Robust monitoring and evaluation mechanisms will be key to the success of multisectoral initiatives.
Future research should focus on evaluating the long-term impact of various financial risk protection models on diabetes care outcomes in West Africa, investigating the effectiveness of intersectoral interventions in addressing social determinants of diabetes in LMICs, and exploring innovative financing mechanisms to sustain diabetes prevention and control efforts in resource-constrained settings.
Leadership and governance play a critical role in realising this vision. Effective multisectoral action for diabetes care in West Africa requires strong political commitment, stakeholder engagement, and sustainable financing mechanisms. By prioritising diabetes and, by extension, NCDs on national health agendas, fostering cross-sectoral partnerships, and exploring innovative funding sources, LMICs can lay the foundation for more resilient and responsive PHC systems.
Strengths and Limitations
The predominance of studies from Nigeria in our review may limit the generalizability of findings across West Africa due to contextual variations. Secondly, the heterogeneity of study designs, populations, and settings could introduce variability and impact comparability. Additionally, the lack of formal quality assessment of included studies, consistent with the scoping review methodology, may affect the reliability of the synthesised evidence. The focus on published literature risks potential publication bias, while the time-bound evidence synthesis may have missed developments in the rapidly evolving diabetes care landscape. Despite these limitations, this review aims to offer a comprehensive synthesis, identifying critical gaps and highlighting areas for future research to advance strategies for improving diabetes primary care in West African settings.
Conclusions
Our multi-framework analysis revealed the complex landscape of diabetes care in West Africa, calling for a significant change in how we conceptualise and implement health interventions in resource-constrained settings. Our findings underscore the need to move beyond siloed approaches and embrace a systems-thinking approach that recognises the connections between health systems, sociocultural contexts, and individual experiences. This holistic perspective requires us to redefine NCDs not just as medical conditions but also as sociocultural phenomena deeply ingrained in societies.
Looking ahead, the challenge lies in translating these insights into actionable strategies. This necessitates boldly reimagining health system strengthening efforts that prioritise context-specific innovations, empower communities as active partners in health creation, and foster multisectoral collaboration. Future research and policy initiatives must focus on developing and evaluating adaptive, culturally resonant models of care that can effectively navigate biomedical and sociocultural factors shaping diabetes management in LMICs. By embracing this complexity and leveraging local strengths, we can pave the way for more resilient, equitable, and effective NCD care systems that improve health outcomes and contribute to broader social and economic development.
Data Availability
No datasets were generated or analysed during the current study. All relevant data from this study will be made available upon reasonable request
References
- 1.↵
- 2.↵
- 3.
- 4.↵
- 5.↵
- 6.
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵



