
Abstract
Objectives Examine the characteristics of patient engagement (PE) practices in exercise-based randomized trials in type 1 diabetes (T1D), and facilitate T1D stakeholders in determining the top ten list of priorities for exercise research.
Design Two methodological approaches were employed: a scoping review and a modified James Lind Alliance priority-setting partnership.
Methods Published (Medline, Embase, CINAHL, and Central databases) and grey literature (www.clinicaltrials.gov) were searched to identify randomized controlled trials of exercise interventions lasting minimum four weeks and available in English. We extracted information on PE and patient-reported outcomes (PROMs) to identify if patient perspectives had been implemented. Based on results, we set out to determine exercise research priorities as a first step towards a patient-engaged research agenda. An online survey was distributed across Canada to collect research questions from patients, caregivers and healthcare providers. We qualitatively analyzed submitted questions and compiled a long-list that a twelve-person stakeholder steering committee used to identify the top ten priority research questions.
Results Of 9,962 identified sources, 19 published trials and 4 trial registrations fulfilled inclusion criteria. No evidence of PE existed in any included study. Most commonly measured PROMs were frequency of hypoglycemia (n=7) and quality of life (n=4). The priority-setting survey yielded 194 submitted research questions. Steering committee rankings identified 10 priorities focused on lifestyle factors and exercise modifications to maintain short-term glycemic control.
Conclusion Recent exercise-based randomized trials in T1D have not included PE and PROMs. Patient priorities for exercise research have yet to be addressed with adequately designed clinical trials.
Introduction
Exercise provides numerous health benefits for individuals with type 1 diabetes (T1D)1 and is an important component of diabetes self-management2. Despite vast health benefits, only one third of people with T1D meet minimum recommendations for regular exercise to achieve health benefits3. The unique barriers to exercise for people with T1D4,5 are severe, particularly loss of glycemic control and hypoglycemia. With few evidence-based strategies available to overcome these barriers, novel approaches are needed to improve the efficacy of future exercise trials to address patient-relevant concerns.
Including patients in designing and delivering research studies can help address patient-relevant gaps in clinical research6,7 such as understanding barriers to uptake of exercise among people with T1D. Patient-oriented research, being “a continuum of research that engages patients as partners, focusses on patient-identified priorities and improves patient outcomes” 8, is becoming a priority within clinical trials, but has had little traction in exercise and T1D science9. Individuals with T1D have previously been involved in a range of patient engagement10–12 (PE) or priority-setting activities13 to optimize blood glucose self-management and overall health. Notably, these studies have not centred on exercise research. The current status of PE in setting priorities for and conducting research within exercise science for individuals with T1D remains relatively unknown.
This study addresses these gaps in the literature. First, we conducted a scoping review of exercise training randomized trials for people with T1D to map patient engagement within recent trials. Informed by these results, we then engaged people with T1D, caregivers and healthcare providers in conducting a modified James Lind Alliance (JLA) model14 of research prioritization to identify the most important questions about exercise and health.
STUDY DESIGNS AND RESEARCH METHODS
Study 1: Scoping Review of Physical Activity/Exercise Randomized Trials and Type 1 Diabetes
We conducted a scoping review of published and grey literature available from the past twenty years to determine in a single narrative analysis: (1) the characteristics of exercise training interventions delivered to people with T1D and (2) the extent patient partners or patient-reported outcomes (PROMs) were involved in study development. The primary question guiding this review was “Is there evidence of patient perspectives being implemented in developing or implementing long-term exercise training trials for individuals with T1D?”
This review was conducted following the five-stage Arksey and O’Malley framework15 and formatted in accordance with PRISMA Scoping Review reporting guidelines16. A review protocol was not published prior to its conduct. Our team conceptualized PE as per the Canadian Institutes of Health Research definition as being “meaningful and active collaboration in governance, priority-setting, conducting research and knowledge translation” 8.
Data Sources
Information for this review was collected from published and grey literature. A trained university librarian (NA) developed and implemented search strategies (Appendix A). The published literature search strategy was developed for Medline and adapted to Embase, CINAHL and Central databases respectively. Database searches were conducted on August 22nd, 2018, updated on May 16th, 2019, and restricted to articles published in the preceding 20 years (January 1998 to May 2019, inclusive). Citations and abstracts for identified publications were uploaded to Rayyan QCRI review management software17 for screening.
Additionally, the Clinical Trials online registry (www.clinicaltrials.gov) was searched to identify ongoing trials (grey literature).
Included trial registrations satisfied the same inclusion criteria as published literature according to information provided. Registrations with related publications were added to the published literature analysis; otherwise, detailed aims and protocols were recorded.
Inclusion/Exclusion Screening
We included randomized controlled trials of exercise training for individuals with T1D, limiting to interventions lasting four weeks or longer to exclude lab-based acute exercise studies, which are common in exercise science. Interventions providing education to support behaviour change without directly implementing an exercise program were excluded. Full-text sources had to be available in the English language.
Screening of published literature occurred in duplicate. Two reviewers independently screened titles and abstracts from the initial (NK and AM) and updated searches (NK and NB). Conflicts following independent screening were resolved through discussions between reviewers. Full-text versions of potentially eligible articles were searched and uploaded to Rayyan software. Full-text screening was undertaken by both reviewers concurrently. The principal investigator (JM) was consulted throughout screening where disagreement remained after reviewer discussions.
Data Extraction
Publications were randomly divided between two co-authors to independently extract data (NK and AM). Where further information was required18,19, corresponding authors were contacted electronically. A data extraction form was developed in Microsoft Excel for all published and grey literature data to identify: publication information, participant characteristics, intervention details (frequency, intensity, type, time and intervention duration) and measured outcomes (extracted as per reporting within each study). Reviewers noted evidence of patient engagement if authors declared involvement of people with T1D in research question selection, study design, recruitment, data collection, data analysis and interpretation, or manuscript preparation. Finally, reviewers recorded whether PROMs were measured, as a proxy for reflecting patient-relevant research interests. PROMs included quality of life, diabetes distress, perceived competence, problem areas, self-management behaviours, frequency of glycemic symptoms and several core outcomes identified by the Irish D1 Now Study12.
Study 2: A Priority-Setting Partnership for Research in Type 1 Diabetes and Exercise
Following the scoping review, our team conducted a priority-setting partnership with patients, caregivers and healthcare providers living or working with T1D. We adapted the JLA model of priority-setting, which is supported by the Cochrane Collaboration20. This study was approved by the University of Manitoba Health Research Ethics Board (H2018:187) and is reported in accordance with GRIPP2 reporting standards for patient and public involvement in research21.
The JLA approach to priority-setting is a multi-stage, mixed-methods research design14,22, which we modified to identify priorities for exercise and T1D.
Phase 1
We created an online survey using REDCap Surveys server hosted at the University of Manitoba23,24 to collect responses to the item, “What questions about physical activity and type 1 diabetes would you like to see answered by research?” Four open-text response boxes were available for respondent submissions. Demographic (age, province of residence and relationship to diabetes) and related patient information (current age, age of diagnosis, gender and ethnic identity) were also collected. The survey was distributed across Canada for six months through partnerships developed with diabetes advocacy organizations (JDRF, Diabetes Canada and Diabetes Action Canada), social media advertising, and posters in diabetes clinics or wellness centres in several urban centres. Concurrently, 12 individuals (eight patients, three caregivers and four healthcare providers) were recruited via maximum variation sampling methods25 to participate in a steering committee. This steering committee was responsible for prioritizing submitted questions.
Phase 2
Upon survey closure (February 2019), demographic information was extracted directly from the REDCap database. Submitted questions were uploaded to NVivo 12 analysis software. A graduate student trained in qualitative research methods (NK) analyzed submissions by conventional content analysis methodology26. Four senior investigators (JMM, TAD, SDM and KMS) were consulted throughout analysis to review results and provide guidance for complicated decisions. A long-list of 38 research questions was developed for phase 3 as per JLA recommendations14.
Phase 3
Long-listed questions were distributed to the steering committee in a randomized order. Each committee member reviewed the list and ranked their top 10 questions in order of one (most important) to ten (tenth most important). Rankings were returned after the two-week review period by email in word documents encrypted with personalized passwords for each member. Rankings were collated through an inverted points-based system whereby top-ranked questions of each member were denoted ten points, and each successive ranking received one less point. Total points for each question were summed and each question receiving ten or more points (in keeping with the JLA T1D partnership) was short-listed for further prioritization.
Phase 4
A one-day in-person workshop for steering committee members was facilitated by the research team (NK, JMM, NB and JLH) to create the final top 10 list of research priorities in exercise and T1D. The goal of the workshop was to reach consensus on priority research questions, defined as every member having at least 80% agreement with the resulting top ten list. The workshop began with ice-breaker activities followed by an independent prioritization activity. Committee members were asked to individually select, in no particular order, their top and bottom three questions from the short-list.
The steering committee was then divided into three groups, each with equal proportions of representative stakeholders. Printed cards for short-listed questions were presented to committee members in categories anonymously reflecting their independent selections (ie. consensus important, less important, mixed ratings or no ratings). Each group ranked all short-listed questions in order of importance. A collated ranking from all groups was presented to members, and the full steering committee was divided into three different groups. These new groups discussed the list and re-ordered printed cards, if necessary.
The final top ten list was presented to the full steering committee. Each member anonymously rated their level of agreement from one to ten. Consensus on the final top ten list was not reached after the first two rounds of group discussions, and a third round was necessary.
Patient and Public Involvement
As per the IAP2 Spectrum of Public Participation27, patients and public stakeholders were consulted to prioritize research questions throughout three of four priority-setting project phases. All research question data were developed and prioritized by patients, caregivers and healthcare providers of individuals with T1D. These research questions will inform our future research agenda, for which we plan to collaborate with stakeholder partners.
RESULTS
Study 1: Scoping Review
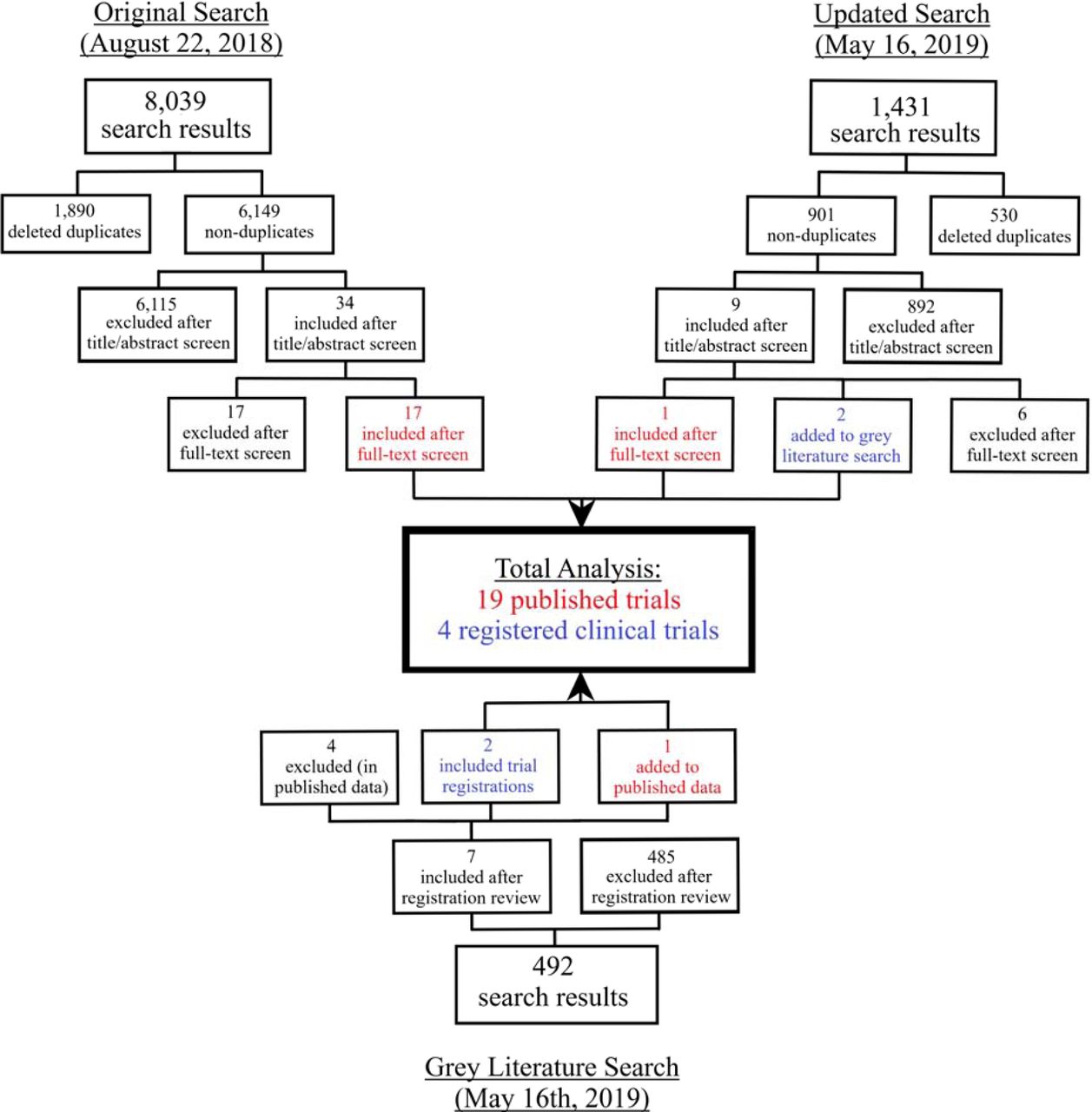
The published literature search yielded 9,470 citations (Figure 1). Following independent deletion of duplicates and title and abstract screening, 43 citations remained for full-text review. Twenty citations remained after full-text review, two of which were clinical trial registrations and added to the grey literature, leaving 18 published articles. Grey literature searches identified 492 possibly relevant registrations. After eligibility screening, seven fulfilled inclusion criteria; however, four were excluded as relevant articles were already included in the published literature analysis. One registration provided a full-text publication, and was thus added to the published literature. Therefore after screening, 19 published articles and four registered trials were included for analysis.

Published Literature
Data were available for 890 individuals living with T1D (n=18 trials reporting sample sizes). Among studies providing demographic information, 53% of participants were female (n=17 trials), 61% were children or adolescents (n=16 trials) with a mean HbA1c of 8.43% (95% CI: 7.26-9.61%, n=13 trials). Most participants were sedentary or unconditioned (n=12 trials) at enrollment and had lived with T1D for a mean of 5.5 years (median: 5.4; range: 2.9-24.4 years, n=14 studies).
Intervention summaries are provided in Tables 1 and 2. The majority of trials compared aerobic or combined aerobic and resistance training to a non-exercise control group. Interventions were delivered under supervised conditions by a kinesiologist or equivalent, for a median of 60 minutes/session (range: 10-90 minutes), three times/week (range: 1-5 times) for 20 weeks (range: 6 weeks-4 years). Twenty-three outcomes were reported across the 19 trials, of which nearly all focused on physiological factors, with glucose control and predictors of cardiovascular health being most common.
There was no evidence that any trials conducted to date engaged individuals with lived experience of T1D. Number of hypoglycemic events was the most commonly discussed PROM (n=7 studies)18,19,28–32. Additionally, episodes of diabetic ketoacidosis were indirectly observed in two studies30,32 (number of adverse events) and quality of life was measured in three studies29,33,34 (using different scales).
Clinical Trials Registrations
Across the four identified registered clinical trials35–38 (Table 3), there are plans to collect data from 187 participants. Three trials are exclusively enrolling youth participants. Planned exercise sessions frequency is a median of 3 times/week (range: 2 times/week – 3x/day, n=3 trials) for 45 minutes/session (range: 3-50 minutes, n=3 trials) lasting 15.1 weeks (range: 12-32 weeks, n=4 trials). One trial37 has reached target enrollment and anticipates publishing by the end of 2019. No trial registration described partnerships with stakeholders in developing or implementing the study. Quality of life is the only PROM explicitly disclosed in one trial38.
Study #2 - Priority-Setting Exercise
The online survey was available and advertised to the public between July 2018 and January 2019. We collected responses from 115 individuals across nine Canadian provinces. Respondents were a mean age of 40.9 (±15.1) years, and the majority (73.9%) identified as a patient with T1D. The remainder identified as caregivers (15.7%), friends (7.0%) or healthcare providers (12.2%), with some respondents identifying as more than one category (8.7%). More females completed the survey (63.4%) than males, and no participants identified as a non-binary gender. Most patients identified as being of Canadian ethnic origin (74%), with the next largest samples being European Canadian (15%), Métis (4%) and Caribbean Canadian (3%).
Of the 115 respondents, 100 submitted at least one research question, producing a total of 194 submissions. After qualitative analysis (Figure 2), 38 research questions were included in the phase 3 long-list and distributed to steering committee members for review. We received 100% of our steering committee rankings between February 21st and March 8th, 2019. Twenty-four questions were short-listed after receiving ten or more points in collated rankings.

{kind=link}
{kind=link}
Eleven of twelve steering committee members attended the Phase 4 workshop on April 6th, 2019. The workshop lasted approximately six hours. Three rounds of small group discussions occurred. Following the second round, three members did not sufficiently agree with the aggregated list. The third round resulted in slightly lower agreement for two of those members. Therefore, we conducted a post-workshop analysis using small group rankings from the third round to supplement the aggregated list from the second round. This analysis resulted in the final top ten list of research priorities for T1D and exercise (Table 4).
DISCUSSION
This study examined the characteristics of randomized trials and patient priorities for exercise science research for people with T1D. In our scoping review, we determined that patient engagement methods and PROMs have not been historically used to inform exercise-based interventions. Guided by these results, we facilitated a priority-setting project with T1D stakeholders to identify priority research questions pertaining to exercise and health. We identified that patients and caregivers are interested in modalities and strategies to exercise safely and maintain glucose control. Collectively, these findings provide a novel patient-centred rationale for designing future randomized trials of exercise interventions for people with T1D.
Previous Literature
This is the first scoping review of exercise randomized trials for individuals with T1D designed to determine if patient engagement exists in exercise and T1D literature. This topic was not addressed in recent systematic reviews of exercise training and health outcomes in people with T1D39–41. We found that exercise randomized trials published or being delivered for individuals with T1D did not focus on stakeholder engagement. This gap is not exclusive to trials of T1D and exercise. A scoping review of priority-setting practices in all health research found only 27studies engaged patients in identifying research topics, and 12 in identifying specific research questions42. Many studies simply inferred stakeholder priorities from qualitative data. Additionally, most trials engaging stakeholders do not integrate multiple stakeholders’ perspectives (ie. patients, clinicians, caregivers etc) in the prioritization process. This is an important consideration when engaging stakeholders in research, as stakeholders with different experiences of a health condition may have different priorities for research topics or outcomes43. Engaging T1D stakeholders is a significant gap in exercise science literature and should be considered within future randomized trials.
Patient engagement and priority-setting projects identifying important research topics from stakeholders’ perspectives are becoming more common within clinical research42,44,45. This project revealed that stakeholders are largely concerned with short-term outcomes, strategies to prevent hypoglycemia and stabilize short-term glucose control. This contrasts the JLA T1D treatments project13, where prioritized questions focused on long-term outcomes including adverse effects of various insulin analogues or potential cognitive impacts of living with T1D. This difference may indicate some uncertainty felt by stakeholders regarding the safety of exercise given their individual situation. Fear of short-term health complications is a common barrier to regular exercise among people with T1D5. This fear itself has a range of health implications including reduced physical activity46, increased glycemic variability46, poorer sleep patterns47 and reduced quality of life47. Although guidelines and consensus statements about prevention of post-exercise hypoglycemia exist48,49, the literature on which these recommendations are based has limitations. As this is the first investigation into patient priorities in T1D and exercise, previous research may not have been intentionally directed towards established patient-identified questions. Future randomized trials should focus on stakeholder priorities to provide optimally relevant recommendations to individuals with T1D.
Strengths and Weaknesses
This study was strengthened by using two complimentary methods to identify gaps in exercise science for individuals with T1D. Our priority-setting project followed a modified JLA approach to priority-setting. We believe the recognition and support for this model20 is a strength for our study. We were also supported by a highly engaged steering committee (100% phase 3 participation rate). Despite these strengths, several limitations should be addressed. The scoping review was limited to trials published recently and in the English language, therefore we may have missed some trials. Additionally, we were not able to achieve consensus in person at the workshop. Although the JLA Guidebook14 mentions a majority vote can be obtained in cases where consensus is not achieved, this process had to be conducted in a post-workshop analysis since several members had other commitments.
Impact of Patient Engagement
A quantitative evaluation of patient engagement was not conducted. Consulting end users as participants was integral to this study. The developed list of research questions was based on submissions collected directly from and prioritized by end users of research. Without input from patients and caregivers, prioritized research questions would likely have been very different.
CONCLUSION
We have outlined the current status of patient engagement in exercise research for individuals with T1D and engaged stakeholders in developing a list of priorities in T1D and exercise research. This list of priorities will be used to guide our future research agenda, and we recognize the need to continue working with stakeholders in designing future research. It will also be critical to re-evaluate priorities as new information becomes available.
Summary Box
We found no evidence of patient engagement or involvement in exercise science research for patients living with type 1 diabetes over the past twenty years
We worked with a Canadian sample of patients, caregivers and healthcare providers living or working with type 1 diabetes to develop a top ten list of priorities for future exercise science research
Current researchers interested in type 1 diabetes and exercise now have a framework of priorities set by stakeholders, which can be used to guide future research programs and result in more clinically relevant exercise science findings
Data Availability
The de-identified datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Statements
Contributorship statement
NK, JM, NA, AM and NB all contributed to the conduct of the scoping review. NK, JM, TD, KMS, SM, JY, JLH and NB contributed to the priority-setting project, in varying capacities including project planning, data collection and recruitment and data analysis. All authors contributed to writing or editing this manuscript.
Competing interests and funding statement
This study was supported by funding from the Canadian Institutes of Health Research Strategy for Patient-Oriented Research (SCA-145101) and an Applied Public Health Chair in Resilience and Obesity in Youth held by Dr. McGavock. JLH was supported by a CIHR Vanier Scholarship. KMS holds a Canada Research Chair in Integrated Knowledge Translation in Rehabilitation Sciences. JEY received personal fees and/or non-financial support from Dexcom Canada, Abbott Nutrition Canada and LifeScan Canada, outside the submitted work. NK was supported by a University of Manitoba Graduate Fellowship award. The authors do not declare any competing interests in the conduct of these studies.
Data sharing statement
The de-identified datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical approval statement
Ethics approval was not required for the scoping review. The priority-setting study was approved by the University of Manitoba Health Research Ethics Board (H2018:187).
References



