
ABSTRACT
Background Elderly patients, 65 years old and older, largely represent (>50 %) of hospital- admitted patients with acute coronary syndrome (ACS). Data are conflicting comparing efficacy of early routine invasive (within 48-72 hours of initial evaluation) versus conservative management of ACS in this population.
Objective We aimed to determine the effectiveness of routine early invasive strategy compared to conservative treatment in reducing major adverse cardiovascular events in elderly patients with non-ST elevation (NSTE) ACS.
Data Sources We conducted a systematic review of randomized controlled trials through PubMed, Cochrane, and Google Scholar database.
Study Selection The studies included were randomized controlled trials that evaluated the effectiveness of invasive strategy compared to conservative treatment among elderly patients ≥ 65 years old diagnosed with NSTEACS. Studies were included if they assessed any of the following outcomes of death, cardiovascular mortality, myocardial infarction (MI), stroke, recurrent angina, and need for revascularization. Five articles were subsequently included in the meta-analysis.
Data Extraction Three independent reviewers extracted the data of interest from the articles using a standardized data collection form that included study quality indicators. Disparity in assessment was settled by an independent adjudicator.
Data Synthesis All pooled analyses were based on fixed effects model. A total of 2,495 patients were included, 1337 in the invasive strategy group, and 1158 in the conservative treatment group.
Results Meta-analysis showed less incidence of revascularization in the invasive (2%) over conservative treatment groups (8%), with overall risk ratio of 0.31 (95% CI 0.16-0.61, I2 =0%). There was also less incidence of stroke in the invasive (2%) versus conservative group (3%) but this was not statistically significant. A significant benefit was noted in the reduction of all-cause mortality (RR 0.63, 95% CI 0.55-0.72, I2=84%) and myocardial infarction (RR 0.62, 95% CI 0.49- 0.79, I2=63%) but with significant heterogeneity.
Conclusion There was a significantly lower rate of revascularization in the invasive strategy group compared to the conservative treatment group. In the reduction of all-cause mortality and MI, there was benefit favoring invasive strategy but with significant heterogeneity. These findings do not support the bias against early routine invasive intervention in the elderly group with NSTEACS. However, further studies focusing on the elderly with larger population sizes are still needed.
I. INTRODUCTION
Based on the World Health Organization’s Global Burden of Disease report, ischemic heart disease (IHD) is the overall leading cause of death worldwide.1 Although the annual number of hospital discharges for acute coronary syndromes (ACS) in developed countries has declined slowly over the past two decades, the number has increased in developing countries.2 In the Philippines, cardiovascular disease (CVD) remains the leading cause of mortality.3 The Philippine Heart Association ACS registry reported that ACS is prevalent in the age range 51-70, with mean age group of 66 years old. 3
The most recent American College of Cardiology/American Heart Association (ACC/AHA 2014) and the European Society of Cardiology (ESC 2015) guidelines for non–ST segment elevation ACS (NSTEACS) reflect medical advancements in therapeutics and strategies of care leading to improved survival in ACS, but this was mainly observed in relatively younger individuals (<65 years of age) and in men. These guidelines emphasize intensive and early medical and interventional therapy, particularly for those at high risk.4,5,6
The 2014 AHA/ACC NSTEACS Guidelines generally recommend that older patients with NSTEACS should be treated with goal-directed medical therapy, together with an early invasive strategy, and revascularization as appropriate.5 The 2015 ESC Guidelines for the Management of ACS, on the other hand, recommend that decisions on elderly patients with NSTEACS should be based on ischemic and bleeding risks, estimated life expectancy, comorbidities, quality of life, patient values and preferences, and the estimated risks and benefits of revascularization. 6 Despite the guidelines, older patients are less likely to undergo procedures after an NSTEACS than younger patients due in part to patient and practitioner concerns about the increased risk of complications.7,8,9
Due to conflicting results of studies, lack of specific recommendations from the abovementioned guidelines, and the paucity of data on early invasive strategy versus conservative treatment for NSTEACS in elderly patients, this meta-analysis was conducted to focus on this special population to compare benefits and risks of early invasive therapy versus conservative management.
II. RESEARCH QUESTION
Among elderly patients aged ≥ 65 years old with NSTEACS, how effective is invasive strategy compared to conservative treatment in preventing major adverse cardiovascular events (MACE)?
III. OBJECTIVES
General
To determine the effectiveness of invasive strategy compared to conservative treatment in reducing MACE among elderly patients with NSTEACS.
Specific
Among elderly patients with NSTEACS, to determine the effectiveness of invasive strategy compared to conservative treatment, in 6 months (short-term) to 3 years (long-term), in reducing:
Death or all-cause mortality;
Cardiovascular mortality;
Myocardial infarction (MI);
Stroke;
Recurrent angina;
Need for revascularization.
IV. METHODOLOGY
Study Registration
Prior to the conduct of the research, the study was registered and approved by the Committee on Research (CORES) of Manila Doctors Hospital.
Criteria for considering studies for this review
The studies included were randomized controlled trials that evaluated the effectiveness of invasive strategy compared to conservative treatment among elderly patients ≥ 65 years old diagnosed with NSTEACS. Studies were included if any of the outcomes assessed were: death, cardiovascular mortality, MI, stroke, recurrent angina, and need for revascularization.
Definition of terms
Invasive strategy or early invasive strategy –Routine early (within 48-72 hours of initial evaluation) cardiac catheterization, followed by PCI, CABG, or continuing medical therapy, depending on the coronary anatomy.
Conservative treatment - Initial optimal medical management, with cardiac catheterization reserved for patients with recurrent ischemia at rest or after a non-invasive stress test, followed by revascularization if the anatomy is suitable.
Elderly patients – Patients aged 65 years or older (WHO, 2000), with or without comorbidities.
Non-ST elevation acute coronary syndrome (NSTEACS) – Unstable angina, with or without ST segment depression on electrocardiogram with normal or raised blood concentration of troponin T or I. Elevated troponin was defined as a value exceeding the 99th percentile of a normal population at the local laboratory at each participating site.
Search methods for identification of studies
Systematic computerized search (APPENDIX A) was performed using the Pubmed and Cochrane databases. MESH and free text of the following main key terms were used: “randomized controlled trials”, “elderly”, “non-ST elevation acute coronary syndrome”, “invasive strategy”, “conservative management”, “invasive strategy versus conservative strategy”, “major adverse cardiovascular events”, “all-cause mortality”, “cardiovascular mortality”, “myocardial infarction”, “stroke”, “recurrent angina”, “need for revascularization”. The last search was done on 10 August 2017.
Eligibility assessment was performed independently in an unblinded standard manner by three reviewers. The literature search identified 322 possible articles. Of these, 69 were relevant, particularly they involved studies related to ACS. Prospective cohort studies and post hoc analyses were excluded. Of the 69 articles, 55 were excluded due to different intervention since they did not involve comparing invasive versus conservative management in ACS. After assessing 14 articles for eligibility, 8 articles with different population and methods were excluded (details for the titles of the studies and reasons for exclusion are listed in APPENDIX D). One article was possibly eligible but did not report the event rates per treatment group. To access needed data in this particular study, correspondence with the author via email was done, but with no reply from the author until the time of writing. Five articles were subsequently included in the meta-analysis (Figure 1).

Assessment of risk bias of included trials
Three independent reviewers extracted the data of interest using a standardized data collection form and individually appraised each trial. The reviewers discussed the quality of included trials, outcomes to be collected, and risks of bias. Disparity in assessment was settled by an independent adjudicator. The assessment of random sequence generation, allocation concealment, incomplete outcome data, blinding of participants and personnel, blinding of outcome assessment, and intention-to-treat analysis was done using the quality scale for meta-analytic review, the Cochrane Collaboration Tool for Risk of Bias.
Data analysis
Review Manager 5.3 was used to analyze the data. Analysis of dichotomous data was done using risk ratio, 95% confidence interval, and Mantel-Haenszel method with fixed effects model. Heterogeneity between trials was tested using a standard Chi-square test and I2 statistics. The p- value of <0.10 was considered to be statistically significant and I2 of ≥50% is considered to have high heterogeneity.
Description of studies
Five randomized controlled trials involving a total of 2,495 patients met the inclusion criteria. The data on population characteristics, intervention type, and measured outcomes were extracted from each trial (Table 1). Four of the trials included elderly patients with NSTEACS aged ≥ 70 years while one trial included patients ≥ 65 years old.10 The studies compared the effectiveness of early invasive strategy (treatment group) versus optimum medical treatment (control group) in the management of NSTEACS in elderly patients.
Characteristics of included trials
In the treatment arm, four trials specified the time to intervention (4-72 hours) 10,12,13,14. Only one study did not specify the time to intervention but only mentioned “during initial admission”.11 Two out of the five trials included CABG as part of the intervention when indicated.12,13 In the control group all the trials used standard medical treatment.10-14
All trials assessed the outcome of all-cause mortality. All trials except one reported the outcome of myocardial infarction.11 All trials except two assessed the outcome of stroke.11,14 The outcomes of revascularization were reported by all except by two studies.10,11 Lastly, the events of cardiovascular death and recurrent angina were assessed only by one study.13
The Cochrane collaboration tool was used to assess the risk of bias. The random sequence generation, allocation concealment, incomplete outcome data, blinding of participants and personnel, blinding of outcome assessment, and intention-to-treat analysis were evaluated for each trial. All included trials were assessed to have low risk for bias (Table 2).
V. RESULTS
Effects of intervention on outcomes of interest
A. All-cause mortality
A total of 242 among 1338 (18 %) elderly patients with NSTEACS died in the Invasive Strategy Group; while 296 died among 1158 (26 %) patients in the Conservative Group (Figure 2). The pooled analysis of all-cause mortality showed statistically significant benefit of invasive over conservative strategy with an overall risk ratio of 0.63 (95% CI 0.55 to 0.72) but with significant heterogeneity (p value of 0.0001, I2 =84%).

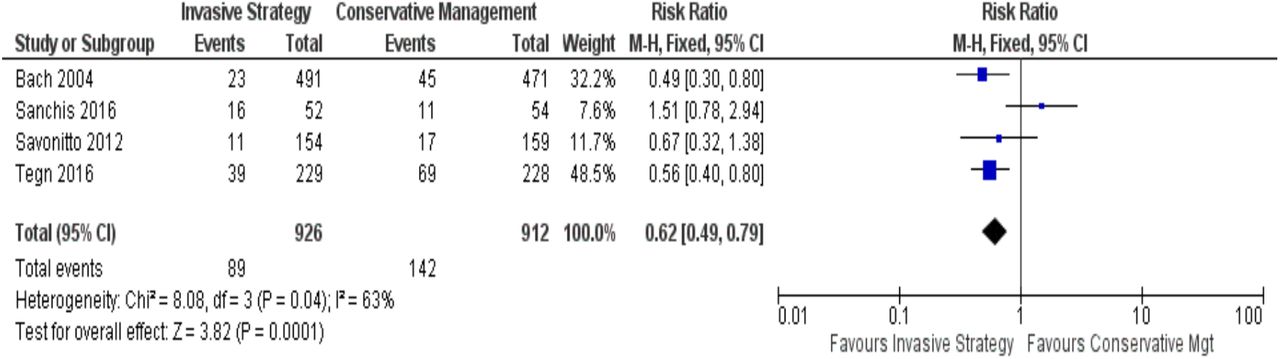
B. Myocardial infarction
In the Invasive Strategy Group, there were 89 events of MI among a total of 926 (10 %) patients; while there were 142 among 912 (16 %) patients in the Conservative Group (Figure 3). The pooled analysis showed that invasive strategy is beneficial over conservative treatment in preventing MI with an overall risk ratio of 0.62 (95% CI 0.49 to 0.79) but with significant heterogeneity (p value of 0.0001, I2 = 63%).

C. Stroke
Among the five trials, Savonitto et al. (2012), Tegn (2016), and Bach (2004) reported the outcomes of stroke (Figure 4). In the Invasive Strategy Group, there were 13 events of stroke among 874 (2%) patients; while there were 24 among 858 (3%) patients in the Conservative Group. The pooled analysis showed that early invasive strategy was favored over conservative treatment in preventing stroke but no statistically significant benefit with overall risk ratio of 0.53 (95% CI 0.27- 1.03, I2 =0%).

D. Need for revascularization
In elderly patients with NSTEACS, there were a total of 10 patients among 435 (2%) who needed revascularization in the Invasive Group while there were 34 patients among 441 (8%) in the Conservative Group (Figure 5). The pooled analysis for need for revascularization showed statistically significant benefit with an overall risk ratio of 0.31 (95% CI 0.16 to 0.61) with no significant heterogeneity (p value of 0.0006, I2 =0%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
E. Outcomes for cardiovascular mortality and recurrent angina
Among the five trials, only one trial assessed the outcomes of cardiovascular mortality and recurrent angina.13 The cardiovascular mortality incidence in the invasive versus the control group was 10% and 11 %, respectively, showing a non-statistically significant benefit of invasive over conservative treatment (RR 0.87, 95% CI, 0.49-1.56, p=0.65). Likewise, an invasive strategy showed a non-statistically significant benefit over conservative treatment in reducing recurrent angina (RR 0.81, 95% CI 0.45–1.46, p=0.49).
VI. DISCUSSION
Meta-analysis of data from the five trials included in this study showed that an early invasive strategy appears to be beneficial in suitable elderly patients ≥ 65 years old with NSTEACS. There was significantly less need for revascularization in the invasive strategy group compared to the conservative treatment group. This finding implies that more patients in the conservative group clinically worsened during their course in the ward, requiring revascularization. It is also possible that early anatomic definition of the diseased coronaries may help the attending physician optimize an appropriate evidence-based management of the patient. The studies that evaluated the outcomes of revascularization stated that the indications for revascularization in the conservative group were: positive pre-discharge stress test, poor in-hospital outcomes, recurrent ischemia, reinfarction, malignant ventricular arrhythmias, refractory angina, and heart failure.12-14 Some patients who subsequently required revascularization could have probably been better off with an early invasive approach.
For the outcomes of death and MI, an invasive strategy showed a statistically significant benefit over conservative treatment but with significant heterogeneity. The possible sources of heterogeneity for the outcomes of death and MI may be the small number of events and sample sizes. In two studies, the elderly population was just a subgroup analysis of the total population.10-11 Hence, the population in the subgroup analysis may not be powered enough to detect the differences in the intervention and outcomes of interest. Furthermore, there were differences in age cutoffs and follow-up period. Two studies had age cutoffs of 75 years11,13 while the other three studies had age cutoffs of 65, 70, and 80 years.10,12,14 Possible clinical differences in outcomes may exist in these age brackets of the elderly population. In terms of follow-up periods, two studies had follow-up of 3 years11,12; one had follow-up period of 3 months to 3 years14; one had follow-up of 1 year13; while one had follow-up of 6 months and 1 year10. However, despite the heterogeneity, data from these studies clustered on the direction towards benefit favoring invasive over conservative strategy.
In the reduction of stroke, invasive strategy showed benefit over conservative treatment but this was not statistically significant. The outcomes for cardiovascular mortality and recurrent angina were assessed only in one study13, which showed also a non-statistically significant benefit of invasive strategy over conservative treatment among elderly NSTEACS patients.
Overall, this study does not support the relatively conservative tendency when dealing with elderly patients with NSTEACS in real-life clinical setting. The elderly population is considered a high-risk group wherein more than half the mortality in NSTEACS occur5 and a more aggressive approach in suitable patients may be more appropriate and beneficial. Among people who die of ischemic heart disease, 83% were >65 years of age.1 This mortality rate is expected to increase in the forthcoming decades due to improving life expectancy of the elderly. Age is one of the most important predictors of risk in NSTEACS. Each 10-year increase in age results in a 75% increase in hospital mortality in ACS patients.15 Despite the relatively higher risk in this age group, elderly ACS patients are under-represented in clinical trials such that subjects older than 75 years of age account for less than 10%, and those older than 85 years account for less than 2% of all NSTEACS subjects. 7 This highlights the need for more clinical trials and studies in this age group.
Data from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines) registry showed that NSTEMI patients aged ≥ 65 years who experienced an in-hospital major bleed had a 33% increased risk of 30-day mortality.16 However, the advancement of equipment and technique has made PCI safer for even very elderly patients (≥ 90 years of age) with high success rates and declining major bleeding risk.17
VII. SUMMARY AND CONCLUSION
Results of this meta-analysis suggest some benefits with an early invasive strategy compared to a conservative treatment approach in the management of elderly patients with NSTEACS. There was a significantly lower rate of revascularization in the invasive strategy group compared to the conservative treatment group. A statistically significant benefit favoring invasive strategy was also noted in the reduction of death and myocardial infarction but with significant heterogeneity. These findings do not support the bias against early routine invasive intervention in the elderly group with NSTEACS.
Although an early invasive strategy may be favorable among elderly patients presenting with NSTEACS, the certainty of benefit versus risk still needs to be supported by larger clinical trials and registries with uniform age cutoff for elderly, particularly ≥ 65 years old, to provide high generalizability and statistical power. Current risk scoring systems such as the GRACE (Global Registry of Acute Coronary Events) Score, TIMI (Thrombolysis in Myocardial Infarction) Risk Score, and CRUSADE Bleeding Score are recommended in the initial evaluation of elderly patients presenting with NSTEACS. A special risk scoring may be developed to more accurately identify those who are suitable for an early invasive strategy, with an expected larger outcome and survival benefit.
Data Availability
All data are available within this manuscript.
IX. DECLARATION OF CONFLICT OF INTEREST
RRC: member of advisory board or speakers’ pool of Servier, Boehringer Ingelheim, Menarini, LRI-Therapharma, Sanofi, UAP Pharma, Unilab; MTR: member of speakers’ pool of Novartis, Servier, Astra Zeneca; the rest declare no conflict of interest.
VIII. ACKNOWLEDGEMENT
The authors would like to thank God; other consultants in the Section of Cardiology, Department of Internal Medicine, Manila Doctors Hospital; family, and friends for their support and patience in making this meta-analysis possible.
XI. APPENDIX
APPENDIX A PubMed Search Strategy
APPENDIX B Sample Data Extraction Template
Participants
Intervention
Method
Quality assessment/Risk of Bias Table
Outcomes
APPENDIX C Summary of Results of the Five Included Randomized Controlled Trials
Tegn et al., 2016. After Eighty Study
Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris (After Eighty study): an open-label randomised controlled trial
Sanchis et al., 2016.
Randomized comparison between the invasive and conservative strategies in comorbid elderly patients with non-ST elevation myocardial infarction
Savonitto et al., 2012.
Early Aggressive Versus Initially Conservative Treatment in Elderly Patients With Non–ST-Segment Elevation Acute Coronary Syndrome
Puymirat et al., 2012. FAST-MI
Use of Invasive Strategy in Non–ST-Segment Elevation Myocardial Infarction Is a Major Determinant of Improved Long-Term Survival
FAST-MI (French Registry of Acute Coronary Syndrome)
Bach et al., 2004.
The Effect of Routine, Early Invasive Management on Outcome for Elderly Patients with Non–ST Segment Elevation Acute Coronary Syndromes
APPENDIX D Excluded Studies and Reasons for Exclusion
X. REFERENCES



