
Abstract
The Liber Mortuorum of Milan, a corpus of 366 volumes, is probably the oldest established mortality register in a large European city. Introduced in 1450 by Duke Francesco Sforza as a measure for the early containment of plague and daily compiled until 1801, it reports demographical data and causes of death, representing an outstanding source for epidemiology, socio-anthropology, and history. Addressed to ascertain and register individual causes of death, the Liber represents an example of disease monitoring and prevention. About this source, this paper describes Sforza’s health policy in 15th century Milan and analyzes the mortality in 1480, a year without plague to investigate interconnected social, historical, and epidemiological domains for interdisciplinary perspective.
Overview
This paper presents the Liber Mortuorum of Milan, an exceptional source for sociological, anthropological, historical, and epidemiological data, put in place by Francesco I Sforza (1401-1466), Duke of Milan since 1450, with the aim to timely track the occurrence of plague. Moreover, as military Sforza has a pragmatic vision of a productive society which requested, as for the soldiers, to keep people in good health, it is also important to track the situation of the health in the city. All the deaths that occurred in Milan since the spring and the summer of 1450, are registered, with an accurate description of the demographical data of the subjects and causes of the death. This enormous amount of data, collected during 350 years, and presently consisting of a corpus of 366 volumes preserved in the Archive of State of Milan, was scarcely utilized by scholars until the Seventies of the 20th Century and remains largely unexplored. Putting into priority individual trajectories rather than quantitative data for statistical purposes, Sforza’s method underlies a qualitative approach focused on a networking protocol of information where corps and individuals are equal parts of a relational environment. This accuracy in collecting personal data reflects the particular attention of Sforza to healthcare problems, which was also witnessed, a few years after, in 1456, by the founding of a large hospital, the first in Europe aimed at the cure of diseases and not at the simple accompaniment to death (Leverotti 1984) The 15th-century registers - Milan Sforza Registers (MiSfoRe) - also included, in most cases, the proximity network of the deceased person (household, neighborhood), addressed to a more effective tracking of the infected cases in the event of a plague outbreak. Such an accurate method of survey remained utmost meticulous for more than one century, and strongly contributed to facing the virulent plague epidemics which stroked the city in 1476-78 and 1483-85 (Alter and Carmichael 1999) (Vaglienti 2013) 1. Our paper offers a brief description of the reforms of health care institutions and charities in Italy during the 15th and 16th centuries, an overview of the spatial organization and mobility in the mid-15th century, and a focus on the MiSfoRe by a summary of the characteristics of the Registers. Information issued by the MiSfoRe has been used to build up a conceptual database, which is included in this paper, with an epidemiological analysis of the data concerning the year 1480, a year without plague, as an example of the current mortality in the city in the last part of 15th century.
Milan in the Sforza’s era: an overview
In 1450, the Milan inhabitants could have been about 110.000 (Chandler 1987) although this number remains controversial and possibly oversized. Considering as city an urban agglomerate with at least 10.000 inhabitants (De Vries 2013), in the 16th century Italy counted on the largest urban population in Europe 2. At the end of the 15th century, Milan was one of the major centers for the production of arms, armor, and fabrics in Europe and a trading center of primary importance, connecting northern Europe with Italy (Tucci 2011).
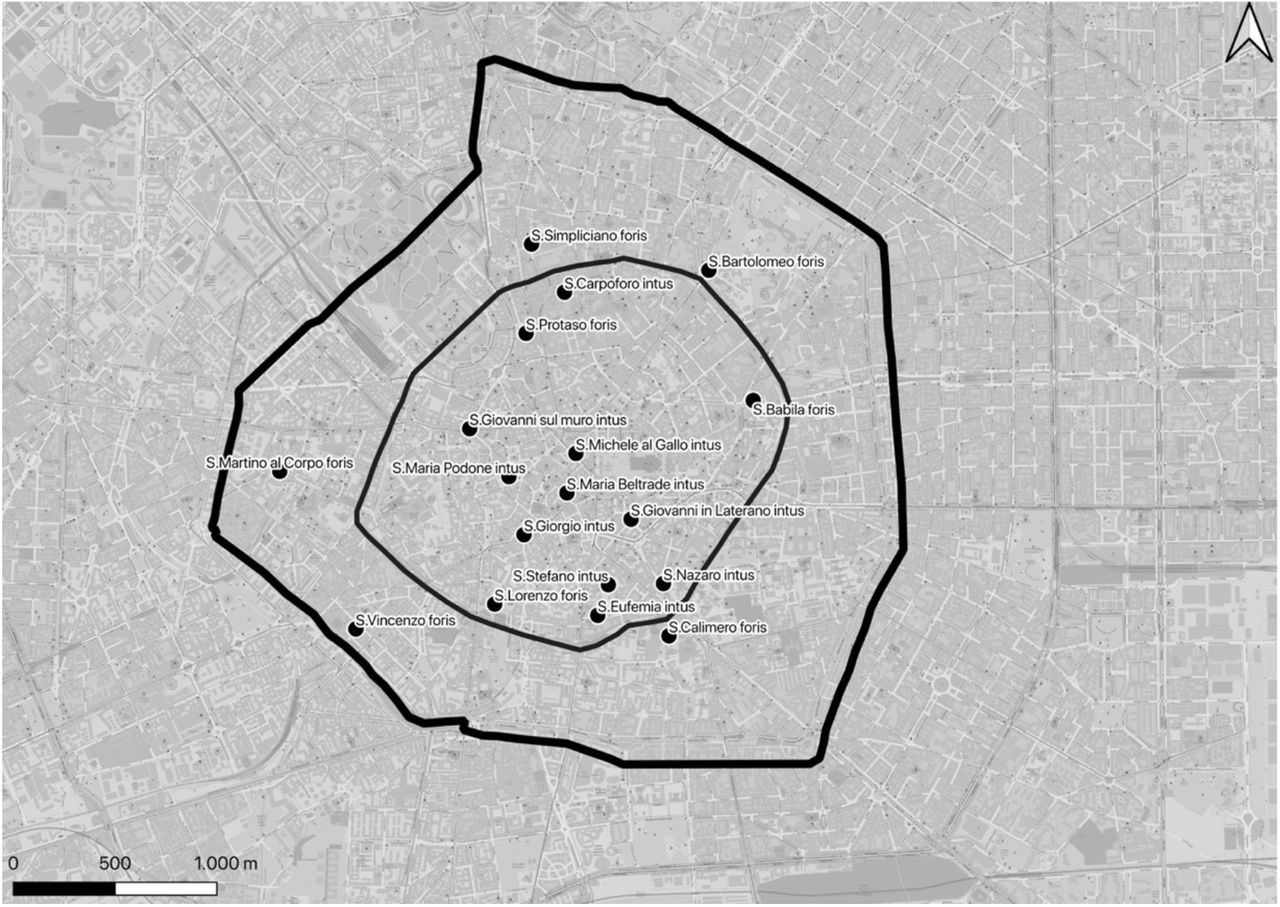
Milan’s map reflected the expansion of the city by time: Roman walls, built between the first century B.C. and the end of the third century A.C., delimited the development of the ancient Mediolanum during the Roman period and were largely destroyed thereafter. A second wall ring was built between 1156 and 1171 and included the medieval city. The building of the most recent wall ring began in 1459 with Francesco Sforza and was completed in 1560, during the Spanish domination. Of all three circles of walls, only a few remains are now visible, incorporated into the further growth of the city in modern times. The medieval city was divided into six parts, called Sestieri, each of which drew on the map of the city an irregular triangle, whose vertex was the Palazzo della Ragione, that for centuries played the role of Broletto (Municipal building) and was located in Piazza dei Mercanti, in the center of the city. The base of each triangle was along the medieval ring of the city walls. Each Sestiere was named after the corresponding Porta of the city - as originally the population of each of them was responsible for the defense of the corresponding gate on the city walls (Tucci, Ronza, and Giordano 2011). They were subdivided into five Contrade, which were contained in the second (medieval) ring of walls (Fig.1). One of them, not necessarily the Contrada closest to the city center, but probably the richest one, bore in each Sestiere the denomination of “noble” (Milano Città Stato, 2020).

The position of the Contrade in the city of Milan along with the distribution in the Sestieri. The position of the medieval walls and the Spanish walls are also represented.
The city doors were called, going clockwise starting from the North, Porta Nuova, Porta Orientale, Porta Romana, Porta Ticinese, Porta Vercellina, Porta Comasina. Originally located on the second ring of walls, each door of the city was transferred thereafter on the new wall. The part of the city included between the second and third wall was divided among the Porte, but not attributed to the Contrade. Table 1 reports the names of the Contrade, their surface in square meters, the Sestiere they belong to, and the number of parishes located in each of them along with the name of the parishes.
The Contrade of Milan, their surface, the Sestiere to which they belong, and the number of parishes whose reference church was located in the territory of each of them. The names of the parishes in each Contrada are also presented.
This division in Porte did not reflect the social organization of the city in the second half of the 15th century, which was mainly based on parishes (Colombo 1955). Organized on religious criteria and needs, each parish could include, particularly in the central part of the city, territories belonging to two or more different Porte or Contrade.
In the mid of 15th century, many large parishes were located inside the medieval walls, and most parts of the population lived outside the medieval ring of walls and did not territorially belong to a Contrada. Moreover, neither a defined pattern of distribution of different social classes residences in the city territory nor an evident separation among them could be found, even if nobles and wealthy people’s homes were concentrated in the central part. Moving to the peripheral areas, the social conditions of the inhabitants became increasingly less wealthy. Nevertheless, four concentric centers were somewhere defined: the first, the central one, was the commercial center of the city with the majority of the shops and homes of merchants and retailers. The second one was mainly a residential area with the houses of noble and wealthy people. In the third one there were many craft shops, especially producing textiles and weapons and armor, and trade places and stores near waterways, artificial canals called Navigli. The last area towards the periphery and outside the second ring of the walls was populated by workers and the poorest part of the citizens, even if some noble houses were also present. Churches and monasteries were scattered throughout the city but particularly concentrated inside the line of the medieval walls. Even if areas that could be considered completely homogeneous as regards the social composition were virtually absent, some parishes were predominantly inhabited by noble and wealthy people, and some streets and neighborhoods were inhabited by artisans and traders with similar activities called Mestieri. In particular, there was a radial distribution of commercial activities along the roads that connected the gates to the city center, while residential districts were located between these trade routes (D’Amico 1994).
Health reforms in Milan: the great lay hospital
From 1350, the cities and the Italian states showed a renewed interest in charity activities to affirm the legitimacy of control civil authorities over hospitals. An early example of this growing attention is the decision of the municipality of Siena to assume - since the 13th century and not without contrast - the management of Santa Maria della Scala, a hospital and shelter for pilgrims, poor and abandoned children, that was initially entrusted to the Canons of the Duomo (Cathedral). The secular authorities declared to assume the management to guarantee a correct administration of the hospital properties (Piccinni 2013) (Baron 1990).
Referring explicitly to the Siena experience, on 6 November 1401 the first Duke of Milan, Gian Galeazzo Visconti, informed the Vicario and the Dodici di Provisione (the Milan Municipality) that he had entrusted Enrico da Caresana, the former general administrator of the ducal possessions, to ensure the management of the city hospitals. In parallel, having to deal with the health emergencies related to a resurgence of the plague epidemic, the Duke appointed his official, Giovanni Rosselli, for a new charge of “health police” (offitium perquirendi et exequendi expedientia circa conservationem sanitatis civitatis Mediolani). Even if the figure of the gubernator et rector established by the Duke was undoubtedly innovative and would have revolutionized the Milanese hospital system, attributing to a single person the administration of various entities previously ruled by the Milanese Church, Gian Galeazzo’s decree never became operational, due to the sudden death of the Duke for plague in 1402. In the mid-fifteenth century, the reform promoted by Francesco Sforza and implemented, albeit in different ways, in all cities of the duchy, gave substance to the decree of the first Duke of Milan, giving place to a profound transformation and sanctioning the end of the religious “medieval” hospital. The roles, relationships, and functions of existing hospitals were redefined, new charity and assistance initiatives were implemented, the “large” or “major” hospitals experienced a deep rationalization and become more devoted to curing than to generic assistance. Even if ancient hospitals remained active, the large hospital became the fulcrum of a new way of conceiving assistance. The membership of the hospital Capitula (councils) became a prerogative of those lay noblemen to whom the administration of hospitals and the organization of the collection of alms, appeared to be a suitable instrument of social prestige. Those lay noblemen, through those actions, could also protect their social class from an unpredictable future by giving help to the pauperes verecundi, people who struggle to maintain a standard of living adequate to their prestige and who were ashamed to admit their difficulty (Albini 2016). Such attention to Sforza’s policy for the integrity of the individual in his conditions of healthiness and illness mirrors the Neoplatonician vision of Marsilio Ficino who defined the human body as copula mundi, the joining link between the hyperuranion and the earthly world. Filarete, influenced by the Neoplatonician, was called by Francesco Sforza to his court not only to strengthen the political and military power of the new lord, symbolically represented by the reconstruction of the Visconti castle at Giovia Gate - currently named thereafter Castello Sforzesco - but also to reinvigorate Milan’s vocation in helping the needy as part of a tradition of the city over the centuries. The promise of the Duke, expressed as a solemn vow to the people of Milan in 1451, to establish «a large and solemn hospital» was transferred in a decree proclaimed on 1st April 1456 and Filarete was commissioned to design the plan of the hospital building.
Discover the plague soon, inspecting every single death
In 1438, under the Duke Filippo Maria Visconti, it was provided that health professionals (doctors, surgeons, barbers, and apothecaries) should report the names of the sick persons they were caring for, while the Anziano of the parish was required to notify all the sick and dead people by a maximum of five days from the event (Albini 1982). At the beginning of the century, Duke Gian Galeazzo Visconti had already charged the Anziani of the parishes to report suspected cases of plague (Rollo-Koster 2016), including those that occurred among the members of the clergy (Cipolla 1974) (Zanetti 1976). The figure of Anziano (Elder), a layperson elected by the parishioners, represented a reference for the population of the neighborhood Three decades later, the prohibition of burials, in the absence of the regular license issued by the Health Office, called sepeliatur (literally: let them be buried), obliged the population to report any death to the competent authorities.
Francesco Sforza’s project takes the early detection of plague cases to a higher organizational level and accentuates the attention paid to individual conditions in each case of death. Moreover, the individual responsibility of health officials is emphasized and moral integrity would be warranted through personal commitment and legal liability. The officials engaged in registering the deaths in the MiSfoRe were personally responsible to ascertain the causes in front of a possible investigation by the competent judiciary. Each ring of the health chain was supposed to be professionally competent, incorruptible, and scrupulous to ensure the overall performance of the intervention. In several cases, the Registers report not only symptoms and supposed causes of sicknesses causing the death, but also the elapsed time from the beginning of symptoms and the death or the visit of the health officer, and the possible presence of symptoms in the relatives living in the same house. To note the course of the disease along with the duration of the illness was important to exclude the plague as the cause of death, which was entrusted with the compilation of a daily list of seriously ill patients. The ascertainment that the death had occurred after the fourth day was considered sufficient proof to exclude the suspicion of plague (Cohn Samuel K and Alfani 2007) The scrupulousness requested by Sforza translates into the obligation for official agents to visit sick people, including the poorest, even in periods of plague, in whatever condition they were in. Health officials were in charge of inspecting the corpses personally, collecting the deceased’s data, and registering them on the same day or within a day after death, unlike Filippo Maria Visconti’s method. The same duty was imposed on the graduate doctors for their patients who died at home. Although aimed, at the time of their establishment, at the rapid detection of plague, the MiSfoRe also reported the detail of the concomitant pathologies observed in each case, and the modalities of the violent deaths, including those caused by accidents at work. It, therefore, seems that the ducal government intended to deal also with the risks associated with certain works or environments (Vaglienti 2020a).
It is therefore clear that the MiSfoRe program implied a foreseeing vision of the community as an interdependent whole, beyond class and economic distinction. As for this, the exemption from registration of the persons deceased in the monasteries was not extended to members of the secular and ordinary clergy who died outside convents and religious institutions. A characterizing element of Sforza’s program was the inspection of the body of the deceased in their home or the place of death. Interestingly in 1449, during the brief parenthesis of the Repubblica Ambrosiana, doctors were allowed to agree with their patients on the use of their bodies for science in the event of death. This agreement, which remained valid during the entire Sforza period, testifies to the secular attitude of the Milan authorities in the mid-15th century and their openness to scientific investigation through the study of the human body. Since 1491, as soon as the completion of the 15th-century wing of the hospital allowed the preparation of a room for anatomical dissections, the Capitulus dell’Ospedale Maggiore (the council of the great hospital) of Milan established that “dei poveri venienti a morte nell’ospedale si facesse particolare anatomia a disposizione dei signori fisici e di essa anatomia si redigesse ricordo, da conservare in perpetuo nell’ospedale” (it should be given particular anatomy of the poor coming to death in the hospital at the disposal of the physicians and memory of this anatomy should be drawn up, to be kept in perpetuity in the hospital). Due to the abuses connected with the abundance of corpses for anatomical dissection in Milan, but not outside the duchy, in 1449 the Capitulus resolved to allow the dissection of corpses only following a specific authorization (Pecchiai 1926). This agreement represents another example of the attention of rulers to moral integrity regarding sick people and their death in the Sforza period.
The Health Office, to which Duke Francesco entrusted the responsibility for the compilation and conservation of the Registers, was composed of a doctor specialized in detecting epidemic diseases, a surgeon, commonly called Catelano, a barber, a carter, two gravediggers, a notary, two horsemen, three servants, a messenger in charge of carrying the death reports and, at the top, a commissioner and a variable number of deputies, with the task of preserving public health in the duchy for citizens and strangers (Cipolla 1976). In 1468 there were two deputies with authority over the entire ducal territory, Pietro Trivulzio and Franceschino di Castelsampietro, drawn respectively from the Secret Council and the Magistracy of Extraordinary Revenue, two of the highest institutional expressions of the Sforza central government (Vaglienti 2020b) ( Vaglienti 2020a) (Gamberini A 2020). Moreover, during Francesco Sforza’s government, the professionals who composed the Health Office reported directly to the Duke. The entire system of registration was based on those important figures: bill officials, parish Elders, doctors (hospital or private doctors), and the Catelano. The 15th-century ducal physicians could use the registers in the daily exercise of protecting public health because they could quickly identify the first outbreak of an infectious disease. Circumscribing the epidemic phenomenon, in addition to an appreciated saving in human lives, would have avoided the use of more drastic forms of health prevention, such as the total blocking of the circulation of men and goods. This blocking would have heavily compromised the progress of commercial traffic, on which much of the economic prosperity of the duchy rested, as well as the regular supply of the same urban markets.
The corpus of Mortuorum Libri
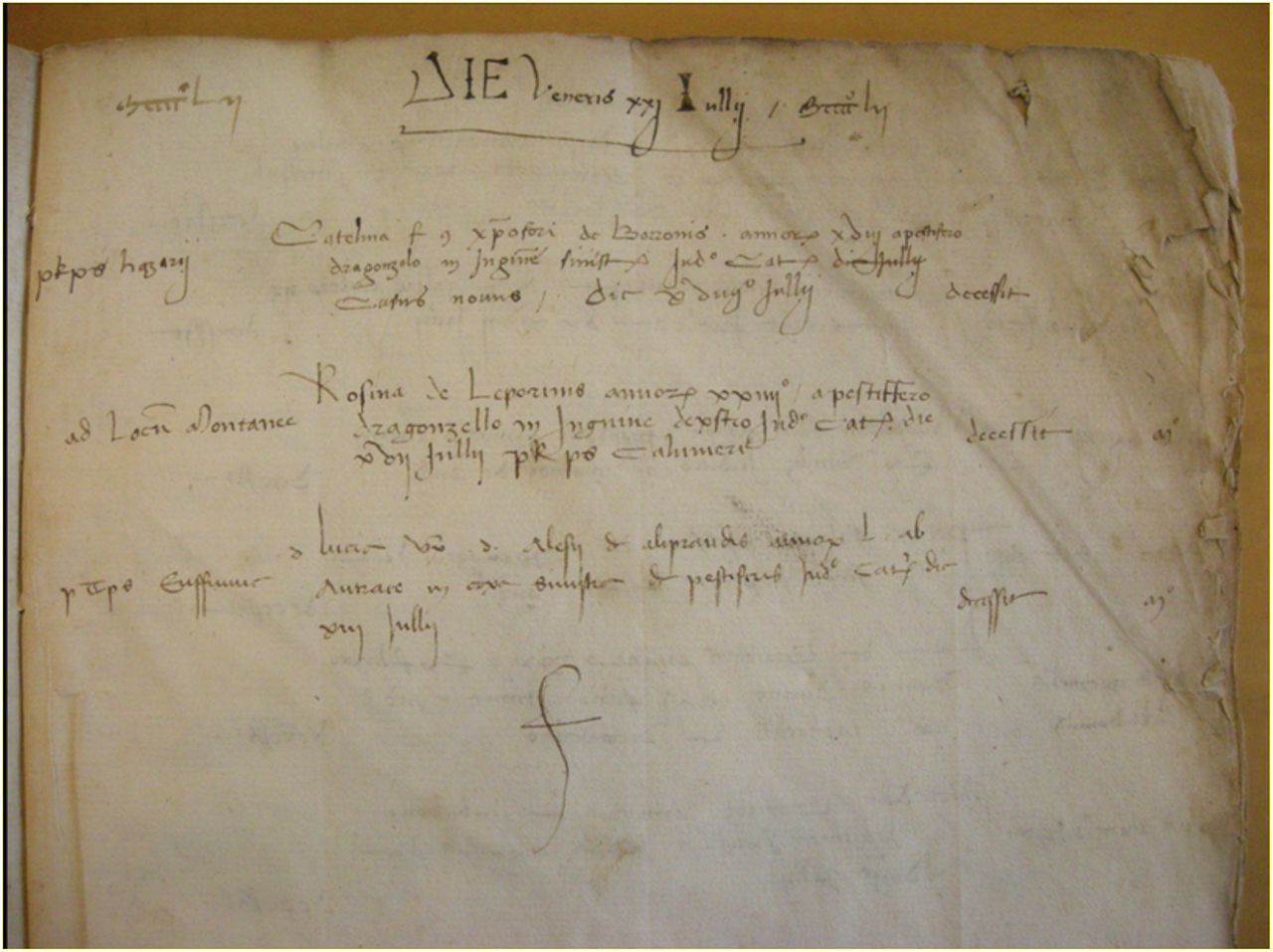
The State Archives of Milan presently holds a continuous series of 366 handwritten Registers (an example of a page of the Register of 1452 is shown in Figure 2), with only some discontinuities in the 15th and early 16th century due to the fire on the night between December 31, 1501, and January 1, 1502, of the headquarters of the Office of Health (Ufficio di Sanità), where the volumes were stored at that time. Because of this fire, the collection of the Registry in our possession started on July 21, 1452.

Sample picture of Mortuorum Libri register of 1452 (kindly authorized by State Archives of Milan).
The Registers of the 15th century were written in Latin 3. Each page reported the day and the month in which the enlisted death occurred (Vaglienti 2013) and, for each case:
to which of the six Porte the death should be attributed.
the parish where the deceased person lived or died or would be buried.
the place where the death occurred if it did not correspond to the home of the dead person (the street, a hospital, an inn, a prison).
the name, surname, or nickname of the deceased person. For children, adolescents, and unmarried women were reported (with few exceptions) the name of the father (specifying if still alive or deceased) or, if the father was unknown, of their mother. The foundlings were named hospitalis filius or filia (son, or daughter, of the hospital) or received a surname, most frequently da Milano or Colombo, with modifications in the frequency of their use and their variants over the centuries. The name of married women is often accompanied by the name and the surname of their husband. Gender is not mentioned, but with a few missing cases, it is inferable from the person’s name or from some adjectives that are used in the wording.
the social and professional status of the deceased (of the father in the case of children or the husband in the case of adult women) including titles of nobility, ecclesiastical, professional or deriving from military functions or in the administration as well as the status of servant, merchant, craftsman or worker, the condition of poverty, or the status of a prison inmate.
the age at death, expressed in years for adults, and in months, days, or even hours for infants.
the cause of death. Simply reported as plague or other than plague in the first registers, the causes of death became shortly thereafter accurately described, in some cases with a detail such as that achieved in the following sample, taken from the register of 1459: “Long-suffering of quartan fever, the night before he had a paroxysm, aggravated by an indigestion that caused heart palpitations and blurred intellect, then evolved into syncope and apoplexy that led to the death “.
the name of the official in charge of inspecting the bodies and determining the causes of death to be transcribed on the register along with all other information requested. This official could be a ‘collegiate’ doctor (indicated in this case with personal name and title) or a health official appointed to this specific duty; less frequently, the Elder of the parish or, in exceptional cases, the gravedigger.
The MiSfoRe and the others: registering mortality and morbidity in Italy and in Europe
As established in 1450, the MiSfoRe are undoubtedly older than the most renowned source of morbidity and mortality data of the European modern age, the Bills of Mortality of London. The first Bill is believed to date from November 1532. Produced intermittently in several parishes of London during outbreaks of plague, where Parsons reported the total number of plague deaths and bodies buried each week, the Bills became stably compiled in 1611, when this duty was imposed on the Worshipful Company of Parish Clerks by James I (Slauter 2011). By 1560 pairs of older women in each parish were charged with examining the dead and determining the cause of death. This choice of relying on the practical experience of those women and their knowledge of the local social context was considered adequate to the quantitative approach of recording deaths of the Bills (Boyce 2020). The clerk of the Parish Company had the task to send a copy to the Privy Council within the following day (Heitman 2020). The Bills reported for the first time a classification of the causes of death and the gender of deceased persons only in 1629, while the age at death was reported only from 1728 (Mazur 2016). It can therefore be concluded that not only the MiSfoRe were stably functioning from more than a century before the London Bills, but that through a focus on every single case of death, from the beginning including information on the age and sex of the deceased, on their social condition, on the cause of death, they represent a much richer source of information. Compared to the Bills, moreover, the MiSfoRe were the expression of a direct government intervention, mainly based on specifically dedicated health officials, with the task of issuing judgments on the causes of death of each individual and registering the date of death daily. In contrast, the Bills reported weekly and collectively the burial dates of deceased persons whose causes of death were evaluated by elderly parish women (Rollo-Koster 2016). However, even if before the plague of 1592 the reports were available only to the Privy Council, the sovereign, and the London’s Lord Mayor, thereafter the Worshipful Company of Parish Clerks began to produce a large-scale broadsheet and posting them in public areas. As a consequence, Bills of Mortality of London became the most renowned source of morbidity and mortality data, the primary source of information for public health sciences since its early origins (Heitman 2020). The identification by John Graunt, as early as 1661, of some fundamental demographic laws such as the numerical regularity of births and deaths, the relationship between the sexes at birth and death, the percentages of each cause of death relative to the total of deaths, and the consequent predictability of many biological phenomena, derives from the opportunity provided by access to the data of the Bills of Mortality (Sutherland 1963). On the contrary, the MiSfoRe have remained manuscripts and their use limited to Health Offices until 1774, three years after the beginning of the systematic surveys of the Lombard population commissioned by the government of Maria Theresa of Austria when they began to be published in print (Zanetti 1976). Despite this scholars began to be interested in them only in the 30s of the 19th century (Ferrario 1840) and incredibly this extraordinarily rich source of data remained in further long oblivion until the 70s of the 20th (C. Cipolla 1974) (Albini 1982) (Zanetti 1976). The other registers of the deaths of the main Italian cities had a similar fate. In Venice, from 1504, each parish priest must visit daily sick people living in their parish daily and must report in a book the information about the illness and if a doctor was taking care of the case. Daily information was transmitted to the Ufficio della Sanità (the Office of health) and, from 1537 to 1805, systematically reported in the Necrologi (necrologies). From 1537 to 1565 the registered data included for adult men the name, for others a more generic definition such as “a child” or “a widow”, the occupation (for adult men, for others, when provided, that of the father) and the parish. From 1565 the included data become more similar to those reported in the Milan registers, including name, surname, age, length and nature of the illness, occupation, gender, and parish. From 1731, the physicians who visited the sick people had to certify the nature of the illness, and their names were reported in the registers, but clergy remains responsible for the transmission of the information (Bamji 2016).
The Libri neri dei morti of Florence were established in 1385 by the Board of the Grascia, an agency to regulate the provisioning of the city. Compiled up to 1778, they contain the name, the paternity, the date of the deaths and the place of the burial, and sometimes age and the social status of the deceased person. From the early 17th, the occupation was added. A second register was provided by the Guild of Physicians and Apothecaries and covered the period between 1450-1808. The gravediggers, who belonged to the Guild, were the source of information, reporting the names of those they buried and the date of the death. From 1780, parishes got the task to report information about the deceased people (Parenti 1943) (Cipolla 1978). Apart from rare exceptions, there are no records on infant and children mortality. Therefore, even if the Florentine registers were established before the MiSfoRe, the data contained in them are overall less complete. Moreover, both in Venice and in Florence the registration of the dead was not a responsibility directly assumed by the state government.
In Italy, many other registers have been established to detect the presence of the plague in the city: in Mantua, for example, from 1456 there were lists of death and indications about the causes of death; in 1839 Count Carlo D’Arco makes statistical observations on them, in particular on the fluctuations of the causes of death during the year and the change in the main causes of death in the various historical periods. Verona’s registers (from 1629) were similar to those of Milan, dead people were reported day by day (women, men, and children), as well as the cause of death and socio-demographic information such as age, country, and duration of the disease.
Bologna’s registers started in 1456 and Padova’s from 1598 (Zanetti 1976). Outside Italy, Barcellona’s registers, started in 1457 (Zanetti 1976). They were constituted by the city council and for the fourteenth to the fifteenth centuries to detect the presence of the plague. At that time the recurrent epidemics were leading to the commercial decline of the Mediterranea area.
Having the exact count of plague deaths available had the advantage of not leading to exaggerations regarding the severity of the disease, and therefore to convince people to stay in the city, as well as monitoring the situation in the city that allows coping with the situation.
The information network for compiling the Barcelona registers started from the letter carrier: it had the task of obtaining and reporting daily information on the number of funerals and baptisms in each parish. It is uncertain whether these records also included infants (Smith 1936).
The Database project
The interdisciplinary approach to the Registers has implied the creation of a conceptual database to make accessible the information contained in MiSfoRe to scholars of different disciplines (e.g. historians, medical historians, anthropologists, clinicians, epidemiologists).
The importance of making information accessible has been receipted by studies about other death registers such as the Bills of Mortality of London, whose data collected from 1664 to 1849 were made accessible to any user (UK Data Service, 2020). A conceptual overview of the projected database is shown in Figure 3, where data are described in terms of entities, attributes, relations among entities, and their cardinality constraints. The main entity is the DECEASE, which represents the event of a death as recorded in the MiSfoRe corpus. Such an event is associated with a date and has a PROVENANCE, that is the reference to the specific book in the corpus where the deceased record has been retrieved. Three main contexts conceptualize a variety of other entities, each depicting the historical and interpretative background of the death event. Namely, Social Context, which is related to the people directly or indirectly involved in the death event and their mutual relations. The Geographic Context is related to the distribution of the events over the territory of the historical city of Milan. The Clinical Context is referred to the hypothesis and the causes concerning the death. In particular, two main kinds of causes, namely EVENTS (e.g., incidents, fights, murder) and DISEASE (i.e., any natural cause of death that is interesting from a clinical perspective) have been also considered.

A conceptual overview of the data extractable from the MiSfoRe.
The 1480 register: epidemiological analysis
The data entry was performed by the staff collaborating with the paleographer. The contents of the variable in the version of this study are reported in Table 2.
Variables in the 1480 database and their codification.
To obtain integrity of data collected considering the need to uniform data to perform analysis such as statistical and spatial analysis, and to obtain data correctly readable by software such as R (R Core Team 2021) the following steps were performed on the first input of data in the trial database:
The potential presence for repeated records was checked and the repetitions were removed from the dataset.
The presence of special characters was checked (for example *) in the header and the cell was checked and were removed. The recordings of missing data were codified as NA. If not, a recording of them has been carried to obtain a unique identification. If the information about the missing data could be deduced from other fields, a correction has been made (i.e.: a subject had a NA for Sex; the name of this subject was Giovannina, so the Sex could be codified as female).
A spelling or typing error correction has been performed (i.e.: A. Maria al Circolo has been corrected as S. Maria al Circolo). Those cases where the inconsistencies or errors could not be attributed to a typing were solved after an expert check.
To attempt an etiopathological classification, the causes of death reported in the register were grouped after an accurate evaluation of each case supported by the consultation of ancient treatises, with particular regard to the Libro della cura delle febbri, a treatise of the XIV century (reported by (Manuzi 1863) and to the medical treatises of Sennert (Sennert 1608) and Borsieri de Kanilfed (Borsieri de Kanilfeld 1781).
Mortality may be an important indicator of the size and socioeconomic status of the population living in each area of the city. Accordingly, it was tested whether the total mortality could be a proxy of population density in each parish and the perinatal mortality in different parishes was compared as a possible indicator of poverty.
The location of the many parish churches no longer existing has been defined as precisely as possible. Several parishes were divided into two parts, one inside and one outside the second (medieval) ring of walls (for example, San Lorenzo foris and San Lorenzo intus).
For parish churches inside the medieval walls, where not otherwise specified, the subjects were classified as “intus” and for parish churches outside the medieval walls, all subjects were classified as “foris”. According to this classification in the registry, there were 994 (54,8%) subjects codifies as “intus” (inside the medieval walls) and 819 (45,2%) as “foris” (outside the medieval walls).
Since most of the parishes concentrated in the central part of the city had an extension, as well as a population very variable, the mortality was assessed in larger and theoretically homogeneous areas such as the Contrade, attributing to each Contrada the mortality of the parishes whose church was located on their territory. Moreover, it was compared the mortality that occurred in the Contrade, inside the old walls, with the mortality in the parishes placed between them and the third circle of walls which was under construction at the time of the Sforzas.
In particular, to quantify the indicators of the socio-economic conditions territorial density was used. The territorial density of events (for all subjects and for infant and perinatal subjects) was expressed as (number of events/area of the Contrada)*1000.
For subjects with the indication of “foris” to calculate the territorial density of the same indices was consider the area between the Spanish walls and the medieval walls.
The representation of the territorial density was carried out through maps and in particular the analyzes were performed using Qgis (vers. 3.16.2) (Qgis Development Team 2021) and the basemap is OpenStreetMap (© OpenStreetMap contributors).
Mortality in Milan in 1480: results and discussion
The Register of 1480 (76/I) starts from January 23rd. It was impossible to find the recordings of the first 22 days, which should have been accessible in the ‘30s of the 19th century to Ferrario (Ferrario 1840), who reported in January 1480 a total of 170 deaths, and a total of 1938 deaths in the entire year. After excluding some double registrations, the total number of deaths enlisted in the 1480 register resulted to be 1813. Table 3 shows the comparison between the monthly deaths for each month resulting in our study to those reported by Ferrario (Ferrario 1840), Only minimal differences were evidenced, apart from the deaths that occurred in January. No significant differences have been observed in mortality in the different seasons.
Deaths monthly registered in 1480 as reported by Ferrario compared to those found in the present study.
In table 4, which presents the descriptive statistics of the distribution by age (years) at death and by gender in the 1811 subjects whose age was reported, females appear slightly older at death than males.
Age (years) at death and distribution by gender.
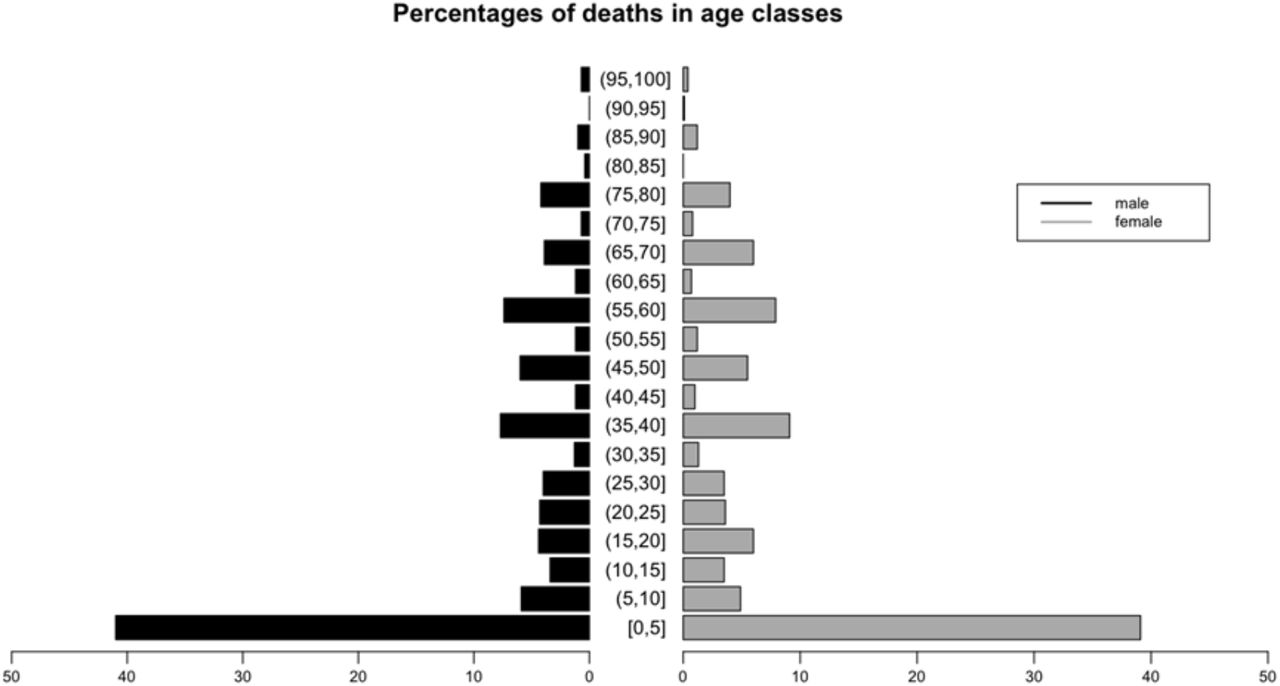
However, the mortality by gender was not significantly different in the different age classes (figure 4). It appears evident that in 1480 children aged 0-5 years paid the highest contribution to the mortality of the Milanese population, representing about 41% of the total deaths in males and 39% of those occurred in females.

Comparison of percentages of deaths in the different age classes in males and females.
Interestingly, in the 1046 subjects remaining in the analysis after excluding children younger than 8 years old, no more differences in the age at deaths between males and females were observed (Table 5).
Distribution of age (years) at the death after excluding infant mortality.
The mortality in the different parts of the city
The parishes cited in the register were 104 to highlight a marked fragmentation of the territory among them, especially in the most central part of the city. The number of deaths observed in each parish was very variable, probably due to their different size and population. Figure 5 shows the location on the map of Milan of the church giving the name to the parishes where occurred several deaths were higher than 1% of the total mortality observed.

Distribution on the Milan map of the parishes with more than 1% of the total number of deaths.
Table 6 shows the percentage of the total mortality that occurred in each parish. The highest mortality was seen in the parishes of S. Lorenzo foris, S. Protaso foris, S. Simpliciano foris, S. Nazaro intus and S. Calimero foris.
Parishes with a number of deaths higher than 1% of the total mortality.
Figure 6 illustrates the distribution of the deceased people in the Contrade taking into consideration the area of each Contrada and in the area between the Spanish walls and the medieval walls. The number and the percentage of the deceased people among the Contrade and outside the Contrade are in Table 7.

Distribution of the deceased people in the Contrade taking into consideration the area of each Contrada and in the area between the Spanish walls and the medieval walls.
The number of deaths and the percentage of the total deceased persons in each Contrada and the area outside the Contrade. The denominator was the subjects in the registry.
The causes of death
Attempting an etiopathogenic classification, the occurred deaths could be divided among 31 different natural causes and 5 non-natural / violent causes. Table 8 shows their distribution, considering only the main cause of death reported in each case by the health officers.
Deaths occurred in 1480 grouped by identified causes.
As will be discussed in more detail below, limited attention was payed in the register to detail the causes of infant death. Nevertheless, perinatal mortality was the most frequent ‘cause’ of death, and mortality in children without any specification of the causes the third. Taken together, these two ‘causes’ accounted for 35% of the observed deaths. Besides these, the causes accounting for more than 5% of the total deaths recorded causes reported were various types of fevers without the signalization of specific organ involvement, which taken together accounted for 315 cases and acute pneumonia.
Infant deaths
The deaths registered in children 0 to 7 years old were 765, of which 395 (51,6%) were observed in males and 370 (48,4%) in females. Table 9 shows the distribution of age at deaths in infants.
Distribution of age (years) at death for infants.
About 50% of the infant deaths occurred within the first year of life, and 75% before the end of the second. These data on infant mortality in Milan in 1480 are to our knowledge the oldest available today among those taken from death registers. It is known that the deaths observed in the first 27 days of life should be mainly attributed to ‘endogenous factors’ such as inborn diseases, congenital abnormality, birth trauma, or pre-term birth, while deaths occurring from the 28th day to 1 year of age are more likely to ‘exogenous causes’, such as infectious disease, malnutrition and poor living conditions (Bourgeois-Pichat 1951) (Lewis and Gowland 2007).
In Table 10 is presented the distribution of the age of subjects which had an age equal ore less than 27 days.
Distribution of age (years) at death for subjects which had and age equal or less than 27 days.
The data from Milan in 1480 are in agreement with the observations on infant mortality reported in later times. An excess of mortality in male infants has been well described both in contemporary and historic populations (Stinson 1985) (Drevenstedt et al. 2008). In particular, the relative fragility of male infants was confirmed by an analysis of data of fifteen developed countries regarding the period between the mid-18th and 1970, where the excess of male mortality increased in association with an overall decrease in infant mortality. The male disadvantage could be related to the decline of the contribution of infectious disease to infant mortality, and the decrease of this disadvantage after 1970 was due to the decline in the contribution of perinatal conditions to infant mortality (Drevenstedt et al. 2008) The number and the percentage of deaths under the age of eight occurred in each parish are reported in Table 11.
Distribution of subjects from 0 to 7 years old in parishes.
In Table 11 is presented the distribution of infant and perinatal mortality, of the subjects from 0 to 6 months old (all, females and males) and from 6 to seven years (all, females and males) for parishes. For children aged 0 to 7, the denominator is the total number of children of that age (765) and was also considered for the total number of children who died within six months of life and after six months of life. The total number of dead males within six months of life was 208, while females were 170. For the denominator of males and females who died within six months of life, the total number of subjects who died within the first six months of life was considered (378). The females who died from six months to seven years of age were 200, the males were 187. For the denominator of the males and females who died from six months to seven years, the total number of dead subjects from six months to seven years was considered (387).
The parishes with the highest perinatal and infant mortality were S. Lorenzo foris, S. Protaso foris and S. Simpliciano foris. All of them were located outside the ring of medieval walls, in the peripheral part of the city (Fig. 7).

Distribution on the Milan map of the parishes with an infant and perinatal mortality more than 1% of the total number of deaths of infant and perinatal mortality.
The poorest and probably most populous parishes had higher infant mortality and a fair excess of perinatal mortality in males. In London during 1580–1650 a higher male infant mortality was observed in poorer parishes, but not in the wealthier ones (Finlay 1981). Similarly, in the parish of Christ Church Spitalfield in London there was significant excess male infant mortality in the 1750– 59 cohort, but not in later ones (Humphrey, Bello, and Rousham 2012).
Figure 8 shows the distribution of the deceased from 0 to 7 years old among the districts taking into consideration the area of each Contrada (the value of the number of deceased divided by area was multiplied by 1000) and for the area between the Medieval walls and the Spanish walls. The number and the percentage of infant mortality among the districts and in the area outside the Contrade are in Table 12.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of the deceased from 0 to 7 years old among the Contrade and in the area outside the Contrade.
Number of subjects from 0 to 7 years old and percentage of total observed deaths in each Contrada and the area outside the Contrada (foris). The denominator was the number of subjects from 0 to 7 years old, so 765.
The distribution of infant and perinatal mortality is similar to the distribution of the mortality for all subjects.
Mortality in foundlings
The register reports a total of thirty deaths at the San Celso hospital, the foundlings’ hospice, occurred in children aged between 2 and 9 years (median 3 years) whose foundling condition is confirmed by the surname da Milano common to all of them. Even in the absence of data regarding the number of guests, it is likely that mortality among foundlings must be very high. Unlike what was observed for deaths in children occurring at their home, for which the definition of the cause of death was not defined or omitted in the majority of cases, for these foundlings, it was reported in all but three cases, three children aging two children, for whom the name of the author of the certification is also missing. On the other hand, 25 certifications were given by the same doctor, Maestro Giovanni Casetti, probably the doctor in charge of hospital care. The most frequent causes of death reported are ethical fever, with 11 cases without other association and other 5 associated with other diseases, and diarrheal diseases with or without fever in 10 cases, whose distribution during the year does not suggest that any epidemic cluster has occurred in the hospital. Four deaths are attributed to generalized edema, which in this case might be attributed to protein deficiency due to malnutrition.
Childbirth mortality
Women who died for childbirth and/ or related causes were 30 (1,7% of the total cause of death and 3.3% of causes of death of females. The percentage of deaths in childbearing age for women (15-45 years) was 229 (25.2%). The mean age for those women was 29.83 years, the median was 30 (sd=9,21).
The mean age at death was 28 years, the median was 28.5 years (sd= 5.81, min=20 years, max=40 years).
Among the women who died for childbirth mortality 12 (40%) were died in the area within the area defined by the medieval walls and 18 (60%) died in the area outside the medieval walls.
Among the women who died in childbearing age for women, 120 (52,4%) died in the area defined by the medieval walls and 109 (47,6%) died in the area outside the medieval walls.
In S. Lorenzo foris six cases have occurred, one-fifth of the total, confirming the probable populousness and possible poverty of that parish.
Not natural/Violent causes of death
There were 33 non-natural/violent deaths in the dataset, 1,8% of the total, a percentage almost identical to that detected by Dante Zanetti in the MiSfoRe of 1503 (55 cases out of 3156 deaths, 1,74%) (Zanetti 1976). Interestingly, in 2012 the percentage of non-natural deaths on the total recorded deaths in Italy was slightly higher (2,27%) and becomes quite similar if the deaths that occurred in transport accidents are subtracted from the total (ISTAT 2012). A marked difference, however, was seen in the deaths from murder, that in the Italy of 2012 were the 0,07% of the total deaths recorded, with about three-quarters of female victims, while in the Milano of 1480 the homicides represented 0.66% of the total deaths and all the murdered were males of the median age of 27 years (range 17-50), all killed by sidearms, as exemplified by the unfortunate case of Bertolino del Signore, killed at 26 a letali vulneri in radice sinistre partis colli (by a fatal wound at the base of the left side of the neck).
Due to the exclusion of suicides from burial in consecrated land, some of the deaths from suicide might have been registered as accidental, as in the case of an 18-years-old girl, registered on January 30, who died from a ‘fall from above’. An attempt to justify a suicide with a mental illness is that of Johannina famula (servant of) Magdalene de Grulis, an 18-years-old girl, registered on June 24: Semifatua nec ex toto sui iuris, se ipsa et de mente propria arsenicho venenavit et yta proprio presbitero confessa est penitentiam agens et in presentia Johannis Petri de Affori et Bernardini speciarii regis et sui famuli et Josep de Ferrariis quibus fides adhibenda est, presentibus etiam duabus matronis fidedignis (Semidiot and not totally in the full capacity of her faculties, she poisoned herself with arsenic and on her initiative and therefore she confessed to her presbyter repenting and in the presence of Gio.Pietro da Affori and Bernardino, the sovereign’s apothecary, and his servant and Giuseppe Ferrari, to whom credit must be given, also present two trustworthy married women). The health officers were not so polite with another 21-year-old girl registered on February 12: Studiose animi, incitata passione, assumpto veneno argento sublimato die martis proxime passata colirica et mortali succedente passione (With premeditation, driven by passion of love, taken for poison mercury last Tuesday, with an ensuing fatal colic attack). Among the deaths due to accidental causes, two deserve to be mentioned as they account for the accuracy of the registrations in the MiSfoRe. The first is the case of Vincenzo di (son of) Ambrogio Griffi, 23 years old qui balando cecidit super tavolam cum capite et facta forti contusione est cerebrum in 7ª (dancing he fell on a table with his head and got a severe contusion to the brain, and died in the 7th day). The second is the accident that occurred to Giacomo Pozzobonelli, a 96 years old gentleman who dead ex casu ab alto cum fractura cosse sinistre et contusione totius corporis (for a fall from above with a fracture of the left thigh and bruising of the whole body).
Deaths in hospitals
In addition to the 30 foundlings who died in San Celso, another 122 deaths occurred in a total of 11 other hospitals. Seven of them (San Dionigi, 9 deaths; San Vincenzo, 5; San Lazzaro and Santa Caterina, 4 each; San Giacomo and San Simpliciano, 3 each; Ospedale Nuovo, 2) probably functioned as parish hospital or hospices, with the only exception of San Lazzaro, dedicated to the treatment of wounds and skin diseases. Of the other four, the two largest, the Ospedale Maggiore and the Brolo hospital recorded 32 and 31 deaths respectively, while the Sant’Ambrogio hospital and the Ospedale della Pietà respectively 18 and 11. In the absence of information on the number of hospitalized persons in each hospital, it is not possible to go beyond this simple description of the data, which nevertheless confirm the presence of a widespread network of still active hospitals, destined to be progressively replaced by the large hospital wanted by Francesco Sforza.
Final considerations
This analysis is intended as a preliminary example of the possible use of the database.
The study aims is to propose an interdisciplinary approach to the MiSfoRe including Health Sciences, Human Sciences, and ICTs to provide epidemiological data within a historical and anthropological perspective.
A further aim is to apply this multi-level approach to other national sources of data on mortality and to create a network of information that could improve the knowledge of the interaction between social-demographical and biological mechanisms. The meticulousness of the description of symptoms and the information on the social context of the patients does reveal the strong relationship between individuals and the community conceived by Sforza. It would be impossible, also considering the experience of COVID-19 in Italy, in particular in Lombardy, to not envisage Sforza’s method as an example for the contemporary health protocols and policies based on proximity and a network of social ties of engagement which seem to level the social stratification of the community.
The return to the community of a virtuous historical experience appears to be of utmost importance for the rehabilitation of civil consciousness. Taking such a perspective into account, the Registers of Milan mirror sustainable social networking based on a fundamental chain of care. Presently the statistical registration for social aims and policies related to welfare and healthcare in Milan and Italy represents an example of heritage in the wake of Sforza’s reform as, for instance, registrations reported on the “Epicentro” web portal (https://www.epicentro.iss.it/#passi). Such a national attitude endorses the aims of the national healthcare system according to our constitutional principles of health as a fundamental individual right.
In conclusion, Sforza’s reform mirrored into the MiSfoRe contains, in a nutshell, the concept of health care which will be developed by the proto-industrial societies at the beginning of the 19th century. The reform exceeds, with four centuries in advance, community-oriented medical-patient management of the disease. Moreover, it anticipates the founding principles of the enlightened enterprises of the industrial era as the case of Olivetti’s firm, which in the post-war period made small and medium-sized Italian companies competitive, foreseeing a causal link between physical well-being and productivity. A centuries-old outstanding heritage is returned then to scholars and society at large thanks to the synergy between digitization of archives, epidemiology, and human sciences.
Data Availability
The data are available from the original source on the Middle-Age registers at Archivio di Stato di Milano, Italy
Declaration of interest
No potential competing interest was reported by the authors
Acknowledgements
The Authors are grateful to Dr.Benedetto Luigi Compagnoni, Director of Archivio di Stato di Milano for letting access the Mortuorum Libri
Footnotes
The paper has been revised according to the suggestions of the Editors of the journal of the original submission. The paper is now resubmitted to the same journal.
↵1 In such a period, so frequently tormented by the recurrence of the epidemics, just to give an example more than 35 treatises on plague have been published in Italy including the De peste, wrote in 1478 by Jacopo Soldi; the Trattato de la pestilentia by Girolamo Manfredi (1479), the Consilium contra pestilentia by Gentile da Foligno (1479), and De Pestilentia by Giovanni Calori. In 1481 Marsilio Ficino published the Consilio contro la pestilentia, which was republished several times between 1575 and 1580 when strong plague epidemics resurfaced (Katinis 2007) (Manfredi 2008).
↵2 (1.339.000, with 51 cities) with respect to France (688.000, 32 cities), Spain (414.000, 20 cities), Germany (385.000, 23 cities), Belgium (295.000, 12 cities), The Netherlands (150.000, 11 cities) and England and Wales (80.000, 5 cities) (Malanima 1998). In Italy, the largest city was Venice, with 150.000 inhabitants estimated in 1423 (Spruyt 1996), while Florence had 54.000 inhabitants in 1470 (Chandler 1987) and London about 50.000 in 1500 (Chandler 1987)
↵3 Registers were written in Latin before 1774 (Zanetti 1976)
Bibliography



