
Abstract
The study aimed to compare and rank the efficacy of various eating patterns for glycemic control, anthropometrics, and serum lipid profiles in the management of type 2 diabetes and prediabetes, and provide evidence for personalized clinical decision-making. We conducted a network meta-analysis using arm-based Bayesian methods and random effect models following the Cochrane handbook. We drew the conclusions using the partially contextualized framework by the GRADE working group. Twelve English and Chinese databases and registers were retrieved, and we obtained 9,534 references, of which 107 independent studies were eligible, including 8,909 participants, ten experimental diets, and thirteen outcome variables. The meta-analysis denoted that: caloric restriction was ranked as the best pattern for weight loss (SUCRA 86.8%) and reducing waist circumference (82.2%), high-fiber diets for lowering fasting plasma glucose (82.1%) and insulin (79.4%), Dietary Approaches to Stop Hypertension for reducing glycated hemoglobin (90.5%) and systolic blood pressure (87.9%), simple high-protein diets for improving insulin resistance (86.3%) and diastolic blood pressure (74.6%), low-carbohydrate diets for improving body mass index (81.6%) and high-density lipoprotein (84.0%), low-glycemic-index diets for lowering total cholesterol (87.5%) and low-density lipoprotein (86.6%), and Paleolithic diets for reducing triacylglycerol (83.4%). However, the results were of moderate sensitivity, and publication bias of glycated hemoglobin, weight, and body mass index existed. Meta-regression suggested that macronutrients, energy intake, baseline, and weight may modify outcomes differently, while the duration did not show a significant association with results. Forty-nine (39.8%) out of 123 pieces of evidence was rated as moderate quality, and there was no high-quality evidence. Additionally, only 38.2% of the effect sizes of the evidence met the minimally important clinical difference threshold. Clinicians can use the evidence to provide personalized nutrition consultations to patients according to their baseline characteristics. However, the results should be carefully explained and applied because of the sensitivity and low quality.
1. Introduction
Type 2 diabetes mellitus (T2DM) has been a major issue for all people and healthcare professionals worldwide, leading to a large proportion of health expenditure. It was estimated that 10.5% of people aged 20-75 suffered from diabetes mellitus globally, within which over 90% were T2DM, with total health spending of 966 billion US dollars [1]. Since T2DM has proven to be preventable and controllable [2], the remission of a prediabetic state (PreD), or impaired glucose tolerance (IGT), was also concerned and included in the comprehensive prevention of T2DM incidence. Dietitians and clinicians have explored diets for the remission of T2DM since the pre-insulin era [3], and nowadays, medical nutrition therapy is a universal, highly cost-effective treatment for T2DM patients with a strong evidence basis, recommended by multiple guidelines [4-6].
Eating patterns play the leading role in the entire medical nutrition therapy. Various patterns of different components and food groups have been investigated and applied to the treatment of T2DM/PreD patients, from the very high-fat diet by John Rollo in the 18th century [7] to the pattern recommended by American Diabetes Association (ADA) in 2003 [8]. From an evidence-based perspective, hundreds of random controlled trials (RCT), cohorts, and related systematic reviews have been carried out to quantify the efficacy of popular and widely-used eating patterns, e.g., caloric restriction (CR), low-glycemic-index diets (LGID), low-carbohydrate diets (LCD), and Mediterranean diets (Med) [9-14].
However, a common and prominent aspect of all evidence is that a variance of the effectiveness of eating patterns exists in improving different indicators such as blood glucose, weight, and cardiovascular risk factors. For example, Diabetes Canada 2018 guidelines [5] summarized the properties of a series of dietary interventions, pointing out the difference between diets. Consequently, diabetes guidelines strongly recommend a personalized medical nutrition therapy process under the supervision of registered dietitians and multidisciplinary professionals [4-6]. Despite the recommendation, it remains a question of how to choose and apply appropriate dietary patterns for professionals, due to the lack of evidence that directly compares the relative efficacy of different interventions. Whether a specific diet is proper for an individual with specific laboratory profiles and situations and whether it is best-matched remains unclear enough, though high-quality evidence of the effectiveness of particular patterns having been drawn.
It is not cost-effective to carry out multi-arm trials directly comparing several diets. Thus, it is crucial to conduct a network meta-analysis to synthesize evidence. Previous network meta-analyses [15, 16] have assessed a number of patterns, but the authors only included a limited number of studies and outcomes. Furthermore, short-term trials were not considered to be included in the analyses, but a short-term effect may be more common for some patterns [17]. Therefore, this study aimed to evaluate the relative efficacy of different eating patterns on glycemic control, anthropometrics and serum lipid profiles in the management of patients with T2DM or PreD, and conclude evidence to promote clinical decision-making.
2. Methods
2.1. Study Design
This systematic review was an arm-based Bayesian network meta-analysis of randomized controlled trials, following the Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 [18]. We reported the results according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses Incorporating Network Meta-analysis (PRISMA-NMA) guideline [19]. An a priori protocol was prepared and registered in PROSPERO (registration number CRD42021278268).
2.2. Eligibility Criteria
We selected peer-reviewed articles and thesis according to the population (P), interventions (I), comparisons (C), outcomes (O), and study design (S). A detailed description of the interventions is in Appendix A.
Inclusion criteria were: (1) P: Adults with type 2 diabetes mellitus or prediabetes; (2) I: The study should contain at least one arm of the interventions as follows: caloric restriction (CR), high-fiber diet (fiber), Dietary Approaches to Stop Hypertension (DASH), high-protein diet (HPD), high-fat diet (HFD), low-carbohydrate diet (LCD), low-glycemic-index diet (LGID), Mediterranean diet (Med), Nordic diet (ND), Paleolithic diet (Paleo), Portfolio diet (PfD), and vegetarian/vegan/plant-based diet (VD); (3) C: The study should contain the control arm as follows, or contain two or more intervention arms: standard diabetes diet, e.g. ADA 2003 diet [8]; ad libitum; general nutrition counselling; or placebo (no intervention); (4) O: the study should reported at least one outcome as follows, where fasting plasma glucose (FPG) was the primary outcome of this meta-analysis: glycemic control, including FPG, glycated hemoglobin (HbA1c), fasting insulin (FIns) and insulin resistance (IR); anthropometrics, including weight, body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), and body fat rate (BFR), systolic blood pressure (SBP) and diastolic blood pressure (DBP); serum lipid profiles, including triacylglycerol (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL) and high-density lipoprotein cholesterol (HDL); renal function, including serum creatinine, serum urea, serum uric acid and (estimated) glomerular filtration rate; other dichotomous outcomes, including attrition rate, remission of T2DM, incidence of hypoglycemia, incidence of drug or insulin discontinuation, incidence of T2DM from PreD; (5) S: randomized controlled trials (RCT); (6) Language: English or Chinese.
If the studies met one of the criteria below, they were excluded: (1) I: any prescribed between-group difference on exercise, antihyperglycemic medications, insulin injection, or other co-interventions; added a single supplement, or single specified food which did not provide macronutrients; or use meal replacement to provide an appreciable percentage of energy intake; or total energy intake (TEI) < 800 kcal/d (3.3 MJ/d); or the adjustment of intervention during the trial; (2) Duration: less than four weeks or one month for parallel RCTs or any phase of crossover RCTs; or intermittent intervention; (3) S: single-arm or self-controlled trials; (4) Data availability: trials not completed, or without data analysis and published reports; or articles with inappropriate or insufficient data.
2.3. Search Strategy
We conducted searches of electronic databases and trial registers: PubMed, Web of Science, Embase, CINAHL and Open Dissertation, ProQuest, Scopus, Global Index Medicus, Cochrane Central Register of Controlled Trials, Clinicaltrials.gov, SinoMed, WanFang Med, and CNKI. All publications from the inception to 13 October 2021 were initially retrieved. An updated search was conducted on March 17, 2022 using Scopus and Google Scholar after completing major data extraction works to identify the latest relevant articles. A “participants AND intervention AND design NOT exclusion” strategy was applied, using MeSH terms and free entry terms. Full search strategy can be found in File S1.
2.4. Data Selection and Extraction
All references identified from the search were imported into EndNote 20 (Clarivate, PA, USA) to move duplicates automatically and manually. After automatic exclusion using terms “Systematic Review; Meta-analysis; Cohort; Protocol; rats; gestation; pregnan*; child; adolescent; Roux-en-Y; Bariatric Surgery; mechanism; intermittent” and relevant Chinese terms, reviewers (B.-T.Z., H.-Q.P., and F.-D.L.) assessed the eligibility of publications and trials in the order of title, abstract and full text. All references were decided by at least two reviewers, and arisen discrepancies were discussed and decided by the three authors together.
We used MySQL 8.0 (Oracle Corporation, TX, USA) to perform data extraction and manage data. Basic information, study designs, arms, participant characteristics, nutrition intake, and outcome measurements at different timepoints were extracted (File S2). Two authors (B.-T.Z. and Z.-Y.Y.) independently extracted and checked the data.
R 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria) and Microsoft Excel 2019 (Microsoft Corporation, WA, USA) were used for data conversion and imputation. For continuous outcomes, we calculated the change from baseline and its standard deviation (SD) based on the baseline and the last measurement time point of each arm according to Cochrane Handbook, if not reported by the article. Correlation coefficients for changes from baseline and for crossover RCTs were estimated using reported SDs from included studies (File S3). Median and interquartile range was converted into mean and standard deviation using methods from Luo et al. [20] and Wan et al. [21] after testing for the skewness using methods from Shi et al. [22]. WebPlot Digitizer 4.5 [23] was applied for extracting data from figures. Ultimately, R package “mice” [24] (predictive mean matching or random forest method) was used for the imputation of missing values of covariates for meta-regression.
2.5. Risk of Bias Assessment
A revised Cochrane risk of bias tool for randomized trials – Risk of Bias 2 [25] and Risk of Bias 2 for crossover trials [26] were employed to assess the risk of bias (RoB) of parallel and crossover RCTs, respectively. Two reviewers (B.-T.Z. and H.-Q.P.) assessed the RoBs independently, with all arisen divergences discussed and reached consensuses.
2.6. Data Synthesis
Our study synthesized evidence through an arm-based Bayesian network meta-analysis in a random effect model. We use R package “gemtc” 1.0-1 for meta-analysis, inconsistency test, heterogeneity test, meta-regression, and sensitivity analysis [27, 28]. Markov chain Monte Carlo sampling was performed using JAGS 4.3.0 via R package “rjags” 4.12 [29, 30]. Comparison-adjusted funnel plots, Egger’s test, and Begg’s test were performed to detect publication bias under a frequentist framework and random effect model using the R package “netmeta” 2.1-0 and “metafor” 3.4-0 [31, 32].
Continuous outcomes were presented as mean difference (MD) or difference in percentage change from baseline (Percentage MD, PMD, only for fasting insulin and insulin resistance) and 95% credible intervals (95% CrI), while relative risk (RR) and 95% CrI were for dichotomous variables.
2.7. Quality of the Evidence and Drawing Conclusions
We rated the quality of evidence of comparisons of experimental diets and control diets based on the GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis [33] and the GRADE handbook [34]. Conclusions were drawn according to the partially contextualized framework for network meta-analysis by the GRADE working group [35], where minimal clinically important differences (MCID) and thresholds for moderate and large beneficial/harm effects were identified based on previous studies [14, 36-38].
3. Results
We identified 9358 publications and registrations from the initial search, and 176 from the updated search. After removing 4466 duplicates, 4164 were excluded through title screening, 600 excluded through abstract screening, and 199 excluded through full-text screening. Manual search and search of reference lists obtained 11 articles, where six were included. As a result, 111 publications [39-149] were included, among which 107 independent studies were identified (Figure 1). All excluded items through full-text screening and their reason for exclusion were listed in File S4.

PRISMA flowchart of data selection. CENTRAL, Cochrane Central Register of Controlled Trials; NCT, ClinicalTrials.gov.
Among our prescribed outcomes, data of FPG, HbA1c, FIns, IR, weight, BMI, WC, SBP, DBP, TG, TC, HDL, LDL, and attrition rate were sufficient to form networks and perform a meta-analysis. However, other outcomes were not analyzed due to insufficient data.
3.1. Study characteristics
The 107 included studies contained 8909 participants for data analysis (full-dataset, completer, or intention-to-treat analysis) and 8583 completers. A total of ten experimental diets and 223 arms was reported. The studies reported efficacy of CR, DASH, fiber, HFD, HPD, LCD, LGID, Med, Paleo, and VD, but ND and PfD were not included.
Characteristics of the studies are displayed in Table 1. Studies were from 26 countries, where 31.8% were from China, 15.0% from the USA, 9.3% from Australia, and 4.7% from Canada. We included 16 crossover RCTs and 91 parallel RCTs. Among them, seven were multi-arm, and six were multicenter. Four studies reported their outcomes in two or more publications. Only five studies focused on PreD population; considering that there was not significant difference among the PreD RCTs and the T2DM RCTs, we did not distinguish them in the meta-analysis. Fundings and conflicts of interest of the studies are listed in File S5.
Characteristics of included studies.
3.2 Risk of Bias Assessment
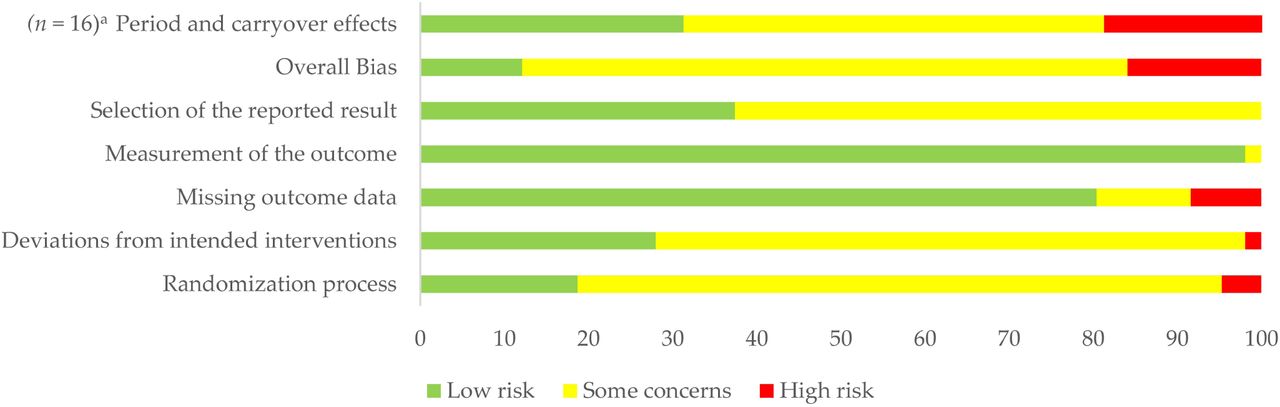
The overall risk of bias of eligible studies was acceptable, but trials of some patterns (i.e., fiber and DASH) had a relatively high risk of bias (Table 1). 15.9% of studies were at high risk of bias, while 12.1% were at low risk and the left were of some concerns (Figure 2). Notably, the risk of bias of crossover RCTs was significantly higher than parallel ones (Mann-Whitney U = 978.00, P0.05/2 = 0.006), mainly due to the period and carryover effects. Detailed risk of bias ratings of each domain is displayed in File S6.

Risk of bias of included studies. a The “period and carryover effects” domain was only for crossover RCTs (n = 16), and other domains were for all included studies (n = 107).
3.3. Main Outcomes
The number of nodes and comparisons varied among outcomes (Figure 3 and File S7). File S8 presented all league tables and cumulative ranking curves; File S9 showed forest plots with heterogeneity and inconsistency tests of all outcomes.

{kind=link}
{kind=link}
{kind=link}
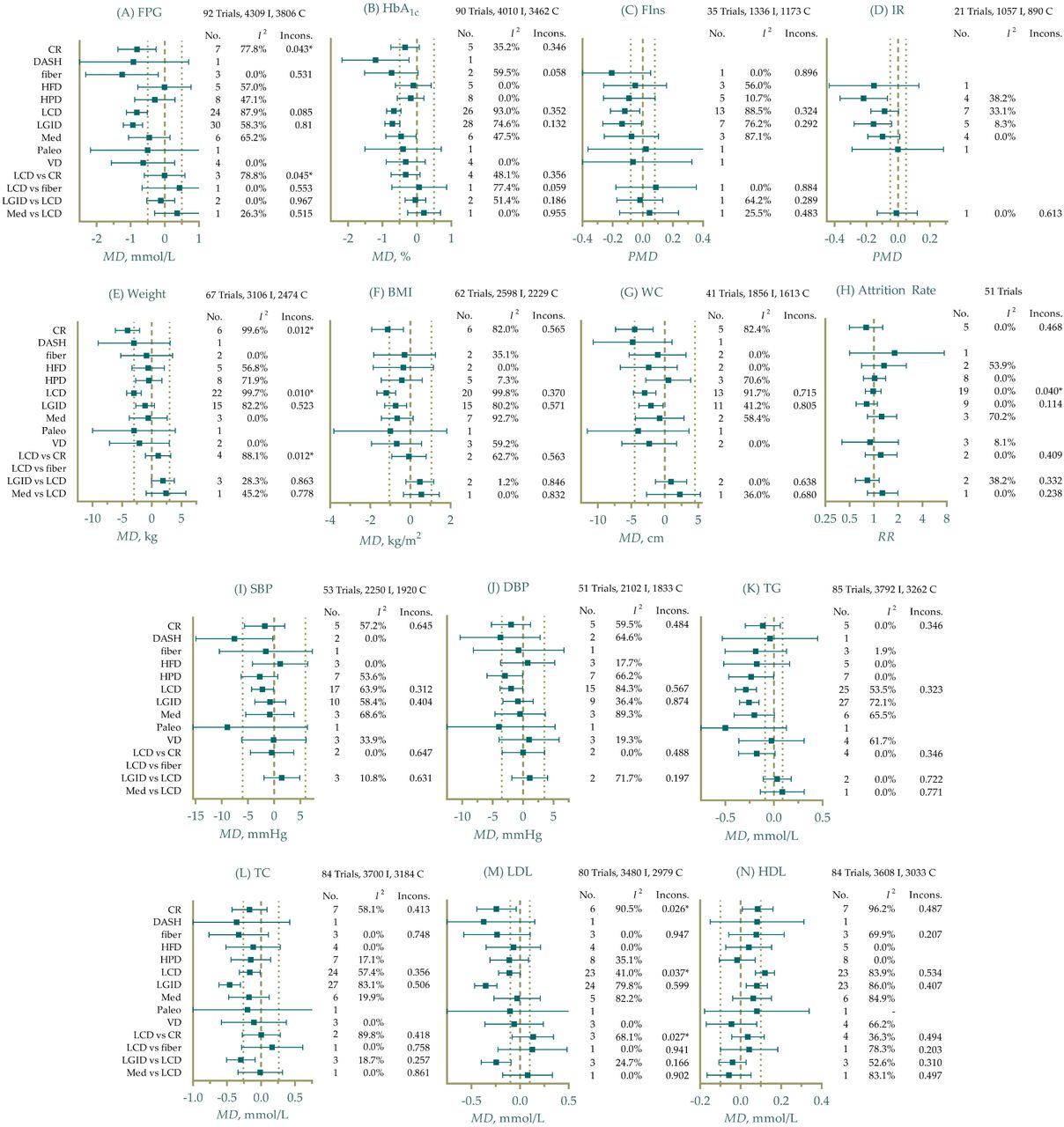
Efficacy of different eating patterns on glycemic control, anthropometrics, serum lipid profiles, and comparative attrition rate. I, intervention arm; C, control arm; No., Number of direct comparisons; Incons., P value of inconsistency test (node-splitting method); MD, mean difference; PMD, difference in percentage change from baseline; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; FIns, fasting insulin; IR, insulin resistance; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; TG, triacylglycerol; TC, total cholesterol; LDL, low-density lipoprotein cholesterol; HDL, high-density lipoprotein cholesterol. Thick dashed referred to the null value, and thin dashed referred to the MCID threshold. Unless otherwise specified using “vs”, the effect sizes were experimental patterns vs control. I2 values were for network heterogeneity, including both direct and indirect comparisons.
3.3.1 Glycemic Control
For glycemic control, high-fiber diet (fiber) was ranked as the best pattern for reducing FPG (MD -1.3 mmol/L, 95% CrI -2.3 to -0.22, SUCRA 82.7%), followed by LGID (-0.94 mmol/L, -1.2 to -0.65, SUCRA 74.6%) and LCD (-0.82 mmol/L, -1.1 to -0.51, SUCRA 65.1%) (Figure 3A). DASH (-1.2%, -2.2 to -0.23, SUCRA 90.5%), LGID (-0.71%, -0.93 to -0.49, SUCRA 76.2%), and high-fiber diets (-0.74%, -1.5 to 0.035, SUCRA 71.2%) had the highest probability of improving HbA1c compared with control groups, but high-fiber diets did not show statistical significance (Figure 3B). The effects on reducing FPG and HbA1c were comparable.
FIns and IR were presented as PMD due to the various units reported by studies and the nature of arm-based network meta-analysis that standardized mean difference was not applicable. Effects on improving insulin-related conditions were not stable and significant due to the limited sample size. High-fiber diets achieved a mean of 21% reduction of FIns (95% CrI 5.2% to 46%) with a probability of 79.4% to be the best pattern, followed by LGID (-14%, -27% to -0.98%, SUCRA 68.3%) (Figure 3C). IR was reported as homeostatic model assessment (HOMA)1-IR and HOMA2-IR from included studies, among which HPD showed the best beneficial effects on improving IR (-22%, -37% to -7.0%, SUCRA 86.3%) (Figure 3D).
3.3.2. Anthropometrics
CR was still one of the most effective diet patterns for weight loss (-4.1 kg, -6.1 to -2.0, SUCRA 86.8%) and WC (-4.5 cm, - 7.4 to -1.8, SUCRA 82.2%), and LCD was ranked as the second (-3.0 kg, -4.3 to -1.8, SUCRA 74.3%) for weight loss and the best (-1.2 kg/m2, -1.7 to -0.74, SUCRA 81.6%) for BMI reduction (Figure 3E-G). As for blood pressure, DASH was found to be the best pattern for lowering SBP (-7.6 mmHg, -15 to -0.29, SUCRA 87.9%) and the second for DBP (-3.7 mmHg, -10 to 2.8, SUCRA 73.7%), while HPD was the most effective for DBP (-3.0 mmHg, -5.9 to -0.068, SUCRA 74.6%) with slight advantage than DASH (Figure 3I-J).
3.3.3. Lipid Profiles
Figure 3K-N illustrated different interventions’ effects on lipid profiles comparing with control groups. LGID showed the most remarkable efficacy for lowering TC (-0.46 mmol/L, -0.62 to -0.30, SUCRA 87.5%) and LDL (-0.35 mmol/L, -0.47 to -0.24, SUCRA 86.6%), but were not of beneficial effects on HDL. Paleo was ranked as the best pattern for improving TG (-0.50 mmol/L, -1.1 to 0.13, SUCRA 83.4%), though the outcome was not statistically significant. LCD led to an average increase of 0.12 mmol/L (95% CrI 0.073 to 0.17, SUCRA 84.0%) for HDL compared to control, thus being the best intervention with a small effect size.
3.3.4. Attrition
Since a considerable number of studies did not report flowcharts of randomization, allocation and follow-up, we only included trials that reported a loss in at least one arm into synthesis. An attrition rate was calculated as: the attrition number divided by the product of participant number when allocation and the duration of intervention (in weeks). The meta-analysis denoted that there was no significant difference among all patterns (Figure 3H; File S8), which implied that participants’ tolerance for each diet might be similar.
3.4. Heterogeneity and Inconsistency Test
Generally, the included dietary patterns were of moderate to high heterogeneity (Figure 3, File S9, and File S10), making the results less confident. LCD vs. control, CR vs. control, LGID vs. control, LCD vs. CR, and LGID vs. LCD were of very high heterogeneity in either direct or network comparison, while Med vs. control and HPD vs. control were with moderate heterogeneity mainly in lipid profiles. Significant inconsistency was observed in LCD vs. CR comparison in FPG, and CR-LCD-control loop of weight and LDL using node-splitting methods. The evidence of CR, LCD and LGID showed severe incoherence and inconsistency and should be interpreted prudently.
3.5. Meta-regression
A random effect meta-regression model with one covariate and exchangeable coefficients was fitted for all included continuous outcomes. All coefficients and adjusted means were presented and summarized in File S11. Universally, the meta-regression denoted that the mean weight, BMI, and macronutrient intake significantly modified the efficacy of interventions of most outcomes. On the contrary, coefficients of the duration of intervention, study design, medication or insulin treatment, duration of disease, and sex ratio were not significant, implying that these factors may not contribute to the effectiveness. Another notable finding that coefficients of sample size and origin (from China or not) showed significance in FPG, weight, and lipid profiles indicated potential publication or selection biases.
3.6. Sensitivity Analysis
Weight, BMI, and TC performed well and showed robustness in the sensitivity analysis using the exclusion of each single study strategy. However, all other outcomes were not robust enough (File S12). The exclusion of Fang 2019 [68], Liu 2020 [98], Lousley 1984 [99], Tang 2021 [127], Wang 2009b [136], Wang 2015 [135], Chandalia 2000 [52], Durrer 2021 [62], Marco-Benedí 2020 [102], Wu 2020 [141] and Zahedi 2021 [146] significantly changed the SUCRA and the 95% CrI of effect size, mainly in comparisons of CR, LCD, and Med vs control, contributing to the severe heterogeneity. When testing for different models, i.e., fixed effect models or unrelated study effect models, Med, HPD, and VD showed narrower 95% CrIs and became statistically significant for more outcome variables (see File S12 for detailed information). The number of included studies for these patterns was small, resulting in a lower weight using a random effect model. The analysis did not observe sensitivity of relative effect priors, between-study heterogeneity priors, and correlation coefficients.
3.7. Publication Bias
Potential publication bias of HbA1c, weight and BMI existed (Egger’s test P = 0.002; < 0.001; and < 0.001, respectively). P values for all outcomes and comparison-adjusted funnel plots were listed in File S13.
3.8. Quality of Evidence and Drawing Conclusions
We identified the minimal clinically important differences (MCID) for each outcome according to the MCIDs reported by previous articles [14, 36-38] (see File S14, Figure 3, and Table 2). Subsequently, the authors reached a consensus on the thresholds of moderate and large beneficial/harmful effects to draw conclusions of evidence under a partially contextualized framework provided by the GRADE workgroup (Table 2). Of all 123 pieces of evidence that compared intervention and control groups, only 49 were rated as moderate quality, and there was no evidence of high quality. At the clinical level, all of the patterns were at least not significantly worse than control diets for each outcome, but most did not show moderate to large beneficial effects. Additionally, more trivial effects were for anthropometrics, while FIns, IR, TG, and LDL were with larger beneficial effects. Because we only included five PreD-related RCTs, all the quality of evidence should be downgraded one level when applying to PreD due to the indirectness.
Summary of findings
4. Discussion
In this study, we evaluated the comparative efficacy of eleven eating patterns (ten experimental and one control). We identified the rankings of each pattern for glycemic control, anthropometrics, and lipid profiles. The restriction of energy intake, carbohydrates, and glycemic index (GI), as well as the intake of dietary fiber, were the most effective approaches to improve glycemic control, weight and lipid profiles of patients with T2DM/PreD, with solid and abundant evidence bases. However, the heterogeneity and the sensitivity implied the need of further studies. On the other hand, DASH, Paleolithic diets, and HPD were of satisfactory efficacy in limited outcomes and worth investigation. The meta-analysis also denoted that Mediterranean diets and VD did not act well in nearly all outcomes, mainly due to the imprecision. High-fat diets without carbohydrate restriction did not show any beneficial effects compared to control diets. Severe heterogeneity and sensitivity should be concerned when interpreting the results.
4.1. Energy and Macronutrients
A previous evidence basis has corroborated the efficacy of CR in weight loss, BMI and WC in patients with obesity, metabolic diseases or in healthy individuals [150, 151]. Minor beneficial effects on weight loss and reducing BMI with low and moderate quality of evidence were observed. Meanwhile, CR did not lead to greater improvement of glycemic control, blood pressure, TG, and TC compared to standard diets. Trivial effects on glycemic and lipid outcomes may result from weight loss but not the caloric restriction, since several studies have suggested that a weight loss be of tight relevance to them [152, 153]. The median TEI of the included CR arms was 1594 kcal/d (interquartile range, IQR 1572 to 1609), with a 150-to-400-kcal negative difference compared to standard diets, which was significantly lower than the prescribed (-500 kcal/d). However, the deviance did not lead to the failure of the intervention. A probable explanation was that participants might focus more on their dietary intake and weight loss to improve their diets once the intention and the belief to improve was built via consultation or menus: not only in energy intake but also in other aspects like food groups, dietary fiber, etc. The phenomena were also observed in LCD and LGID.
Carbohydrate restriction acted well in weight, HbA1c, TG, and HDL, where improving HDL was the unique advantage of LCD. Nevertheless, other types of serum lipids, i.e., TC and LDL were not improved, though the meta-regression suggested that carbohydrate intake be negatively correlated to the effectiveness of LGID and CR in modulating lipids. Similar to the CR arms, the median carbohydrate intake of the included LCD arms was 30.5% (IQR 20% to 40%), which indicated that nearly a quarter of included trials did not meet the low-carbohydrate criteria as prescribed. Nevertheless, the effect size was similar to previous systematic reviews [14], and the strict following of the instruction as well as a more intensive intervention did not enhance the effects but may even lead to a decrease, denoted by the meta-regression (File S11). Participants’ motivation and intention may be an explanation: prepackaged or prepared frozen food may not be of participants’ favors, so they would not adhere perfectly to the intervention, and added food to their diets.
Participants usually decreased their food intake in LCD intervention because of the increased satiety, which led to a spontaneous caloric restriction [154, 155]. Therefore, how to distinguish the effects of carbohydrate and caloric restriction in an LCD trial was always the focus, usually by introducing isocaloric arms. However, we did not find a significant between-group difference of actual energy intake in the included LCD trials, despite the limited number of trials that reported actual intake. The meta-regression also suggested that additional caloric restriction or the TEI did not significantly modify the effects of LCD in lipids, implying that carbohydrates acted as a different role in the treatment. Lastly, the combination of carbohydrate and caloric restriction may have more beneficial effects though it brought more compliance problems: in the trial Durrer 2021 [62], severe restrictions (984 kcal/d and 27%TEI carbohydrate) made all of the outcomes improve substantially.
The increased intake of protein without carbohydrate restriction (HPD) effectively improved IR, blood pressure and TG. Furthermore, protein intake was positively correlated to FPG, HbA1c, weight, and BMI improvement in meta-regression. Compared to the previous review [156], the effectiveness of HPD on FPG, HbA1c and other lipids was not observed, mainly due to the different inclusion criteria: only HPD with protein intake of more than 30% TEI and without carbohydrate restriction was included. This implied the different efficacy of protein and carbohydrate. As for HFD, no beneficial effect was detected, and fat intake negatively modified the lipid improvement. Of all five included HFD trials, three [45, 49, 122] emphasized a high-monounsaturated-fat diet, while the other two did not specify the type of fat. Despite the numerical impact of specific lipids, it remained to be evaluated whether the increased intake of monounsaturated fat or other types of fat improved or negatively affected the overall lipoprotein profile [157]. Unfortunately, the included trials were of limited sample size and did not provide sufficient data to draw a thorough interpretation.
4.2. Glycemic Index and Dietary Fiber
LGID and high-fiber diets emphasized more on the quality rather than the quantity of carbohydrates, compared to LCD. Effects of LGID and high-fiber diets were similar: both showed more excellent effects on FPG, HbA1c, FIns, TC, and LDL than most other patterns, but did not significantly improve weight-related outcomes, consistent with other studies [158, 159]. Dietary GI and fiber of specific single food were not well associated [160]. However, the emphasis on lowering GI may encourage participants to increase fiber intake, because the usually recommended natural food groups in nutrition consultations can be both low in GI and high in fiber, e.g., whole grains and nuts.
A recent meta-analysis published in the Lancet has also denoted that dietary fiber and low-GI food were associated with a lower risk of T2DM incidence, where fiber may be a stronger protector [161]. Dietary fiber also had other benefits, e.g., lower all-cause mortality and coronary heart disease incidence [161]. Rather than a severe long-term restriction of the quantity of carbohydrates which leads to higher all-cause mortality [162], LGID and increased fiber intake can be better and sustainable approaches for the management of T2DM patients without obesity/overweight, especially with the circumstance that most people lacked fiber intake [163].
4.3. Mediterranean Diets
Even if previous cohort studies and RCTs have demonstrated the efficacy of Med in T2DM management [164], our study failed to detect a significant improvement driven by Med. Except for HbA1c, IR and TG, all other outcomes were of great imprecision and trivial effects. The effect size was also more trivial than other meta-analyses [15, 165]. Nevertheless, sensitivity analysis using fixed effects models and unrelated study effects models suggested that Med significantly improved FIns, weight, BMI, blood pressure, and TC. Small sample size compared to other interventions could be the reason when using random effects models; different calculation of effect size, i.e., MD of change from baseline or of endpoint may explain the numerical differences.
Moreover, heterogeneity was detected for almost all outcomes of Med vs control comparisons. Researchers have pointed out the variance and bias of the definition of Med in different trials [166], which can cause great between-study heterogeneity and led to the low quality of evidence. Though several scales have been developed to measure the adherence to Med (e.g., MedDiet Score) [167], few trials employed it, thus not able to assess the impact of adherence to the effects of Med.
4.4. DASH and Paleolithic Diets
Evidence of the efficacy of DASH and Paleo was limited and of low quality due to the sample size. As one of the recommended healthy patterns for the general population by Dietary Guidelines for Americans (DGA 2020-2025) [168], many studies have addressed its benefit in blood pressure and glycemic control [169, 170]. However, RCTs focusing on the effects of DASH in T2DM/PreD patients were rare. Only two RCTs on DASH were included, where one [40] was of high risk of bias; one trial for Paleo was eligible. This study also outlined the beneficial effects of DASH on blood pressure, TC, LDL, and HbA1c, where DASH was ranked as the most effective intervention for HbA1c with a high probability (90.5%), suggesting the potential advantage for T2DM remission. For Paleo, Jönsson T (the author of the included trial [88]) and his colleagues also quantified the improvement of leptin and introduced a scale (Paleolithic Diet Fraction) to measure the compliance, based on their trial [88, 171], which provided a basis for further studying.
Considering the lack of RCTs, a systematic review containing all eligible controlled trials or other observational studies may be better to address the efficacy of DASH and Paleo, and the effects of these patterns in the management of T2DM/PreD still need more demonstration of high quality.
4.5. Vegan, Vegetarian, or Plant-based Diets
VD did not show any significant beneficial effects in the meta-analysis. Nevertheless, the mean differences of VD were similar to the previous studies [37], thus did not affect the conclusion of evidence but lowered the ratings of quality of evidence. While using fixed effects models, the effectiveness of VD on BMI, WC, and HbA1c was detected. However, moderate heterogeneity made it unreasonable to employ fixed effects models, though the small number of participants led to wider 95% CrIs when using random effect models.
Notably, the carbohydrate intake in included VD trials was relatively high (mean 65.8%TEI). The sensitivity analysis also showed a slight improvement of SUCRA in TG after excluding Lee 2016 [92], which contained about 72%TEI of carbohydrate in the intervention arm. Therefore, researchers should consider a lower carbohydrate intake when conducting VD, and the effects would promise to be more significant.
4.7. Strengths and Limitations
We included more than 8000 participants and the most frequently used outcomes in the meta-analysis. Meanwhile, the summary of findings was clearly drawn following the partially contextualized framework. These could be advantages of our study. However, this study had several limitations. First, the severe heterogeneity and sensitivity lowered the quality of evidence. Second, the sample size of VD, DASH, and Paleo was limited, leading to the imprecision. Third, only five PreD trials were included, raising the indirectness when applying the evidence to the PreD population. Moreover, there was not an adequate method to compare the longitudinal dataset of different patterns, though the data of different timepoints have been extracted.
5. Conclusions
This systematic review provided an insight into the efficacy of different eating patterns in the management of T2DM and PreD with moderate-to-low quality evidence. Clinicians and dietitians can take the evidence into consideration when providing nutrition consultations and conducting medical nutrition therapy. However, the quality and the sensitivity of the evidence can be a barrier to clinical practice. More powerful and well-designed RCTs, as well as real-world evidence studies, are needed to draw more precise conclusions, especially for DASH and Paleolithic diets.
Data Availability
All data produced in the present work are contained in the manuscript and the supplementary materials.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, File S1: Full search strategy; File S2: Data extraction template; File S3: Correlation coefficients for estimation; File S4: Reason for exclusion; File S5: Fundings and conflicts of interest of included studies; File S6: Risk of bias assessment; File S7: Network plots; File S8: League tables and cumulative ranking curves; File S9: Forest plots; File S10: Heterogeneity and inconsistency test; File S11: Meta-regression; File S12: Sensitivity analysis; File S13: Publication bias; File S14: Minimal clinically important difference and thresholds for effects.
Author Contributions
Conceptualization, B.-T.Z. and J.-W.D.; Methodology, B.-T.Z.; Software, B.-T.Z.; Validation, H.-Q.P., F.-D.L. and Z.- Y.Y.; Formal Analysis, B.-T.Z.; Investigation, B.-T.Z. and H.-Q.P.; Resources, Y.L.; Data Curation, B.-T.Z. and Z.-Y.Y.; Writing – Original Draft Preparation, B.-T.Z. and H.-Q.P.; Writing – Review & Editing, Y.L. and F.-D.L.; Visualization, B.-T.Z.; Supervision, J.-W.D. and Y.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in supplementary materials.
Conflicts of Interest
The authors declare no conflict of interest.
Acknowledgments
We acknowledge Professor Lawrence J. Cheskin from George Mason University for his kindly replying our email about the data availability of his registered trial.
Appendix A
The dietary patterns included in this article were defined as:
Caloric restriction (CR): a more than 500-kcal negative energy balance.
DASH: a dietary pattern that emphasizes dietary fiber, protein, fruits rich in potassium/magnesium/calcium, vegetables, beans, legumes, whole grains, and low-fat dairy food; avoids sugar and saturated fat intake [172].
High-fiber diet: a total dietary fiber intake of more than 35 to 40 g/d, or 20 to 25 g/1000 kcal.
High-fat diet (HFD): Fat intake of more than 30% TEI with more than 40% TEI carbohydrate intake.
High-protein diet (HPD): 30% TEI or more protein intake with more than 40% TEI carbohydrate intake.
Low-carbohydrate diet (LCD): less than 40% TEI carbohydrate intake.
Low-glycemic-index diet (LGID): a reduced average glycemic index of all dietary intake, less than 50 to 65.
Mediterranean diet: a dietary pattern rich in olive oil, vegetables, cereals, legumes, nuts, seafood/fish, dairy food, and moderate red wine [166].
Paleolithic diet: a dietary pattern that emphasizes the intake of “lean meat, fish, fruits, root vegetables, eggs and nuts” [173], and avoids processed food.
Vegetarian, vegan or plant-based diet: a series of dietary patterns where most of the macronutrients were from plants and not from meat, with or without eggs, milk or other animal-derived food.
The macronutrients and food group intake can be as prescribed or as actual.
Footnotes
zengbentuoxmu{at}outlook.com (B.-T.Z.); yezhenyu1999{at}gmail.com (Z.-Y.Y.)
phq19991011{at}126.com
18350278581{at}163.com
References
- [1].↵
- [2].↵
- [3].↵
- [4].↵
- [5].↵
- [6].↵
- [7].↵
- [8].↵
- [9].↵
- [10].
- [11].
- [12].
- [13].
- [14].↵
- [15].↵
- [16].↵
- [17].↵
- [18].↵
- [19].↵
- [20].↵
- [21].↵
- [22].↵
- [23].↵
- [24].↵
- [25].↵
- [26].↵
- [27].↵
- [28].↵
- [29].↵
- [30].↵
- [31].↵
- [32].↵
- [33].↵
- [34].↵
- [35].↵
- [36].↵
- [37].↵
- [38].↵
- [39].↵
- [40].↵
- [41].
- [42].
- [43].
- [44].
- [45].↵
- [46].
- [47].
- [48].
- [49].↵
- [50].
- [51].
- [52].↵
- [53].
- [54].
- [55].
- [56].
- [57].
- [58].
- [59].
- [60].
- [61].
- [62].↵
- [63].
- [64].
- [65].
- [66].
- [67].
- [68].↵
- [69].
- [70].
- [71].
- [72].
- [73].
- [74].
- [75].
- [76].
- [77].
- [78].
- [79].
- [80].
- [81].
- [82].
- [83].
- [84].
- [85].
- [86].
- [87].
- [88].↵
- [89].
- [90].
- [91].
- [92].↵
- [93].
- [94].
- [95].
- [96].
- [97].
- [98].↵
- [99].↵
- [100].
- [101].
- [102].↵
- [103].
- [104].
- [105].
- [106].
- [107].
- [108].
- [109].
- [110].
- [111].
- [112].
- [113].
- [114].
- [115].
- [116].
- [117].
- [118].
- [119].
- [120].
- [121].
- [122].↵
- [123].
- [124].
- [125].
- [126].
- [127].↵
- [128].
- [129].
- [130].
- [131].
- [132].
- [133].
- [134].
- [135].↵
- [136].↵
- [137].
- [138].
- [139].
- [140].
- [141].↵
- [142].
- [143].
- [144].
- [145].
- [146].↵
- [147].
- [148].
- [149].↵
- [150].↵
- [151].↵
- [152].↵
- [153].↵
- [154].↵
- [155].↵
- [156].↵
- [157].↵
- [158].↵
- [159].↵
- [160].↵
- [161].↵
- [162].↵
- [163].↵
- [164].↵
- [165].↵
- [166].↵
- [167].↵
- [168].↵
- [169].↵
- [170].↵
- [171].↵
- [172].↵
- [173].↵



