
Abstract
Background Chronic Overlapping Pain Conditions (COPCs) are a subset of chronic pain conditions commonly comorbid with one another and more prevalent in women and assigned female at birth (AFAB) individuals. Pain experience in these conditions may better fit with a new mechanistic pain descriptor, nociplastic pain, and nociplastic type pain may represent a shared underlying factor among COPCs
Methods We applied GenomicSEM common-factor genome wide association study (GWAS) and multivariate transcriptome-wide association (TWAS) analyses to existing GWAS output for six COPCs in order to find genetic variation associated with nociplastic type pain, followed by genetic correlation (linkage-disequilibrium score regression), gene-set and tissue enrichment analyses.
Results We found 24 independent single nucleotide polymorphisms (SNPs), and 127 unique genes significantly associated with nociplastic type pain, and showed nociplastic type pain to be a polygenic trait with significant SNP-heritability. We found significant genetic overlap between multisite chronic pain and nociplastic type pain, and to a smaller extent with rheumatoid arthritis. Tissue enrichment analyses highlighted cardiac and thyroid tissue, and gene set enrichment analyses emphasized potential shared mechanisms in cognitive, personality, and metabolic traits and nociplastic type pain along with distinct pathology in migraine and headache.
Conclusions We use a well-powered network approach to investigating nociplastic type pain using existing COPC GWAS output, and show nociplastic type pain to be a complex, heritable trait, in addition to contributing to understanding of potential mechanisms in development of nociplastic pain.
Introduction
Chronic pain can be defined as pain that persists 3+ months (1) and is a main symptom of many conditions as well as being associated with injury and surgery. Chronic pain can also be studied as a complex disease trait in line with recent international association for the study of pain (IASP) redefinitions of pain and definition of ‘chronic primary pain’ codes for the ICD-11 (2–4), and several recent large genome-wide association studies (GWAS) have uncovered genetic variation associated with such chronic pain traits (5–7). More than 1 in 5 US adults experience chronic pain (8), and chronic pain is associated with high socioeconomic and quality of life burden (1,9), and despite genetic studies into chronic pain as a disease trait, and on conditions where chronic pain is a prominent symptom, mechanisms of development of chronic pain are not fully understood.
Neuropathic and nociceptive pain (10) are used to categorize pain and chronic pain according to suspected or confirmed underlying mechanism(s). Neuropathic pain is defined as caused by lesions or disease in the somatosensory nervous system, and nociceptive pain, designed to directly contrast neuropathic pain, is defined as pain arising from actual or threatened damage to non-neural tissue (in the context of a normally functioning somatosensory nervous system). However, pain experienced in the context of many different chronic pain conditions may not fit with these two descriptors – Chronic Overlapping Pain Conditions (COPCs) (11–13) may represent a subset of chronic pain conditions where pain experiences very often diverge from nociceptive/ neuropathic or a mixed nociceptive/ neuropathic pain state. COPCs are a subset of chronic pain conditions commonly comorbid with one another and more prevalent in people assigned female at birth (AFAB). The United States congress and the National Institutes of Health (NIH) listed ten conditions as COPCs; myalgic encephalitis/ chronic fatigue syndrome (ME/CFS), vulvodynia, temporomandibular disorders, irritable bowel syndrome (IBS), interstitial cystitis/ painful bladder syndrome, fibromyalgia, endometriosis, chronic tension-type headache, chronic migraine headache, and chronic low-back pain. In these conditions, there may not be actual or threatened tissue damage or lesion/ disease at the somatosensory nervous system (e.g., fibromyalgia), or if features of nociceptive/ neuropathic pain are present they do not fully capture the pain experience (e.g., chronic low back pain). A proposed third mechanistic pain descriptor, ‘nociplastic pain’, added to IASP terminology (10) in 2017 may better capture features of pain in COPCs (11).
Nociplastic pain is defined as pain arising from altered nociception in the absence of clear lesion/ disease of the somatosensory nervous system and/or absence of actual or threatened tissue damage causing activation of peripheral nociceptors. Pain in COPCs, where nociplastic pain could be the underlying mechanism (or main underlying mechanism if a mixed pain state is suspected), may fit better with this description as many COPCs are not associated with neural/ non-neural tissue damage (e.g., fibromyalgia), or if disease and tissue damage is present pain is often non-proportional to tissue damage and can be diffuse throughout the body beyond diseased tissue sites (e.g., endometriosis, chronic low back pain). Nociplastic pain is also associated, compared to nociceptive or neuropathic pain, with greater risk of CNS-related symptoms such as fatigue, changes in cognition and memory, depression, anxiety, and sleep issues as also commonly seen in COPCs (12).
These features of COPCs, combined with the fact they are commonly comorbid with one another, may suggest that nociplastic type pain is an underlying shared factor across COPCs. Even in COPCs where a mixed pain state with nociceptive pain (i.e., where tissue damage may be present) such as endometriosis, studies have shown that nociplastic pain contributes significantly to pain experience, and is associated with severity of pain independent of surgical procedures, amount of endometriosis, BMI, and age (14). Previous studies also suggest COPCs could be viewed as a single “lifelong” disease that “manifests in different bodily regions over time” (15). There are epidemiological studies of pelvic pain conditions (e.g., MAPP (16,17)), but there are no GWAS of vulvodynia, chronic pelvic pain, or bladder pain syndrome/ IC. In addition, there are to date no sufficiently large studies with both genotyping and questionnaire data designed specifically to ascertain nociplastic pain (such as the Central Sensitization Inventory (18) or Nociplastic-Based Fibromyalgia Features tool (19)). However, large-scale GWAS for several other COPCs are available, and can be studied as a network to uncover genetic variation associated with nociplastic-type pain as an underlying factor in all COPCs.
Chronic pain conditions can be highly stigmatized (20–24) – this is likely even more common in COPCs due to a lack of or disproportionate-to-pain-level presence of tissue or nerve damage (25–27), and higher prevalence of COPCs in women and AFAB people (20,28). Understanding mechanisms of chronic pain that are not due to, or cannot be fully explained by, nervous system damage or dysfunction or tissue damage (i.e., nociplastic pain) will contribute to legitimizing the pain experience in COPCs. In addition, finding genetic variation associated with nociplastic pain could inform new treatment approaches in COPCs, conditions where many existing pharmaceutical and surgical treatments can be less effective (29) or even actively worsen pain (30) compared to use in nociceptive/ neuropathic pain.
Methods
GWAS summary statistics
GWAS summary statistics for 6 chronic overlapping pain condition (COPC) traits were obtained through publicly available downloads, requests made directly to study authors, or through data request to FinnGenn (release R9, May 2023). Traits, sample sizes, and sources are summarized in Table X. We opted not to include migraine or ME/CFS summary statistics. With ME/CFS (31) this is due to sample size being too small for successful completion of the multivariable LDSC step of GenomicSEM common-factor GWAS analysis (Ncase = 427, Ncontrol = 972). For migraine, a significant proportion of the ‘broad headache’ GWAS case participants are likely migraineurs and/or have both tension-type headache and migraine, therefore including the broad headache GWAS but not migraine GWAS allows for capturing a fuller spectrum of headache and migraine-associated genetic variation, without over-representation of migraine.
Common factor GWAS
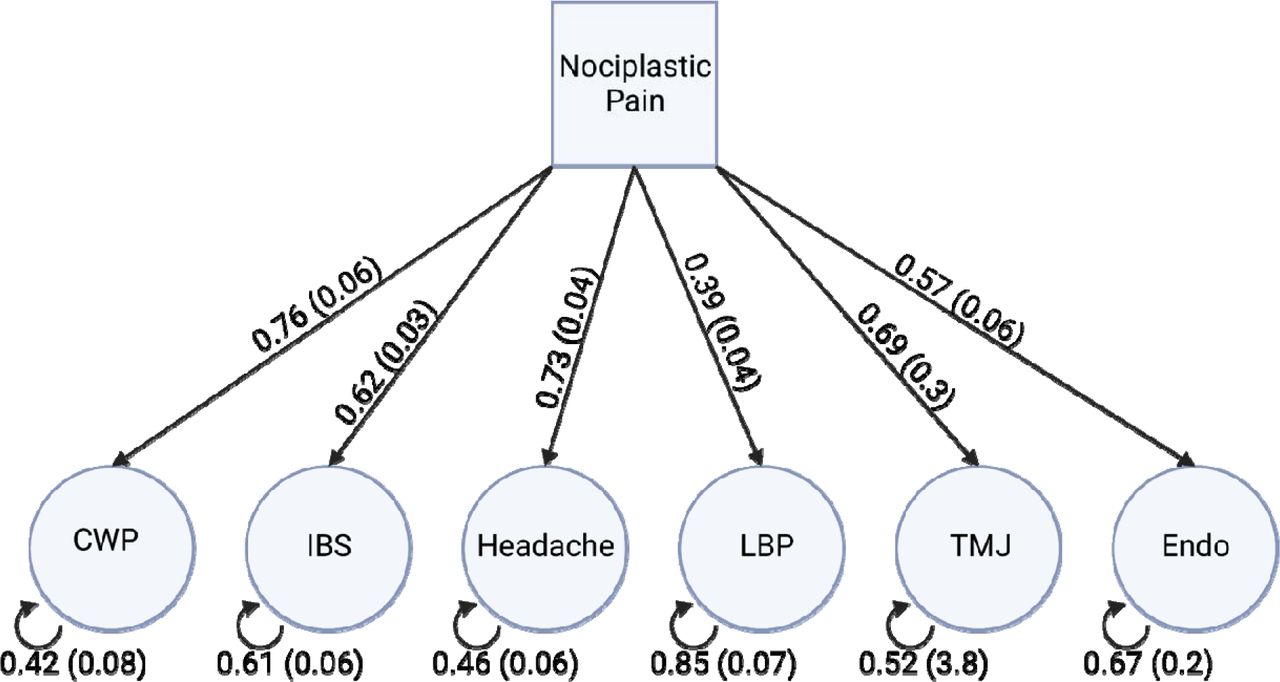
GenomicSEM was used to carry out a common-factor GWAS. First, we prepared (munged) GWAS summary statistics using munge function included in GenomicSEM. Sum of effective sample sizes was calculated for traits LBP and IBS, as these represented GWAS-meta-analyses of case-control phenotypes (see also https://github.com/GenomicSEM/GenomicSEM/wiki/2.1-Calculating-Sum-of-Effective-Sample-Size-and-Preparing-GWAS-Summary-Statistics). Briefly, variants with info values <= 0.9, minor allele frequency (MAF) <= 0.01, that were not single nucleotide polymorphisms (SNPs), with missing values, that were strand ambiguous, those with duplicated rsIDs, those without a match in the HapMap 3 SNP file used for quality control, and those with mismatched allele labels compared to the HapMap 3 SNP file were removed. Next, multivariable linkage disequilibrium (LD)-score regression was carried out to produce matrices used in the common-factor GWAS step. GenomicSEM ‘sumstats’ function was used for a final preparation step, jointly processing the GWAS summary statistics files for each of the 6 traits included in the analysis. This function merges across all summary statistics using listwise deletion, performs quality control (including backing out logistic betas, checking for allele mismatches, missing data, and duplicate variants), and merges with the reference SNP file. Output from multivariable LD-score regression, and from GenomicSEM ‘sumstats’, is taken forward to common factor GWAS using GenomicSEM ‘commonFactorGWAS’ function. Our chosen common-factor model, where the single latent factor represents ‘nociplastic type pain’, is shown in Figure 1.

First, we fitted the common-factor GWAS model without SNP effects and noted loadings of each trait onto the singular factor (Figure 1). These were significant (Table 2, p < 0.05) and model fitting was successful, so we proceeded to fitting the model including SNP effects with ‘smooth_check=T’. We note that TMJ variance SE is very large (Figure 1, SE = 3.8), likely due to the small case number in the TMJ GWAS, but factor loading was significant (Table 2, 0.69, p < 0.05) so we elected to include TMJ in this model. Output produced from the above model is equivalent to GWAS summary statistics (magnitude of association between each SNP and a trait of interest, nociplastic-type pain) for the latent factor onto which the 6 traits load – which we describe as nociplastic-type pain. Next, we calculate an estimated sample size for the ‘GWAS’ of nociplastic-type pain according to instruction provided on the GenomicSEM github, first reserving SNP results for SNPs with MAF <= 0.4 and => 0.1, and then calculating  according to the formula for each SNP:
according to the formula for each SNP:

Taking the mean this set of values then gives  . For nociplastic-type pain
. For nociplastic-type pain  =578,561.3 (where this sample size is necessary in calculations e.g., LD-score regression analyses for genetic correlation, we use the value 578,561).
=578,561.3 (where this sample size is necessary in calculations e.g., LD-score regression analyses for genetic correlation, we use the value 578,561).
Defining significant, independent SNPs
Common-factor GWAS output (nociplastic type pain summary statistics) was then taken forward and analyzed within FUMA (Functional Mapping and Annotation of Genome-Wide Association Studies) (42), a web-based suite of tools for downstream GWAS analyses.
Genome-wide significant, independent SNPs were defined using FUMA as SNPs associated with nociplastic pain factor (p < 5×10^-8) and independent from one another (r2 < 0.6).
LD-score Regression
We used ‘ldsc’ (43,44) to estimate SNP-heritability of nociplastic-type pain, and to estimate genetic correlation between nociplastic-type pain and MCP, and between nociplastic-type pain and rheumatoid arthritis, a chronic pain condition not usually considered a COPC.
Multisite chronic pain vs nociplastic-type pain
We obtained summary statistics for GWAS of multisite chronic pain (MCP) (5), a general chronic pain phenotype previously found to be heritable, polygenic, and significantly associated with gene expression changes in the brain through download from University of Glasgow Enlighten (research data repository). MCP summary statistics were munged as previously described, using ‘ldsc’ package, as was common factor GWAS output for nociplastic-type pain. We then carried out LD-score regression, estimating genetic correlation between MCP and nociplastic-type pain.
Rheumatoid arthritis vs nociplastic-type pain
We obtained rheumatoid arthritis GWAS summary statistics from a recent large GWAS (N = 311, 292) (45) from GWAS Catalog (46). As previously described and again using ‘ldsc’, we calculated genetic correlation between nociplastic type pain and rheumatoid arthritis.
Multivariate Transcriptome-Wide Association Study
An extension of GenomicSEM common-factor GWAS is multivariate (common-factor) TWAS. Here, FUSION TWAS (47) output for each of the 6 COPCs serves as input (as GWAS summary statistics did for common-factor GWAS in GenomicSEM common-factor GWAS). We performed TWAS in each of the 6 COPC traits using GWAS summary statistics and the FUSION package and scripts, and using pre-computed predictive models for all 49 GTEx (48) v8 tissues available at http://gusevlab.org/projects/fusion/#download-pre-computed-predictive-models. We used models including genes with significant heritability and with weights calculated using all genetic ancestries, as recommended for typical analyses and to increase sensitivity. FUSION output (TWAS summary statistics for each of the 6 COPCs) was prepared using the GenomicSEM ‘read_fusion’ function, and then taken forward with multivariable LDSC output from previous common-factor GWAS analysis to perform common-factor TWAS.
Significant gene-tissue association findings were defined at the tissue-wide and experiment-wide level, through Bonferroni multiple testing correction across all tests within a tissue and across all genes tested across all tissues respectively.
Specific and Non-Specific Genes
As part of multivariate GWAS and TWAS analyses, a Q (heterogeneity) value is calculated per SNP-trait association (or per gene-tissue-trait association), indicating degree of heterogeneity (i.e., the proportion of gene expression or SNP association effect that is mediated through pathways other than the shared common factor). Specific (to nociplastic type pain) genes were identified through subsetting multivariate TWAS output to include genes in significant (tissue-wide) gene-tissue associations and with non-significant Q p values (i.e., non-significant heterogeneity). Non-specific genes were also identified as above but with significant Q p values. Q p values were multiple test corrected using Bonferroni testing within-tissue. (Qp adj = Qp/N tests in that tissue).
Tissue enrichment analyses
We carried out binomial tests of enrichment to investigate whether certain tissues showed a higher proportion of tissue-wide significant (P bonf < 0.05) associations results than expected by chance, and whether certain tissues showed higher proportion of nominally significant (P < 0.05) associations than expected by chance.
Gene-set enrichment analyses
Gene-set enrichment analyses on all tissue wide significant genes, on tissue wide significant and specific genes (Q p adj > 0.05), and on tissue wide significant non-specific genes (Q p adj < 0.05) was carried out using FUMA, with all genes tested in multivariate TWAS and with recognized Ensembl gene ID as background (N = 26455 genes).
Results
Common-factor GWAS
We fitted a common factor GWAS model (including individual SNP effects), including data for six COPC traits (CWP, LBP, endometriosis, TMJ, IBS, and broad headache). This model estimates the size of association between SNPs and a latent common factor onto which the six traits load (nociplastic type pain), producing results effectively equivalent to a standard GWAS of this unmeasured latent factor. We found a total of 663 SNPs across fifteen GWAS genomic risk loci significantly associated with nociplastic-type pain (p < 5 × 10^-8), consisting of 24 independent SNPs. The majority of these SNPs (18/24) have not been previously associated with pain-related traits (Supplementary Table 1).

Heritability and Genetic Correlation
Nociplastic-type pain was found to be significantly heritable (liability scale SNP-h2 = 0.03, SE = 0.0014), and was significantly genetically correlated with MCP (rg = 0.92, SE= 0.04) and to a lesser degree with rheumatoid arthritis (rg = 0.18, SE = 0.04).
Multivariate TWAS
We found 819 tissue-wide significant gene-tissue associations consisting of 127 unique genes, across all 49 tested GTEx tissues. As part of multivariate GWAS and TWAS analyses with GenomicSEM, a Q (heterogeneity) value is calculated per association. This value indicates degree of heterogeneity (i.e., the proportion of gene expression or SNP association effect that is mediated through pathways other than the shared common factor, across the traits included in the model that load onto the common factor). Specific genes were identified through subsetting multivariate TWAS output to include genes in significant (tissue-wide) gene-tissue associations and with non-significant Q p values (i.e., non-significant heterogeneity). Non-specific genes were also identified as above but with significant Q p values. Q p values were multiple test corrected using Bonferroni testing within-tissue. (Qp adj = Qp/N tests in that tissue).
450 of the 819 tissue-wide significant gene-tissue associations showed significant heterogeneity (Q p adj < 0.05), and the remaining 369 did not (Q p adj > 0.05). Twenty-eight unique genes showed significant heterogeneity across all tested tissues (Q p adj < 0.05), and 94 showed non-significant heterogeneity (Q p adj > 0.05). Five genes showed both significant and non-significant heterogeneity depending on tissue, and were excluded from gene-set enrichment tests of specific/ heterogeneous genes.
Tissue enrichment
We found that 9 of the 49 tested tissues showed a different proportion of tissue-wide significant gene-tissue TWAS findings than expected by chance. Cultured fibroblasts, atrial appendage of the heart, tibial nerve, and thyroid were enriched for significant associations, whereas amygdala, substantia nigra, EBV-transformed lymphocytes, terminal ileum of the small intestine and vagina showed significantly fewer significant associations than expected. At the nominal significance level (unadjusted P < 0.05), two tissues showed a different proportion of associations than expected by chance – whole blood and skeletal muscle were enriched for significant (unadjusted P < 0.05) associations.
Gene-set enrichment
To explore potential mechanisms in nociplastic pain and shared with nociplastic type pain and other complex traits of interest, we performed three sets of gene-set enrichment tests using FUMA. First we used all unique tissue-wide significant gene findings from multivariate TWAS, then a subset of those findings that showed significant heterogeneity (non-specific genes) and finally a subset with non-significant heterogeneity (specific genes).
Tissue-wide significant genes
Of 127 unique genes, 120 had a recognized ensemble gene ID within FUMA and were included in analyses. Eight positional gene sets were enriched (p adj < 0.05) for nociplastic-type-pain associated genes; chr17q21, chr3p21, chr9q33, chr16q22, chr12q13, chr2q34, chr4q33, and chr1q21. KEGG pathway gene set nitrogen metabolism was also enriched for nociplastic pain genes, as was chemical and genetic perturbation gene set ‘SU_LIVER’ (genes specifically upregulated in the liver). A total of 44 GWAS Catalog traits including cognitive function, extremely high intelligence, sleep duration, and headache were enriched for nociplastic-type pain genes (Supplementary Table 2, Figure 3A). Additional gene sets enriched for nociplastic pain genes including microRNA target sets, transcription factor target sets, computational gene sets and cancer gene modules can be found in Supplementary Table 3.

Specific genes
90 of 94 tissue-wide significant genes without significant heterogeneity across all tissues where a significant association was found, and with an ensembl gene ID recognized within FUMA were included in this analysis. We found seven positional gene sets to be enriched for specific nociplastic pain genes, including chr3p21, chr9q33, chr16q22, chr2q34, chr4q33, chr12q13, and chr1q21. Chemical and genetic perturbation gene set ‘SU_LIVER’ was enriched for specific nociplastic pain genes, as was nitrogen metabolism, and the hallmark gene set fatty acid metabolism. Additional gene sets enriched for specific nociplastic pain genes are listed at Supplementary Table 4. We found 28 GWAS Catalog traits enriched for specific nociplastic pain genes (Supplementary Table 5, Figure 3B), including extremely high intelligence, sleep duration, regular attendance at a religious group, and cognitive function.
Non-specific genes
25 of 28 tissue-wide significant genes with significant heterogeneity across all tissues where a significant association was found, and with an ensembl gene ID recognized within FUMA were included in this analysis. Positional gene sets chr17q21, and chr6q16 were enriched for these non-specific nociplastic pain genes, as were several cancer gene neighborhoods (Supplementary Table 6) and 9 GWAS Catalog traits including migraine without aura, headache, and migraine (Supplementary Table 7, Figure 3C).
There was no overlap in gene sets enriched for specific and non-specific genes, and migraine and headache gene sets were enriched for non-specific nociplastic-type pain genes only.
Discussion
We carried out common-factor GWAS and TWAS analyses incorporating six COPCs, to investigate genetic variation associated with nociplastic type pain, a mechanistic pain descriptor and type of pain likely important across COPCs. We found that nociplastic type pain is a moderately heritable trait with similar liability-scale SNP heritability to rheumatoid arthritis. Our findings indicate that nociplastic type pain is a complex, polygenic trait, and we found 24 independent SNPs significantly associated with this trait.
Nociplastic type pain is genetically correlated with rheumatoid arthritis and MCP
We observed extremely high genetic correlation between nociplastic type pain and MCP (rg = 0.92). Individuals with a non-zero trait value for MCP could as a group be majority composed of individuals with COPCs – to assess this we carried out a series of Fisher’s exact tests on counts of COPC ICD10 code occurrences within and outside of MCP ‘cases’ (MCP trait value >=1) in UK Biobank (see Supplementary Table 8). We found that for ICD10 category codes for COPCs that were available in UK Biobank (back pain, post-viral fatigue (ME/CFS), migraine, IBS, endometriosis and tension headache), all were significantly overrepresented in MCP cases compared to those without chronic pain (MCP trait value 0). Additionally, the main characteristic of MCP (increasing number of sites of chronic pain) might sufficiently represent nociplastic type pain – a recent paper outlining clinical criteria in assessing and grading nociplastic pain lists regional (as opposed to discrete) location and spread of pain as a key indicator of possible nociplastic pain (49).
Traits enriched for specific and non-specific nociplastic-type pain genes indicate distinct pathology of migraine and headache
Gene set enrichment results showed certain genes significantly contribute to variation in nociplastic pain phenotype, but that a large amount of their influence on COPC traits is not mediated by nociplastic type pain (non-specific genes i.e., genes with significant heterogeneity in genomicSEM analyses). GWAS trait gene sets enriched for such genes included migraine and headache, suggesting involvement of factors outside of nociplastic pain in these traits. Non-nociplastic-type-pain-specific genes were also enriched in trait gene sets for male-pattern baldness (androgenic alopecia) – alopecia, including androgenic alopecia, has been previously associated with drugs that block CGRP (calcitonin gene related peptide), a treatment for acute migraine and migraine prevention (50).
Potential metabolic and liver related pathology in nociplastic pain
GWAS trait gene sets enriched for specific nociplastic type pain genes included amino acid and acylcarnitine levels. Changes in amino acid levels are associated with fibromyalgia, migraine, osteoarthritis and complex regional pain syndrome (51). High acylcarnitine levels can indicate disorders in fatty acid metabolism, and diets high in certain fatty acids have been associated with increased allodynia in rodent models, and associated with human chronic pain conditions (52). Lipids generally are also involved in acute and chronic inflammation (53) and changes to acylcarnitine metabolism are observed in dementia, certain cancers, heart failure and coronary artery disease (54). Changes to circulating lipids have also been observed in COPCs including fibromyalgia, headache, migraine, TMD, low back pain and IBS (55), and cholesterol metabolism in microglia has been linked to neuropathic pain in a rodent model (56). In addition, certain drug therapies used in treatment for systemic lupus erythematosus and rheumatoid arthritis can disrupt lipid metabolism (57), and experiencing chronic pain is associated with changes in diet that can result in changes in lipid profiles (58).
Genes specifically upregulated in liver tissue were also enriched for specific nociplastic type pain genes. This could be indicative of liver damage as long-term use of NSAIDs as is common in chronic pain conditions including COPCs. While serious liver injury in NSAID use is rare, NSAIDs are one of the main causes of acute hepatitis globally, and there is some evidence that serum aminotransferase levels (where elevated levels can indicate liver disease or dysfunction) are transiently elevated without other symptoms with NSAID use (59,60).
Curcuminoids (components of turmeric) have been previously investigated in treatment of neuropathic pain, and previous studies found that a possible mechanism of action in alleviating neuropathic pain was via modulating nitrogen metabolism (61). Although ME/CFS summary statistics were not used in this analysis, changes in nitrogen metabolism have been implicated in this condition (62), and our findings suggest these metabolic changes may not be unique to ME/CFS but instead shared across COPCs through influence on nociplastic pain in particular. Those with ME/CFS have also been found to have altered lipid, acylcarnitine, and amino acid levels compared to non-ME/CFS controls (63).
Positional gene sets enriched for nociplastic type pain genes suggest immune and musculoskeletal factors
Positional gene sets associated with specific nociplastic pain genes have also been previously linked to COVID-19 susceptibility and severity (chr3p21, (64)), schizophrenia and bipolar disorder (chr3p21, (65)), and Alzheimer disease in an African American cohort (chr3p21, (66)). Regions in chr9q33 are frequently deleted in certain cancers (67,68), and chr16q22 has been previously associated with a rare duplication syndrome accompanied by varying psychiatric disorder symptoms (69), and with schizophrenia (70). A type of syndactyly (involving fusion of digits and toes) has been associated with chr2q34 (71), along with autoimmunity, amyotrophic lateral sclerosis and schizophrenia (72), and age-related degeneration in the lumbar spine (73). Variants in the chr12q13 region have been associated with childhood obesity (74) and asthma (75,76). Finally, chr1q21 has been previously implicated in GWAS of circulating IL6 levels (77). These findings suggest shared immune and musculoskeletal related etiology in these phenotypes and nociplastic type pain.
In contrast, positional gene sets enriched for non-specific nociplastic pain genes included chr17q21, where duplication and deletion have previously been associated with syndromes involving distinctive craniofacial features, developmental delay, and cardiac symptoms (OMIM 610443, 613533), and genes at chr6q16 with cardiac phenotypes (78) and cluster headache and migraine (79).
Tissue enrichment of nociplastic type pain genes highlights thyroid, heart, and tibial nerve involvement
Hypothyroidism can both cause pain and worsen pain experienced as part of comorbid chronic pain conditions. Autoimmune disorders including autoimmune hypothyroidism may also be misdiagnosed as fibromyalgia (80–82). Enrichment of nociplastic type pain gene associations here may therefore indicate high levels of thyroid involvement in COPCs, or extensive presence of individuals with comorbid (or misdiagnosed) hypothyroidism among COPC GWAS participants, or both.
Atrial appendages of the heart (left and right) are small pouches located on the front upper surface of the right atrium, and anterior to the left atrium and parallel to the left pulmonary veins. Atrial fibrillation, the most common abnormal heart rhythm in adults, can lead to formation of clots (most commonly in the left atrial appendage) and subsequent stroke (83–85). ECG abnormalities, particularly atrial fibrillation, have been linked to chronic pain (86,87), and with physiological stress associated with chronic illness and major surgery (88,89). Chronic pain has also been associated with higher risk of myocardial infarction, death due to cardiovascular event, heart failure, and stroke (90). Our findings may suggest this atrial fibrillation in particular is common in nociplastic pain and COPCs, increasing risk for stroke in these patient populations.
The tibial nerve is one of two terminal branches of the sciatic nerve, providing motor and sensory innervation to almost all of the posterior foot and leg. An ultrasound study comparing participants with fibromyalgia and controls found significant increased cross-sectional area in several nerves, including tibial nerve (91). Tarsal tunnel syndrome, a nerve entrapment syndrome analogous to carpal tunnel syndrome in the wrist, was also found to be more common in fibromyalgia patients (92) – while causes of tarsal tunnel syndrome are likely multifactorial, enlarged tibial nerve diameter may contribute to this nerve entrapment. Neuromodulation involving the tibial nerve (e.g., through percutaneous tibial nerve stimulation) has also been investigated in the treatment of a range of pelvic pain disorders, including IBS, dysmenorrhea, and bladder pain syndrome (93). One caveat is that tibial nerve is the only peripheral nerve tissue sampled in GTEx – other peripheral nerve tissues, potentially also representing therapeutic targets in neuromodulation for chronic pain, could potentially be enriched for nociplastic pain gene expression.
Conclusions
COPCs are a subset of chronic pain conditions that are commonly comorbid and more prevalent in women and AFAB individuals. A third mechanistic pain descriptor, nociplastic pain, may represent the pain experience of those with COPCs, where tissue and/or nerve damage is often not present. Using existing COPC GWAS data and a network-informed genomics approach, GenomicSEM, we found genetic variation at the SNP, gene expression, and gene-set level associated with nociplastic type pain. We also explored genetic overlap with other chronic pain phenotypes, tissue enrichment of nociplastic pain genes, and differences in genes specific and non-specific to nociplastic-type pain. Our findings indicate distinct pathology in migraine and headache compared to other COPCs, and link this distinct pathology with traits such as Parkison disease, sense of smell, and androgenic alopecia, as well as providing unique genes associated with this distinct pathology. We also find tissue enrichment relevant to chronic pain comorbidities including stroke, and therapies such as peripheral nerve stimulation. Our findings contribute to further understanding mechanisms of nociplastic type pain, and indicate this type of pain is important across COPCs.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
References
- 1.↵
- 2.↵
- 3.
- 4.↵
- 5.↵
- 6.
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.
- 23.
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.
- 82.↵
- 83.↵
- 84.
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵




{kind=link}
{kind=link}
{kind=link}